This document discusses various types of birth injuries including:
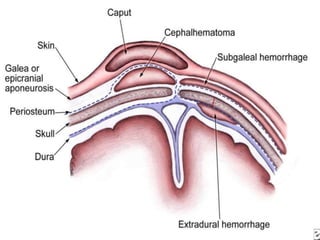
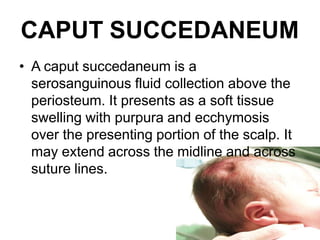
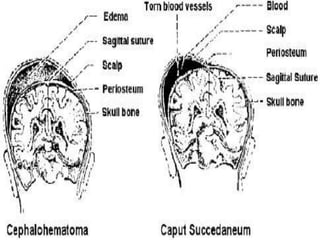
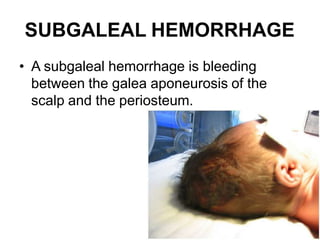
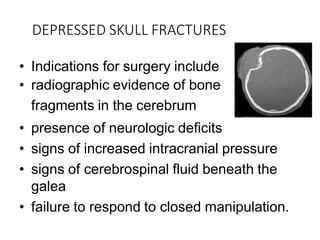
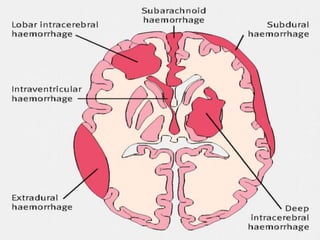
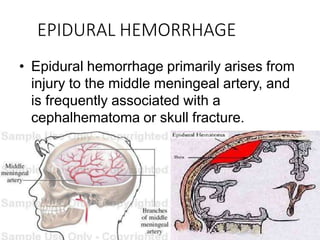
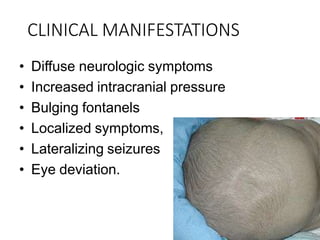
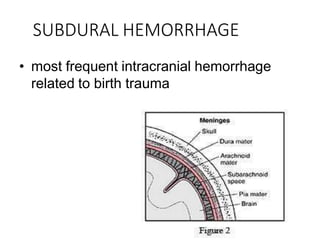
- Head and neck injuries such as caput succedaneum, cephalhematoma, subgaleal hemorrhage, skull fractures, and intracranial hemorrhages.
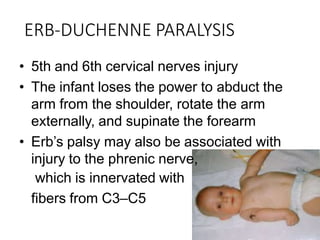
- Nerve injuries including brachial plexus injuries (Erb's palsy and Klumpke's palsy) and facial nerve palsy.
- Risk factors for birth injuries include prolonged or difficult labor, fetal macrosomia, and instrument-assisted delivery. Birth injuries can cause impairments ranging from mild swelling to life-threatening hemorrhages requiring medical or surgical intervention.












































![Fetal birth-injuries[1]](https://cdn.slidesharecdn.com/ss_thumbnails/fetal-birth-injuries1-121204143707-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





































