Download to read offline






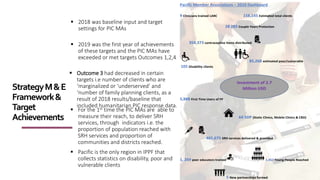
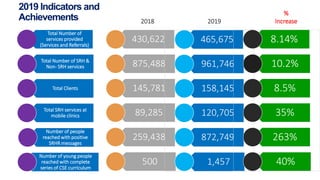
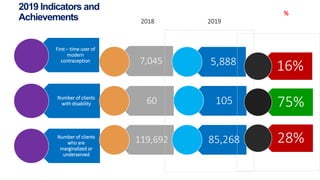




The Niu Vaka Pacific Strategy aims to improve sexual and reproductive health and rights (SRHR) in the Pacific region over the next 5 years. It will provide targeted support to Pacific Member Associations of the International Planned Parenthood Federation, including Papua New Guinea, to improve sustainability, expand reach, build an enabling environment for SRHR, and streamline reporting. The strategy establishes clear targets and emphasizes capacity building, partnerships, and flexibility for Member Associations. Initial results under the strategy have been positive, with Member Associations exceeding or meeting targets in several areas due to increased autonomy, faster implementation, and improved data systems.






















































































