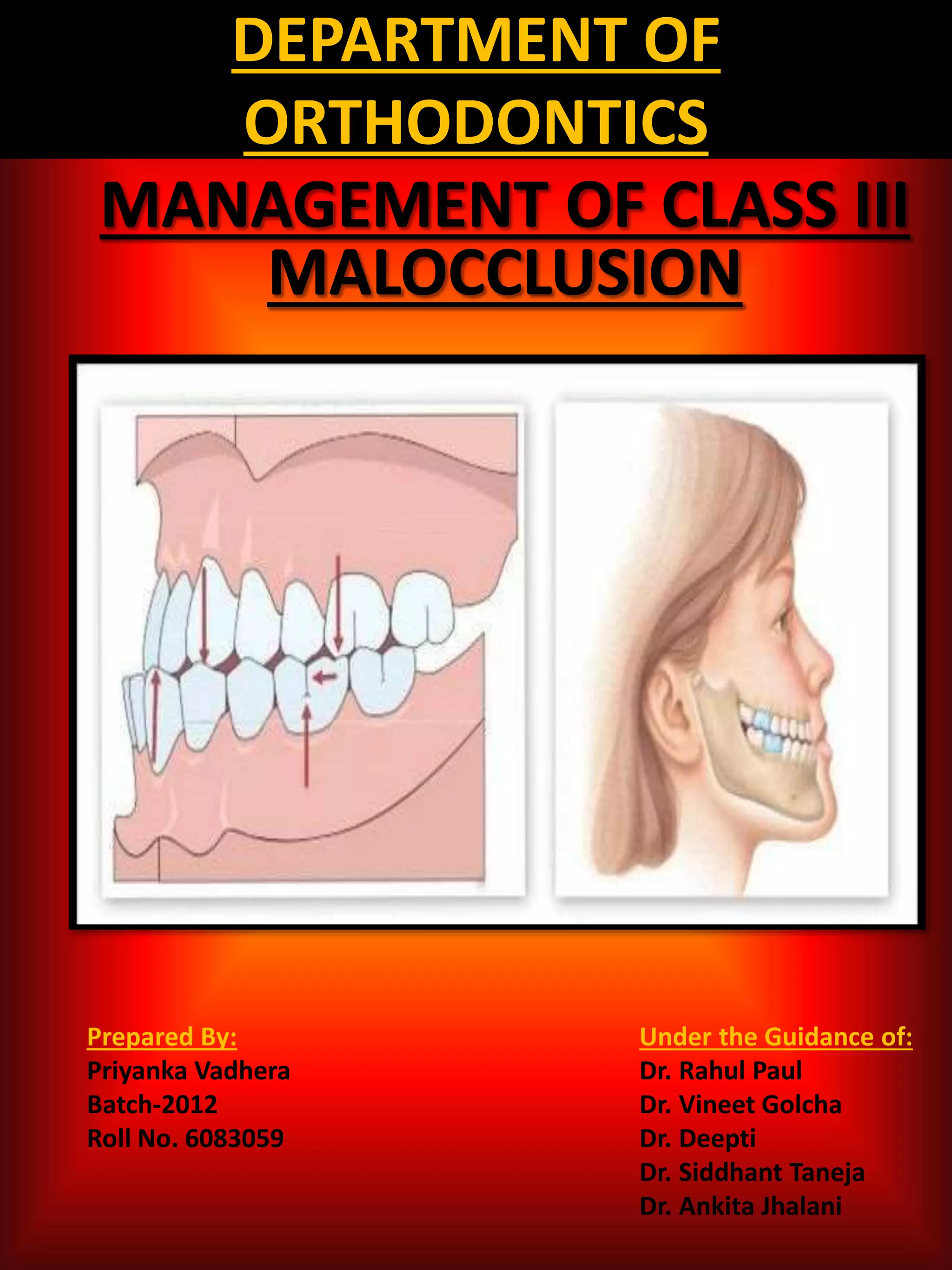
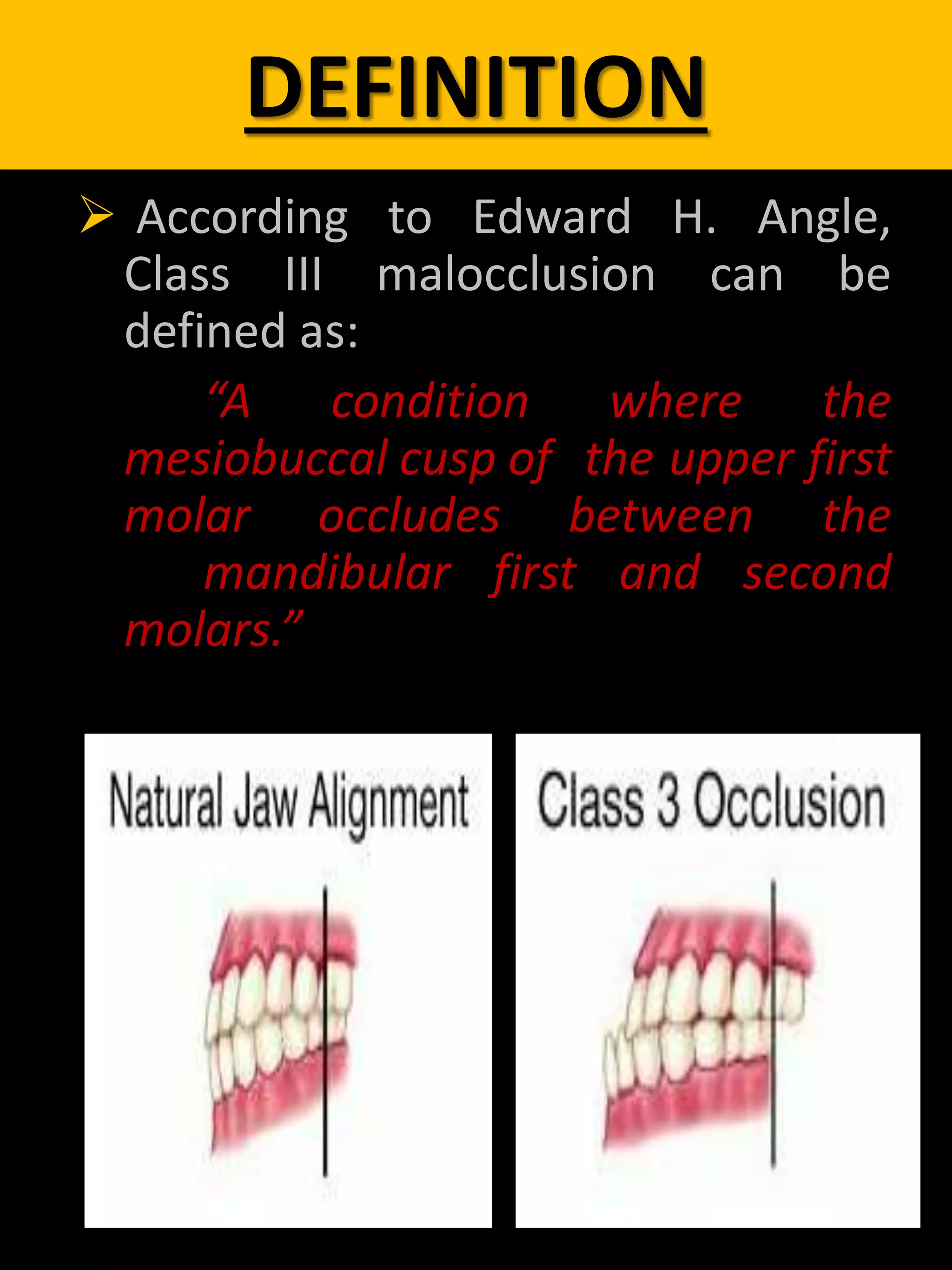
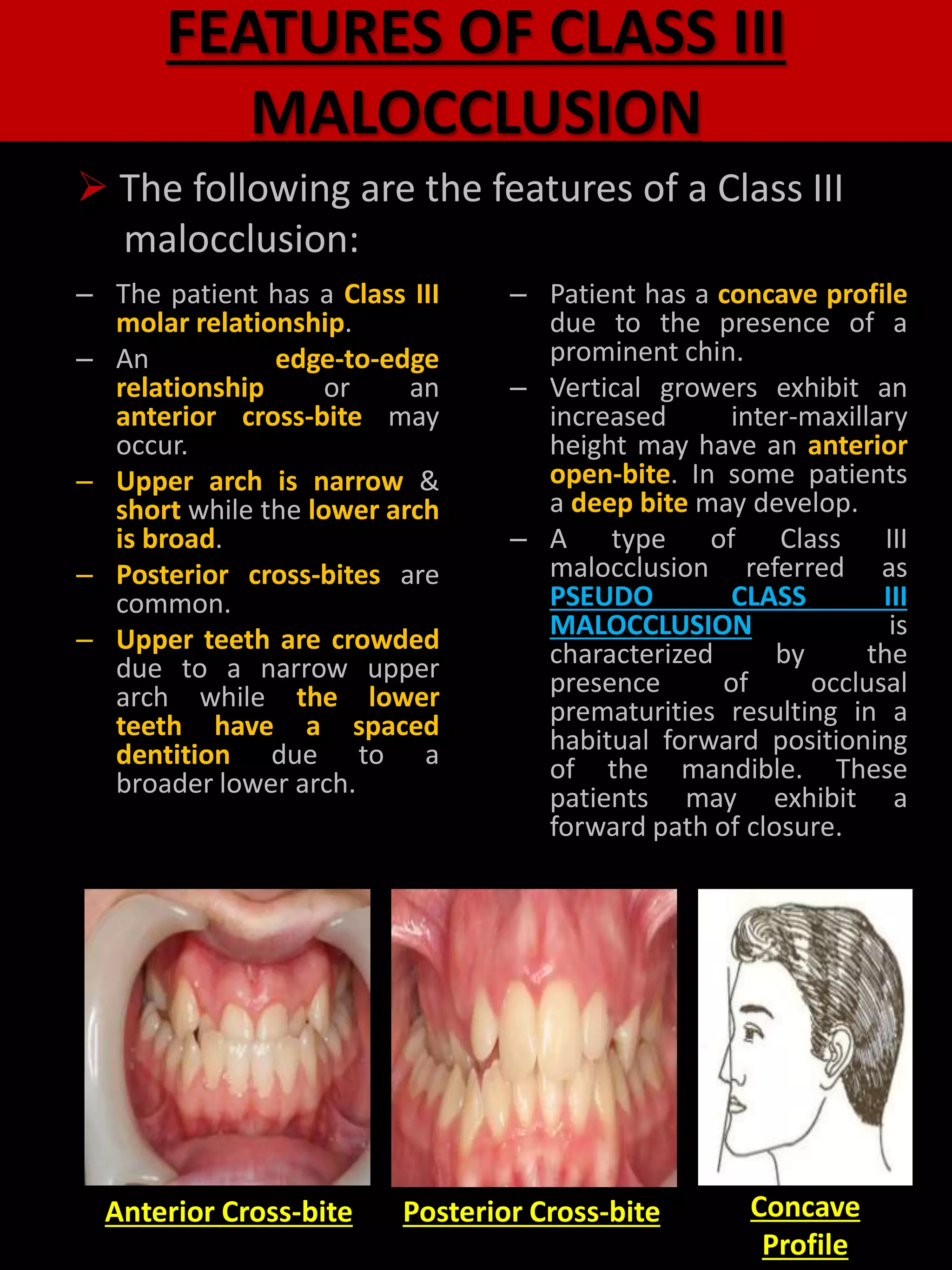
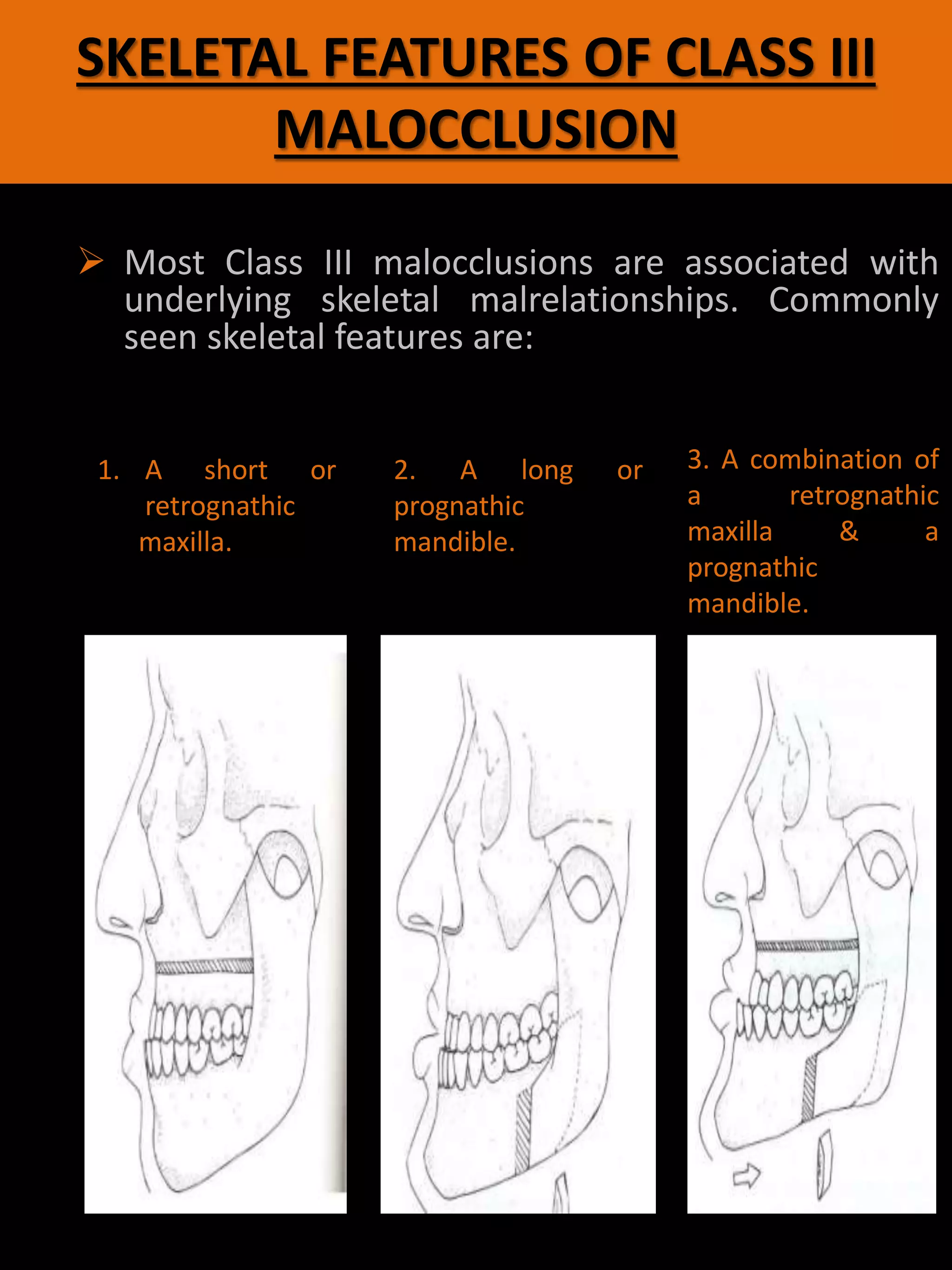
This document discusses the diagnosis and treatment of Class III malocclusions. It begins with definitions and features of Class III malocclusions, noting they involve a mesial relationship of the mandible to the maxilla. Treatment approaches are described for:
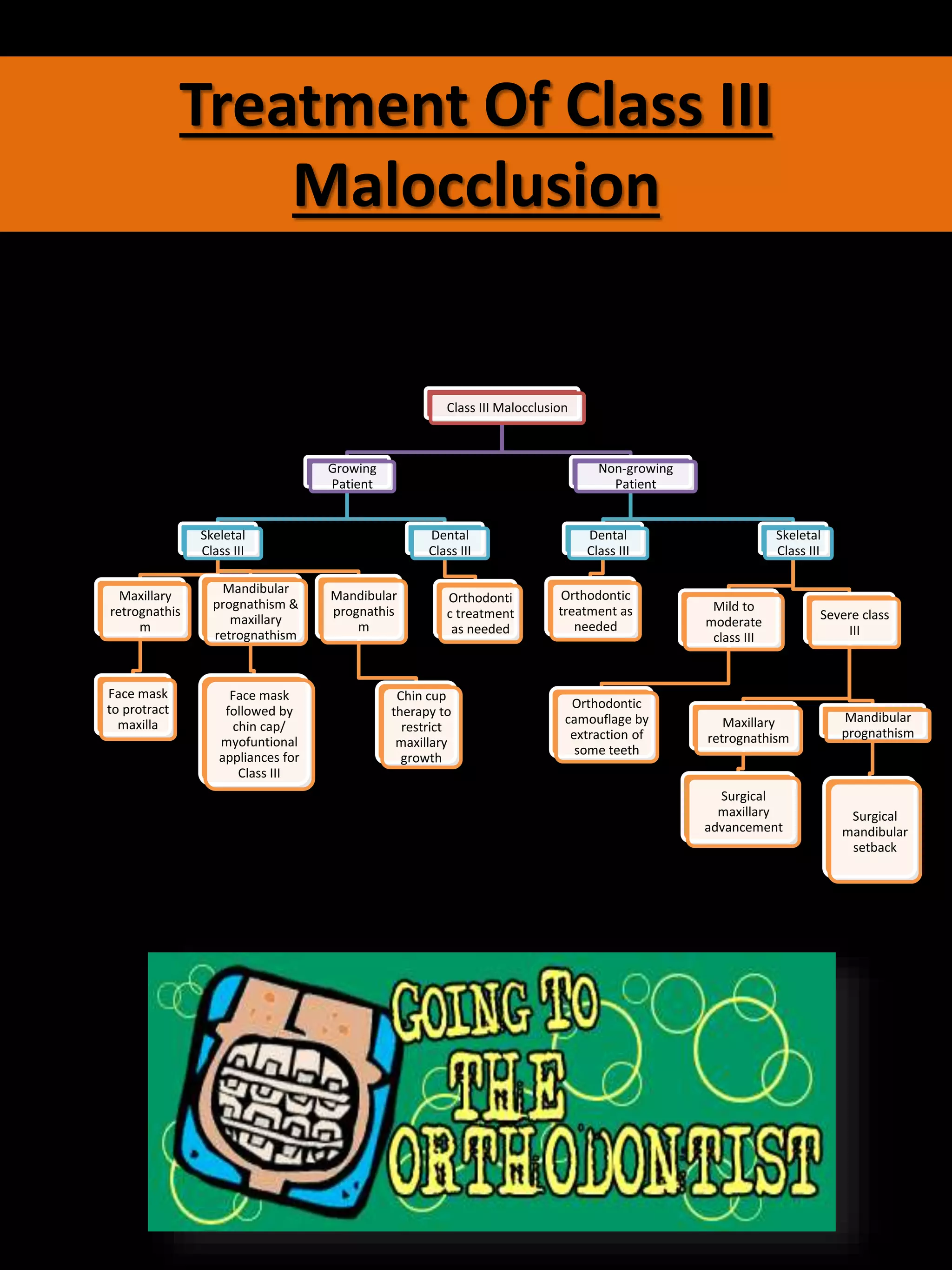
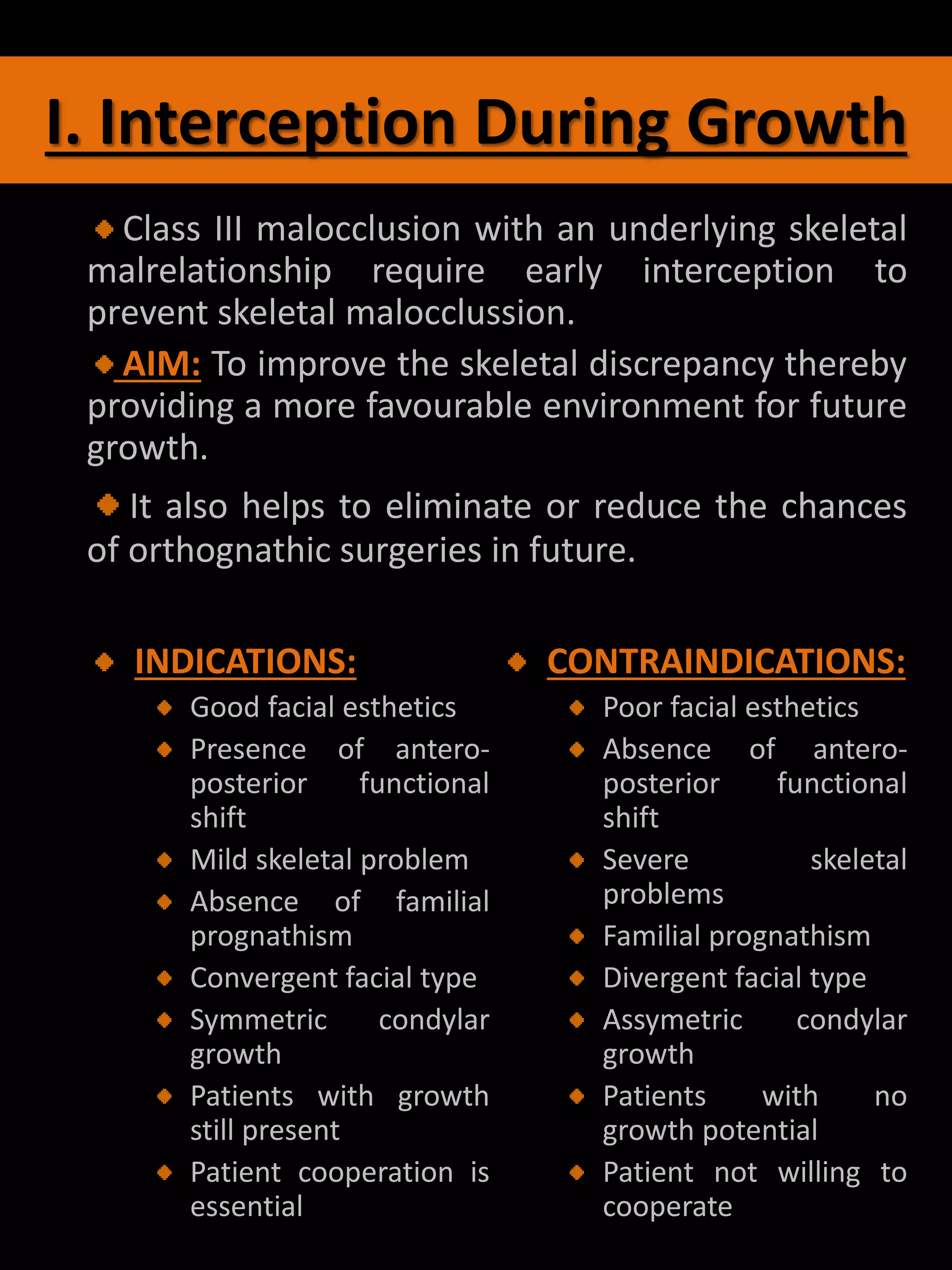
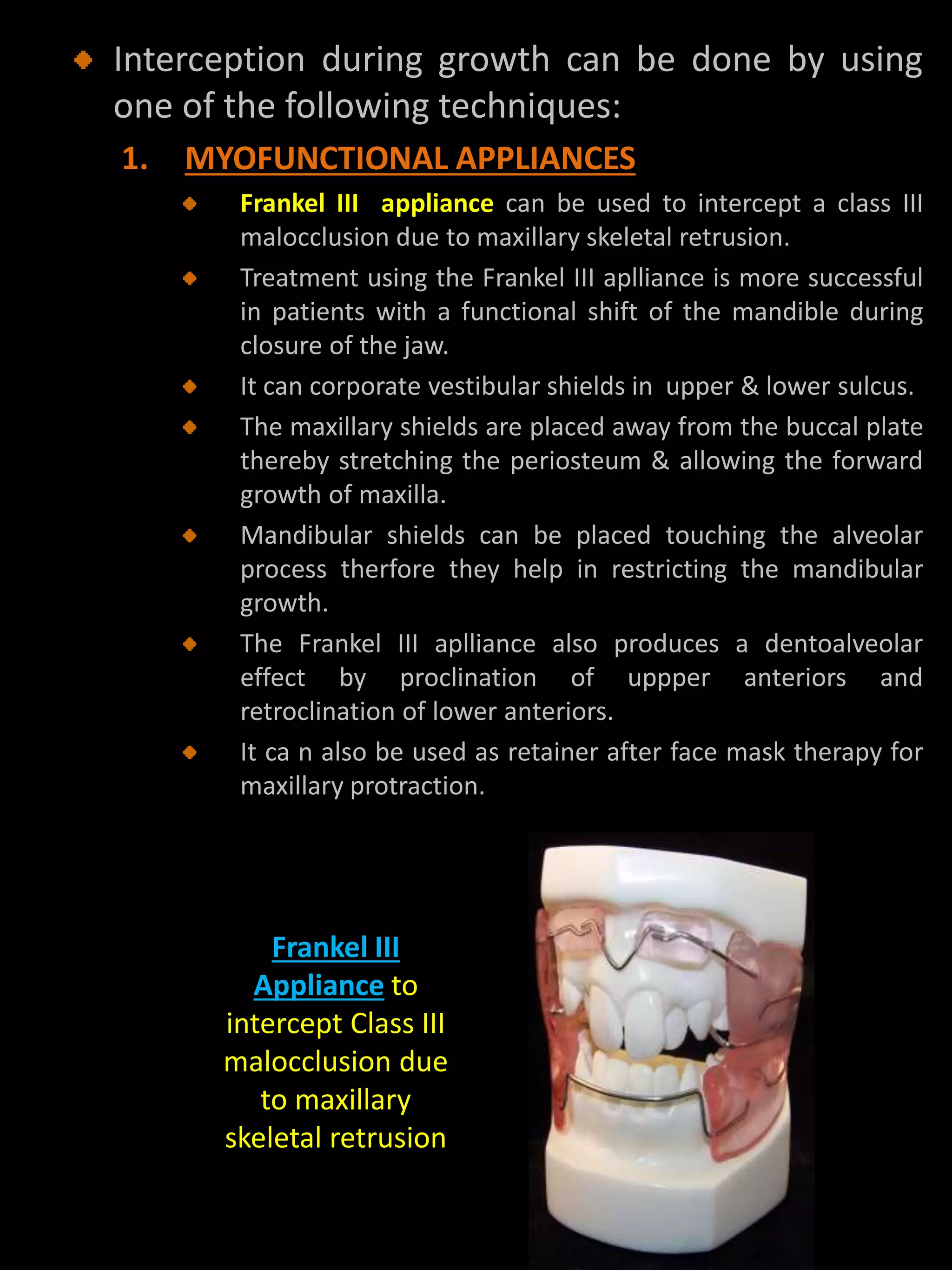
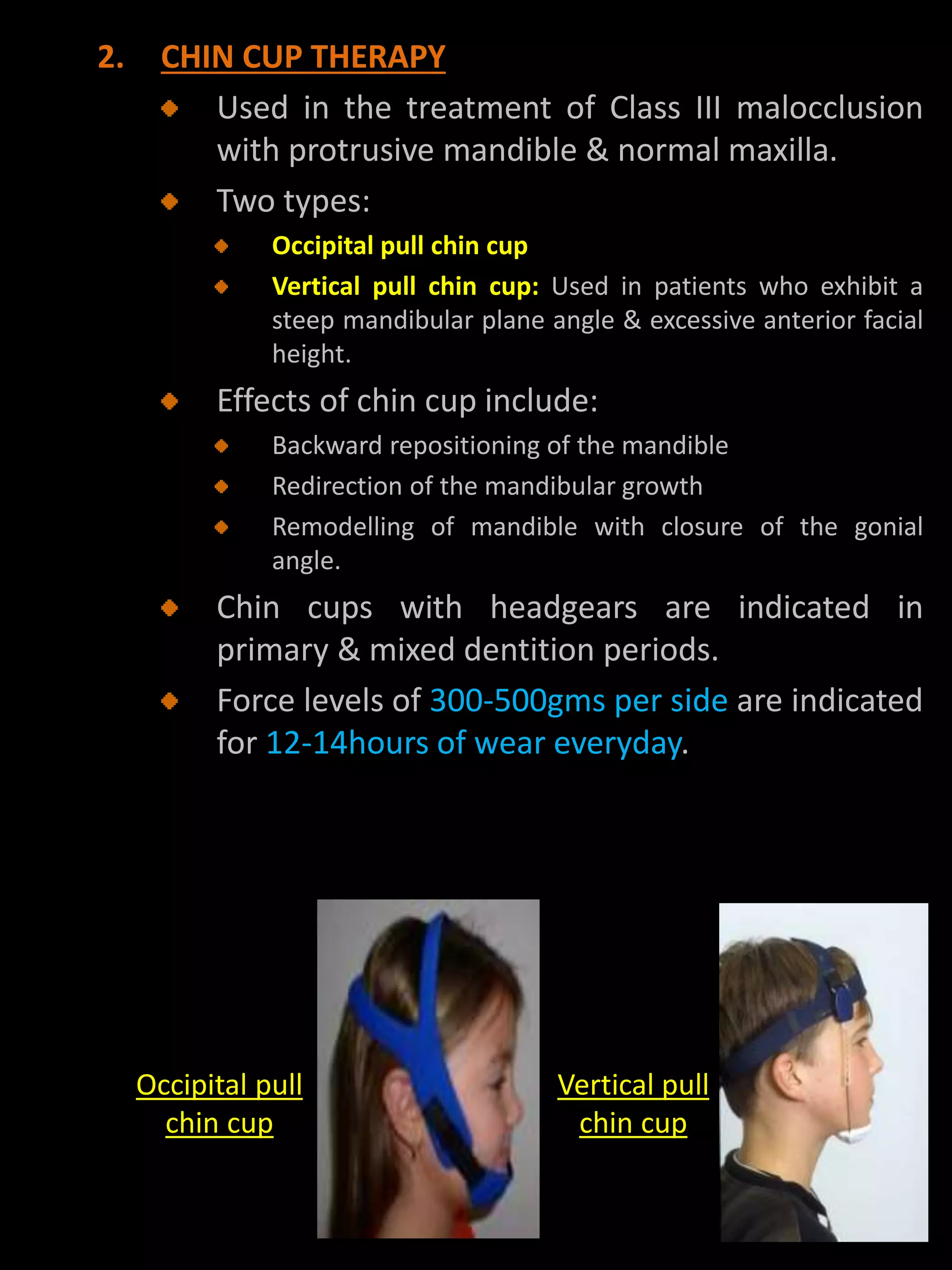
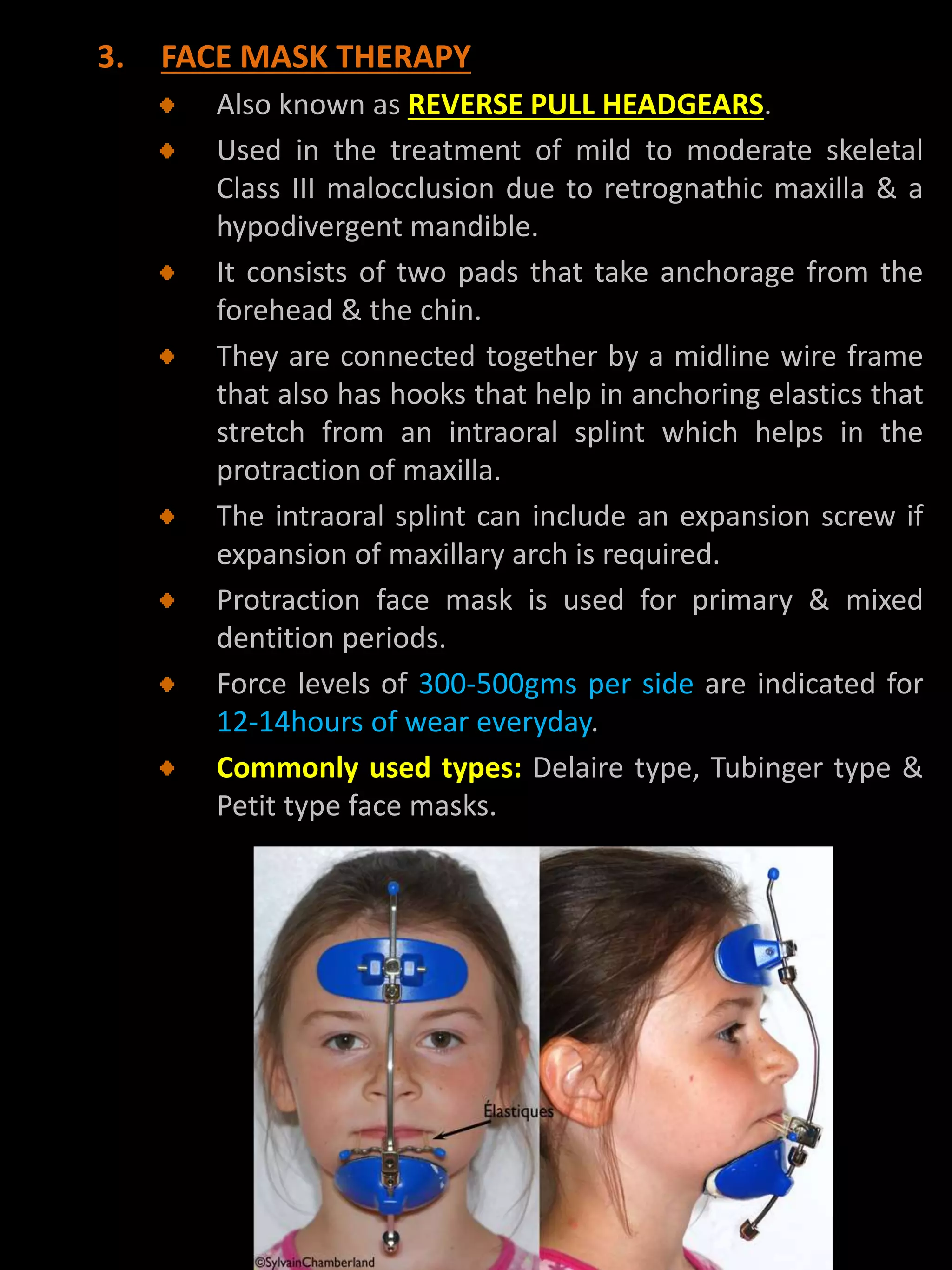
1. Intercepting Class III malocclusions during growth using myofunctional appliances, chin cups, or face masks to redirect growth.
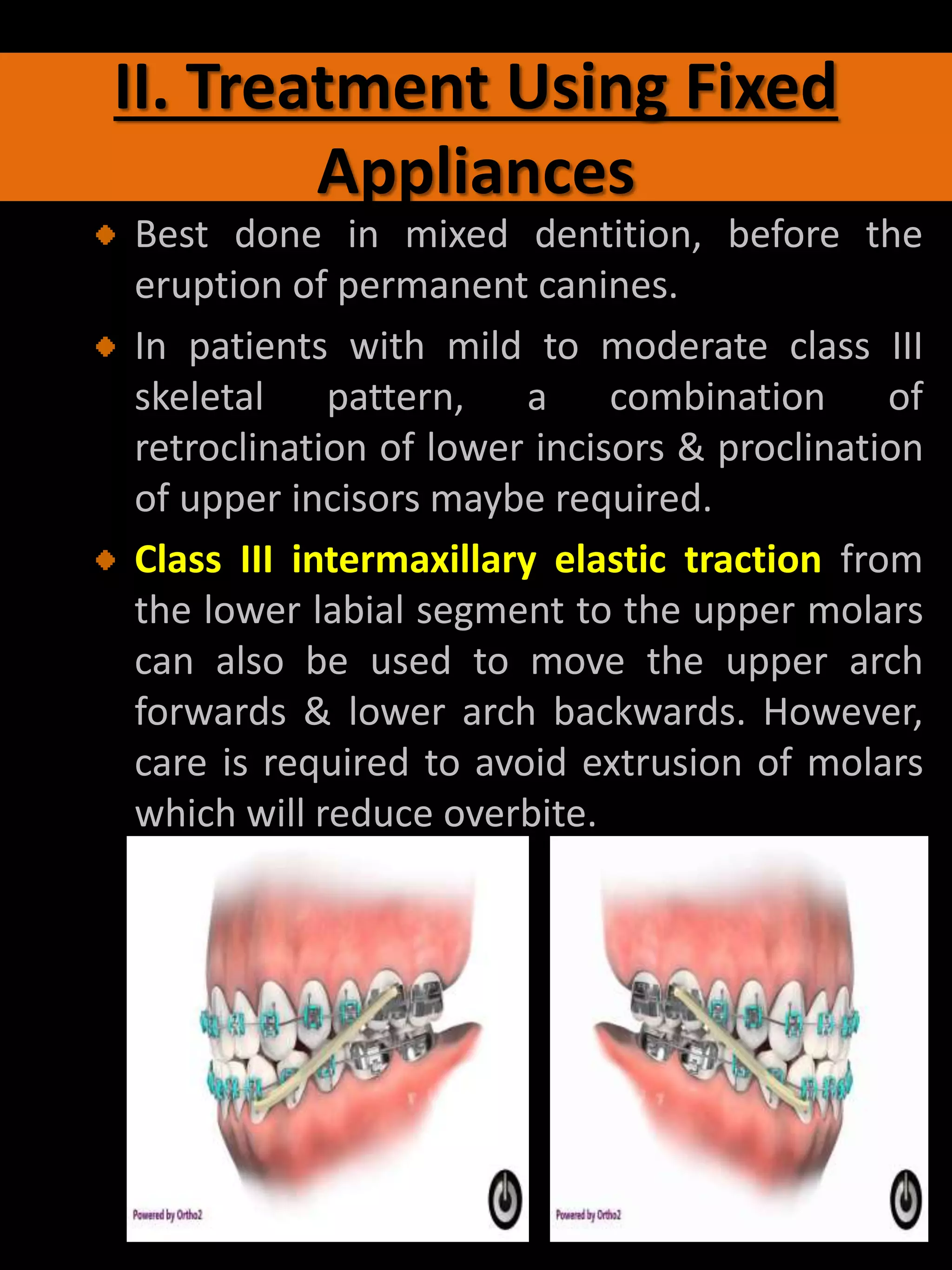
2. Using fixed appliances in mixed dentition to retrocline lower incisors and procline upper incisors.
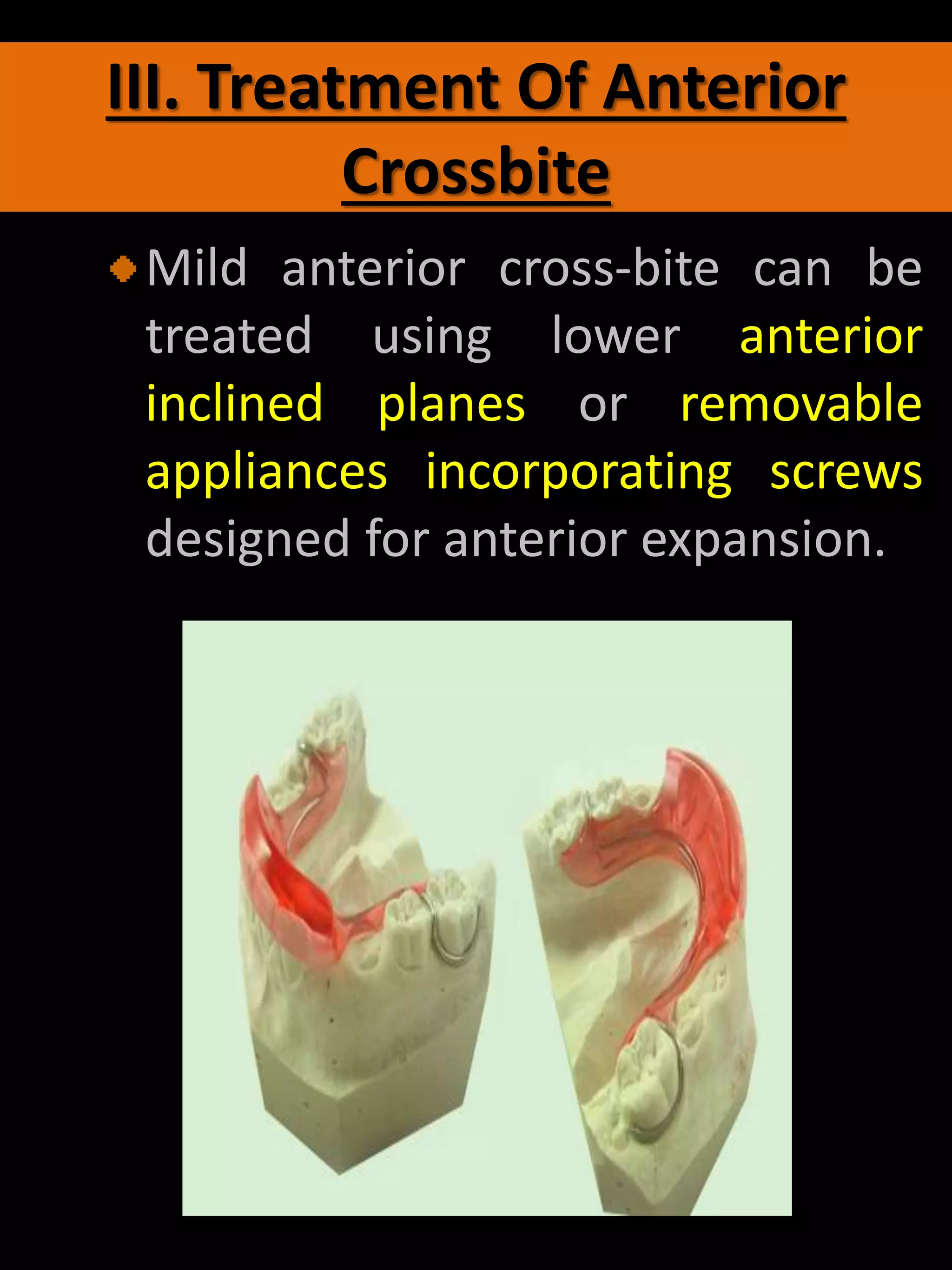
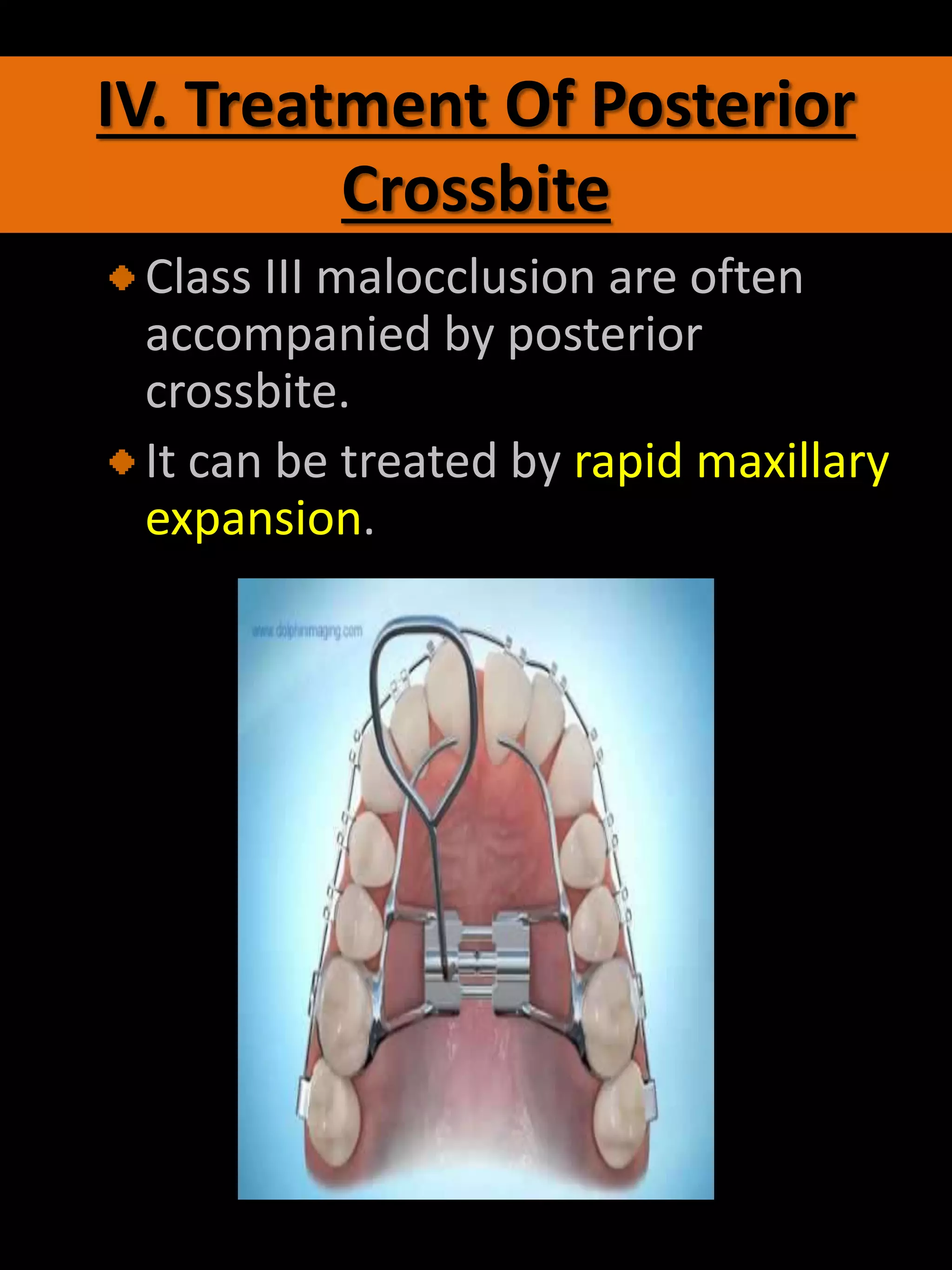
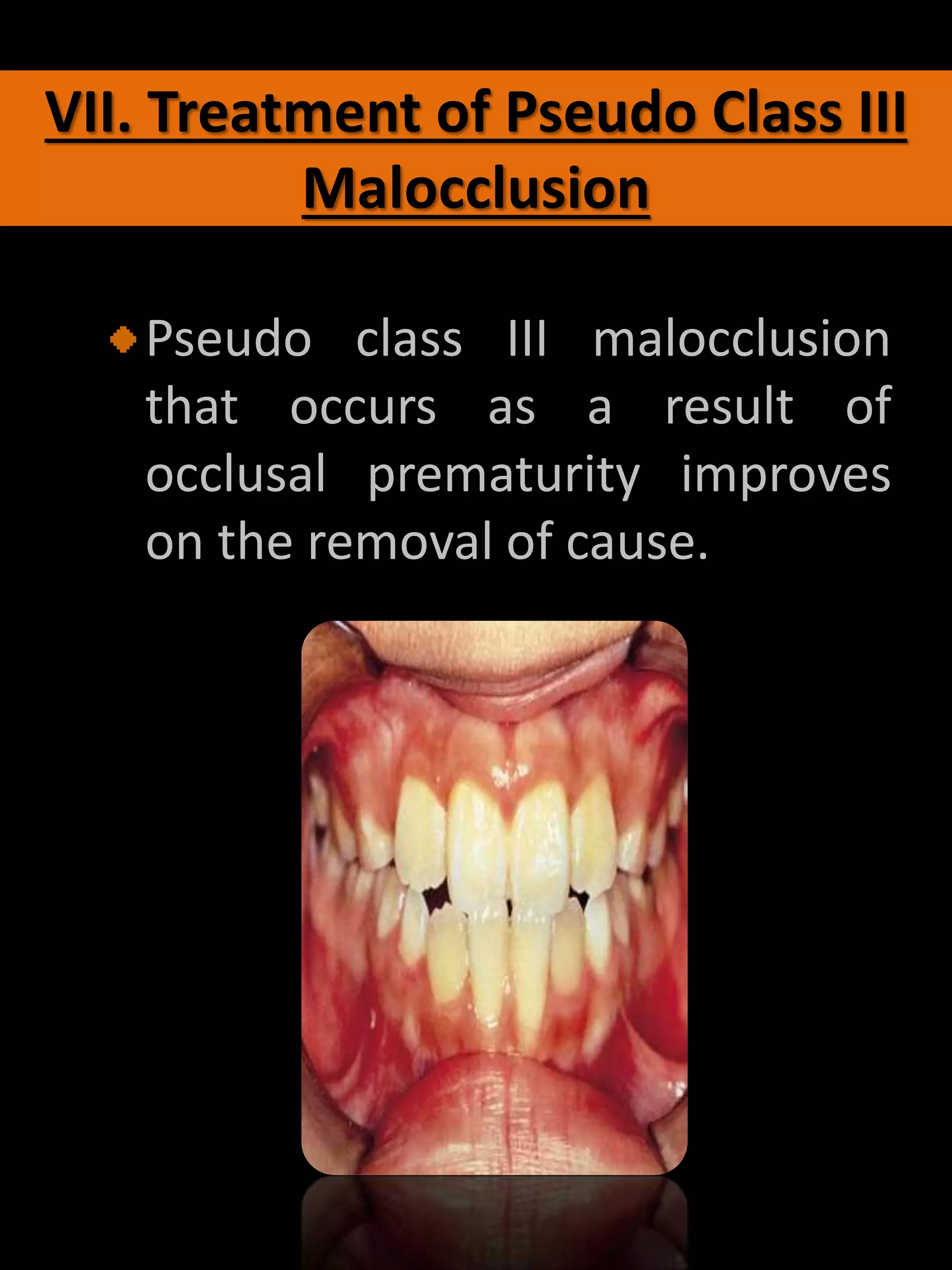
3. Addressing anterior and posterior crossbites.
4. Considering extractions for mild mandibular prognathism.
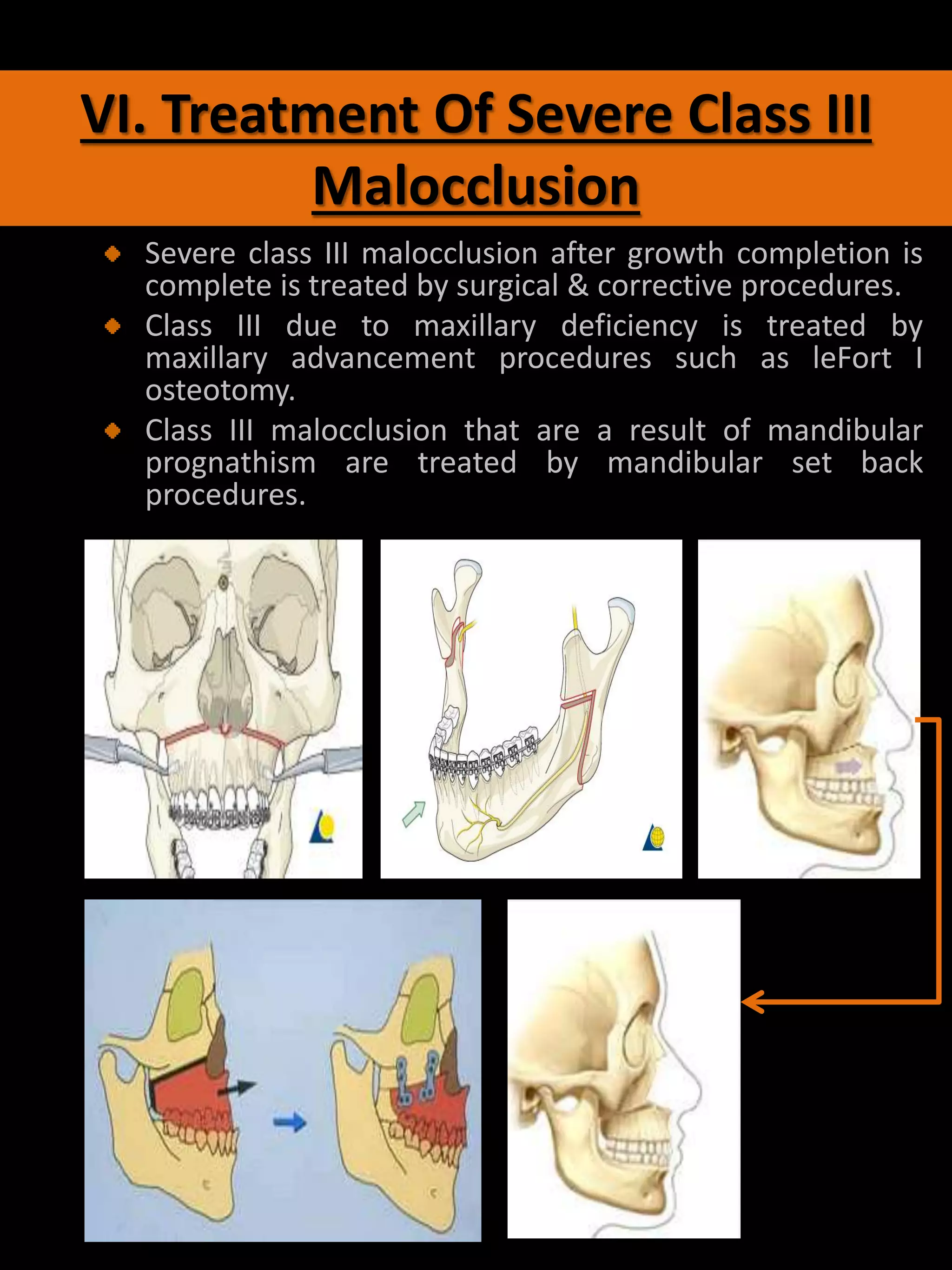
5. Surgical-orthodontic treatment