
Downloaded 136 times













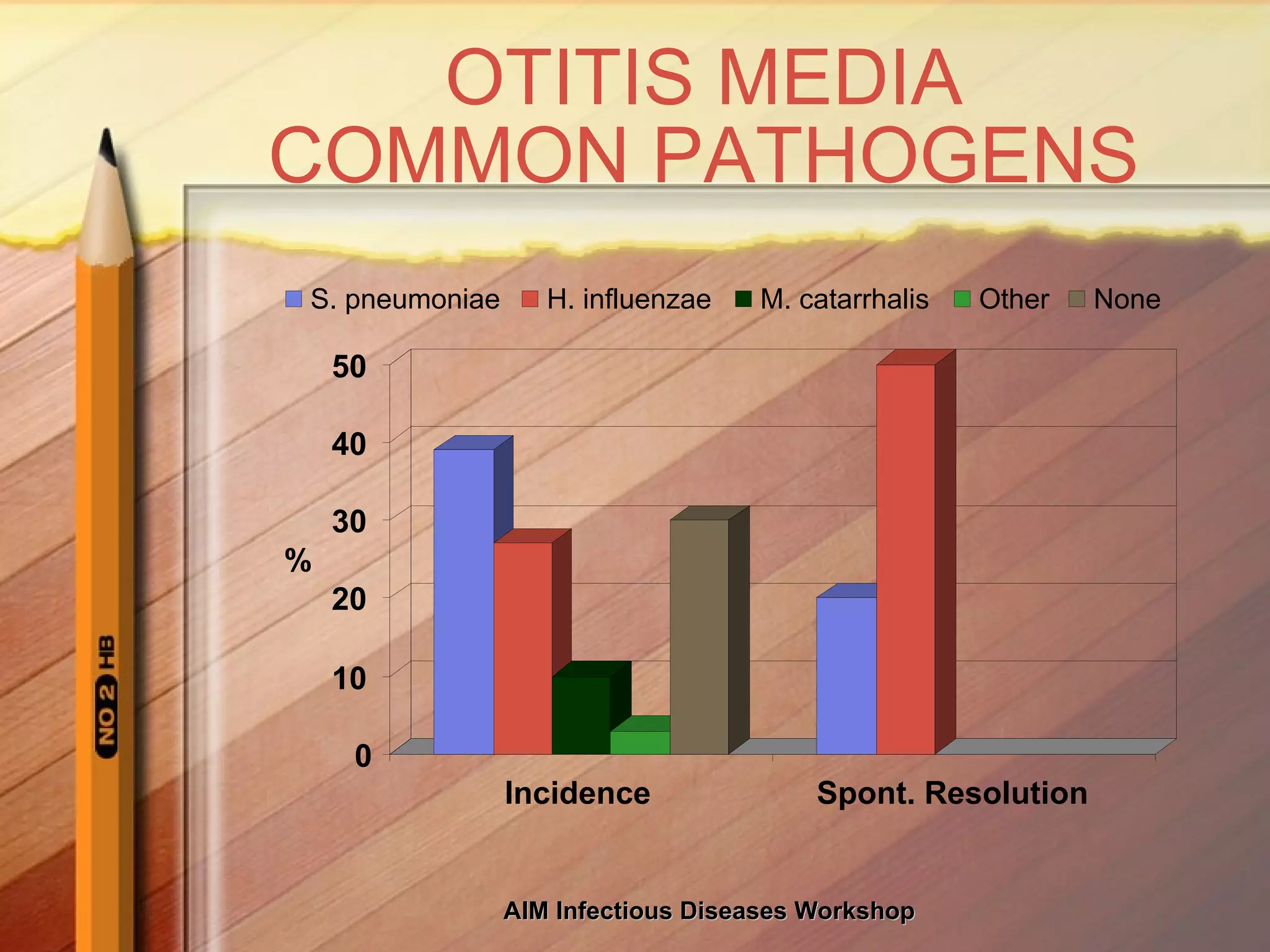






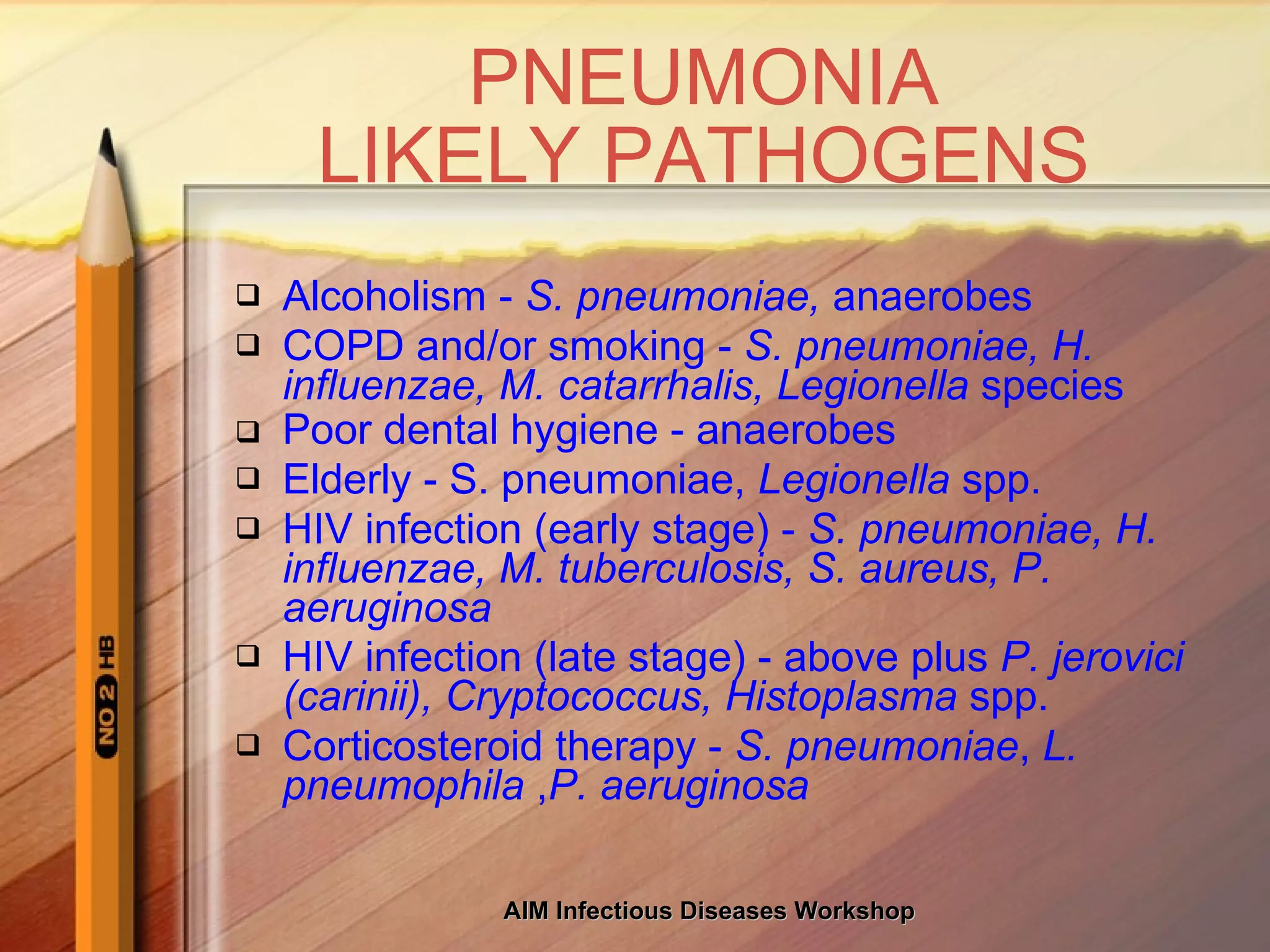
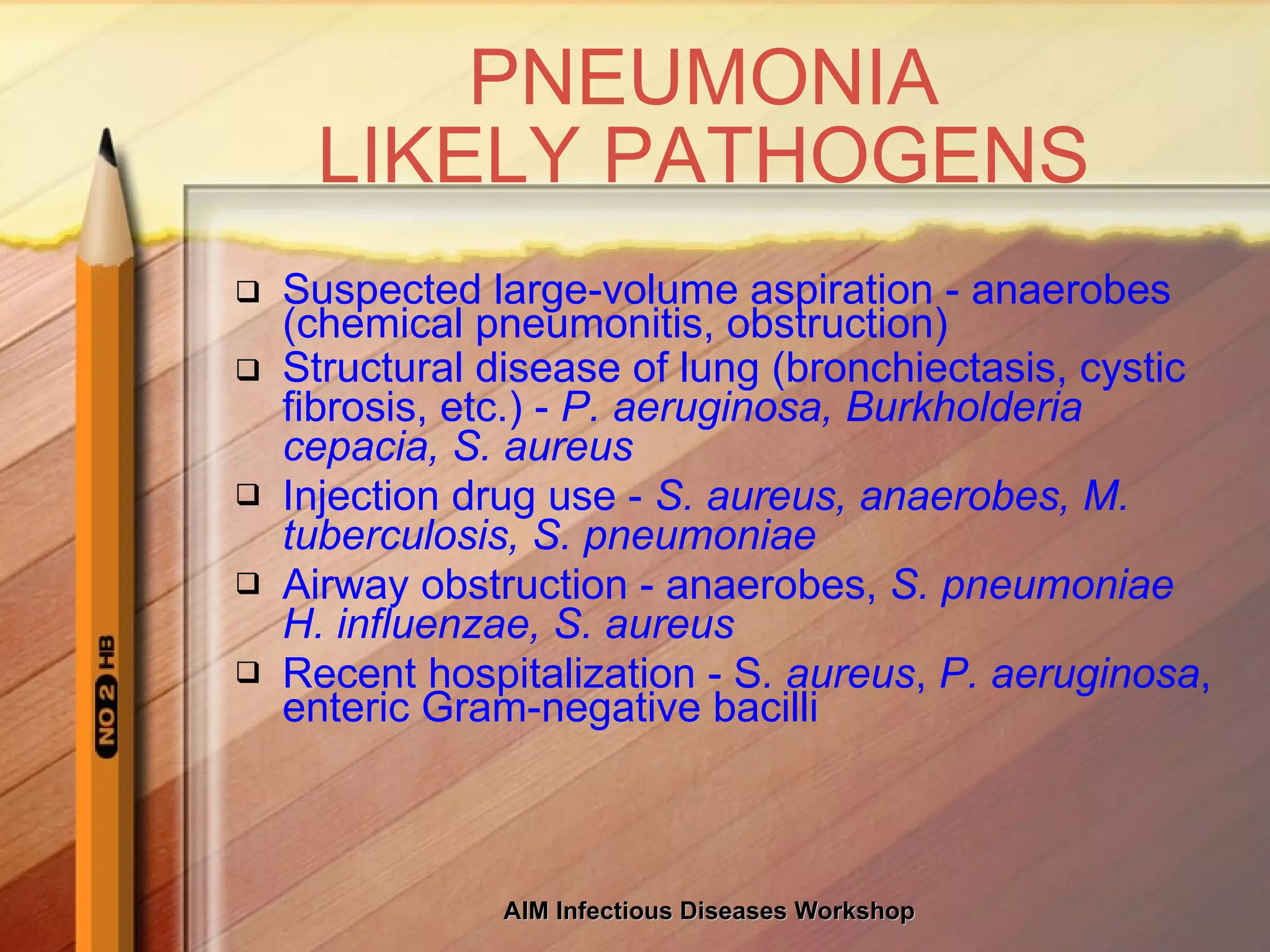



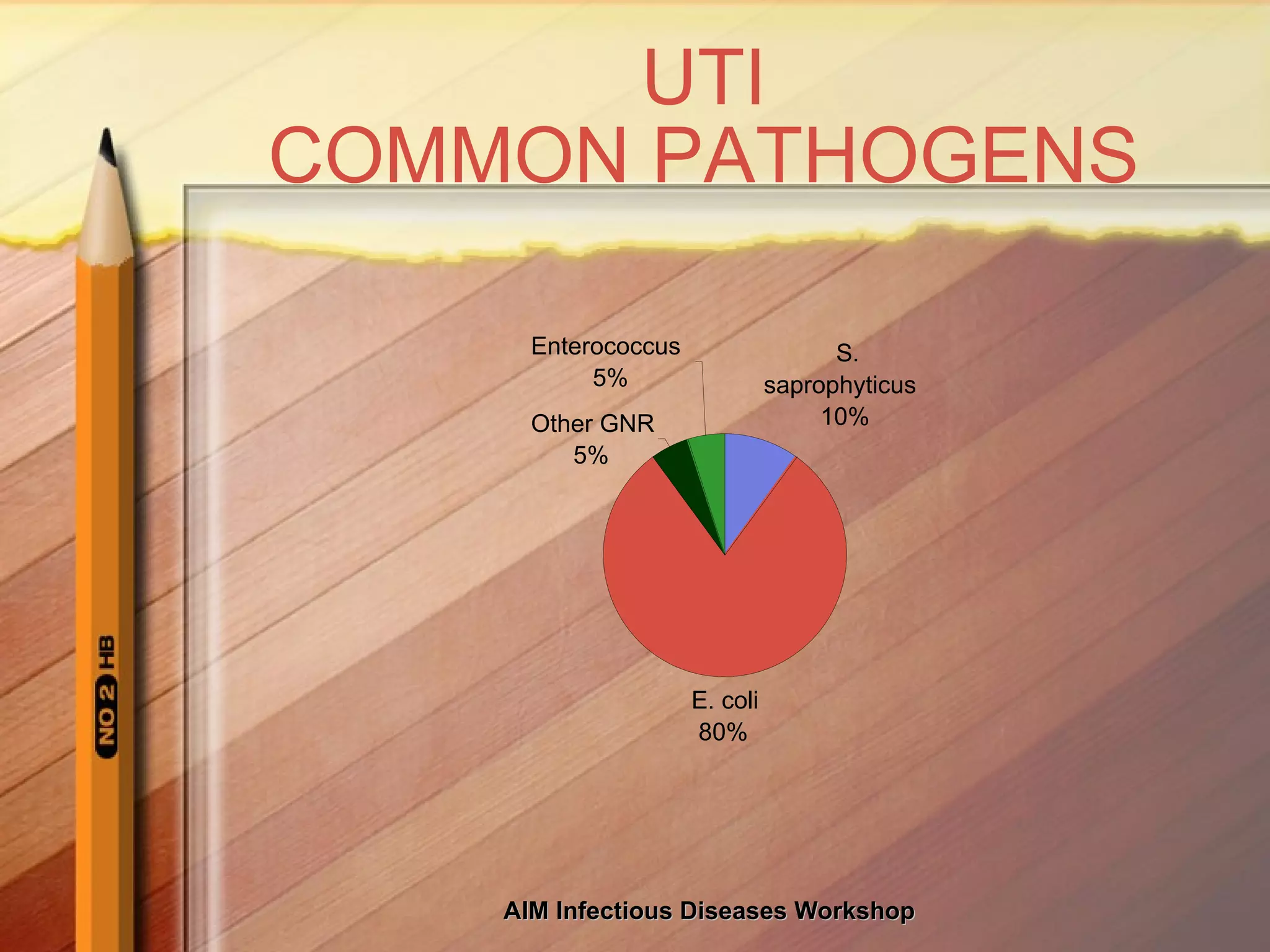
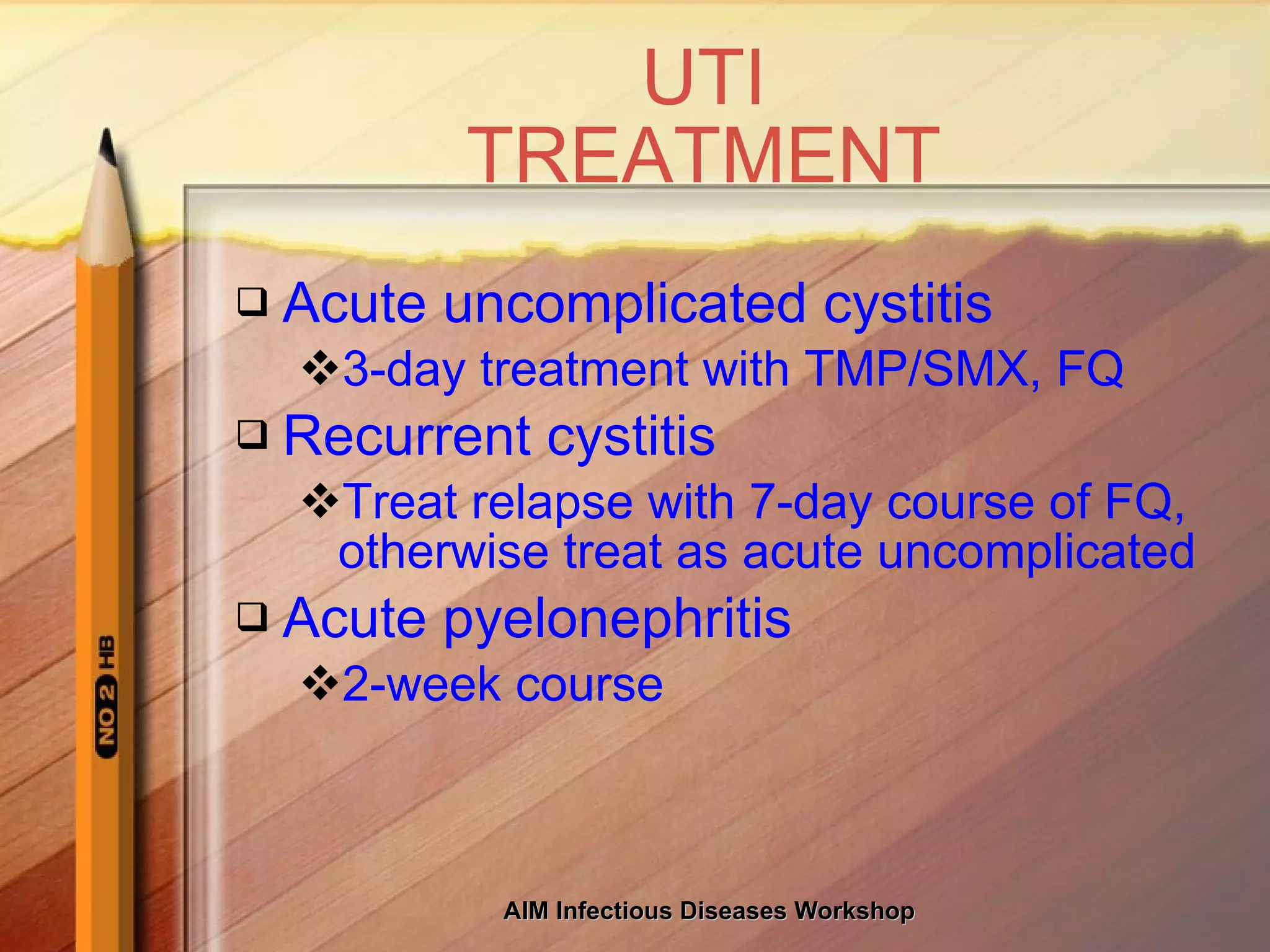















This document discusses the judicious use of antibiotics and increasing antibiotic resistance. It provides information on common infectious disease syndromes, likely pathogens, and antibiotic treatment options. It emphasizes using narrow-spectrum antibiotics when possible, older agents when feasible, and combination therapy only when necessary to help reduce antibiotic overuse and resistance.


















































































