1. 274
INTRODUCTION
Dry eye syndrome (DES) is characterized by ocular irritation and visual
disturbance resulting from alterations of the tear film and ocular
surface.1–10
The effects of DES can vary from minor inconvenience to
rare sight-threatening complications. Although the diagnosis of DES
has traditionally focused on inadequate secretion or aqueous tear defi-
ciency, the tear film is a complex and delicately balanced unit depend-
ent on the normal function of several distinct components.10–13
Current
treatment is heavily weighted toward supplementation, stimulation, or
preservation of aqueous tears, which is satisfactory for many patients.
DES, however, often involves multiple deficiency states that, when
disregarded, can result in treatment failure and frustration for both the
patient and the physician. Currently, a large unmet need exists for bet-
ter treatment options for patients with DES.
EPIDEMIOLOGY
Estimating the prevalence of dry eye syndrome is complicated by the
absence of consensus on a single reliable diagnostic test. Several
population-based epidemiologic studies have utilized questionnaires to
assess prevalence of dry eye symptoms. American and Australian stud-
ies have revealed a prevalence of 5–16%, while Asian studies have
revealed a higher prevalence of approximately 27–33%.14–25
PATHOGENESIS
Normal Physiology
The stratified tear film is composed of mucin, aqueous, and lipid com-
ponents. The mucin layer consists of high-molecular-weight glycopro-
teins closely adherent to an inherently hydrophobic surface epithelium
and its glycocalyx. Mucin provides a smooth, hydrophilic surface per-
mitting even distribution of the overlying aqueous layer. Its primary
source is conjunctival goblet cells with a small contribution from sur-
face epithelial cells.26,27
Comprising the largest volume of the tear film,
the aqueous is secreted by the main lacrimal gland, the accessory
glands of Krause and Wolfring, and, minimally, a transudate of the
conjunctival vessels and cornea. Consisting primarily of water, it also
contains electrolytes (Na, K, Cl) and proteins, including epidermal
growth factor, immunoglobulins (IgA, IgG, IgM), lactoferrin, lysozyme,
and other cytokines.28,29
These components likely play both a protective
and a homeostatic role for the ocular surface. Lastly, meibomian
glands secrete a lipid layer, containing chiefly sterol esters and wax
monoesters.3,30
Although only 0.1 μm thick, the lipid layer serves to
stabilize the tear film by increasing surface tension and retarding
evaporation.
The tear layer maintains a smooth surface for optical clarity, lubri-
cates to facilitate eyelid blink, and offers protection against ocular infec-
tion.11
Average tear flow is about 1.2 μm/minute.31
Blinking serves to
periodically distribute tears evenly over the ocular surface and encour-
ages both secretion and mechanical drainage of tears through the lac-
rimal drainage system. Regulation likely involves both neuronal and
hormonal pathways. Direct innervation of the lacrimal gland, meibo-
mian glands, and goblet cells has been demonstrated, with M3 class
cholinergic receptors predominating in the lacrimal gland.32
While
estrogen has little effect on tear secretion, it may have a supportive role
on the ocular surface.33
Androgens appear to have a positive effect on
the secretion of both aqueous and lipid tears.34,35
Pathophysiology
Reduced aqueous tear flow and increased evaporation of the aqueous
component of tears leads to hyperosmolarity. Tear hyperosmolarity
damages the ocular surface epithelium and sets off a cascade of inflam-
matory pathways which leads to apoptotic cell death, loss of goblet
cells, and deficient mucus production, with resultant tear film instabil-
ity. Tear film instability, in turn, leads to increased evaporation. Impli-
cated cytokines include MAP kinases, NFκB, IL-1, TNF-α, and matrix
metalloproteinases (MMP-9 in particular).36–38
In the early stages of dry
eye, inflammation and mechanical irritation stimulates reflex secretion
from the lacrimal gland and increased blink rate. Over time, damage to
the ocular surface leads to reduction in corneal sensation and impaired
reflex tearing.10
In advanced cases, chronic conjunctival damage can
lead to metaplasia and keratinization.
Diagnosis and Classification
The 2007 report from the International Dry Eye WorkShop (DEWS)
defined dry eye syndrome as follows: Dry eye is a multifactorial disease
of the tears and ocular surface that results in ocular discomfort, visual
disturbance, and tear film instability with potential damage to the ocu-
lar surface.10
This definition encompasses all the clinical entities asso-
ciated with systemic disease, as well as idiopathic dry eye disease. As a
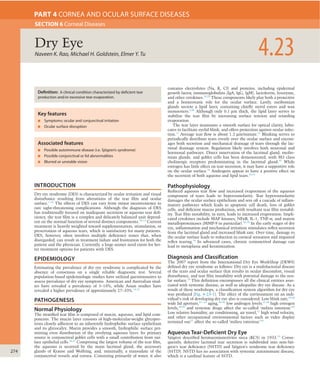
result of these workshops, a classification system algorithm for dry eye
was produced (Fig. 4-23-1). The effect of the environment on an indi-
vidual’s risk of developing dry eye also is considered. Low blink rate,39,40
wide lid aperture,41–-43
aging,44–46
low androgen levels,47,48
high estrogen
levels,49,50
and systemic drugs affect the so-called ‘milieu interieur.’10
Low relative humidity, air conditioning, air travel,51
high wind velocity,
and other occupational environmental factors such as video display
terminal use52
affect the so-called ‘milieu exterieur.’10
Aqueous Tear-Deficient Dry Eye
Sjögren described keratoconjunctivitis sicca (KCS) in 1933.53
Conse-
quently, defective lacrimal tear secretion is subdivided into non-Sjö-
gren’s tear deficiency (NSTD) and Sjögren’s syndrome tear deficiency
(SSTD). NSTD has no association with systemic autoimmune disease,
which is a cardinal feature of SSTD.
Naveen K. Rao, Michael H. Goldstein, Elmer Y. Tu 4.23Dry Eye
SECTION 6 Corneal Diseases
PART 4 CORNEA AND OCULAR SURFACE DISEASES
Associated features
■ Possible autoimmune disease (i.e. Sjögren’s syndrome)
■ Possible conjunctival or lid abnormalities
■ Blurred or unstable vision
Key features
■ Symptoms: ocular and conjunctival irritation
■ Ocular surface disruption
Definition: A clinical condition characterized by deficient tear
production and/or excessive tear evaporation.
2. DryEye
4.23
275
common source for the inhibition of efferent lacrimal gland stimula-
tion through anticholinergic activity or decreased secretion through
systemic dehydration (Table 4-23-1).79
While DES has been reported in
association with menopause, estrogen supplementation has not been
shown to have a beneficial effect.49,80
Alterations in other hormones,
especially androgens, which also are reduced during menopause, have
been implicated.
Sjögren’s syndrome tear deficiency
Sjögren’s syndrome is a clinical condition of aqueous tear deficiency
combined with dry mouth. The syndrome is classified as primary
Non-Sjögren’s tear deficiency
NSTD can occur from primary lacrimal gland deficiencies, secondary
lacrimal gland deficiencies, obstruction of lacrimal gland ducts, or
reflex hyposecretion.10
Primary lacrimal gland deficiencies include age-
related dry eye, congenital alacrima, and familial dysautonomia (Riley–
Day syndrome). The most common form of NSTD is age-related dry
eye, which is associated with ductal and interacinar fibrosis and
obstruction within the lacrimal gland, possibly as a result of low-grade
chronic inflammation.54–56
Congenital alacrima is a rare cause of dry
eye in youth, resulting from primarily absent or hypoplastic lacrimal
glands. Familial dysautonomia is an autosomal recessive multisystem
disorder in which generalized pain insensitivity accompanies absence
of both emotional and reflex tearing. Defective sympathetic and para-
sympathetic innervation of the lacrimal gland and defective sensory
innervation of the ocular surface occur.10
Secondary lacrimal gland deficiency from infiltration and damage to
the lacrimal gland in benign lymphoepithelial lesion (Mikulicz’s dis-
ease), lymphoma, sarcoidosis, hemochromatosis, amyloidosis, HIV/
AIDS, and graft-versus-host disease all can result in dry eye.57–59
Surgi-
cal or radiation-induced destruction or denervation of lacrimal tissue
can result in secondary lacrimal deficiency.57
Secondary obstruction of
the lacrimal gland ducts can occur with trachoma,60
ocular cicatricial
pemphigoid, mucous membrane pemphigoid,61–63
erythema multiforme/
Stevens–Johnson syndrome,64
chemical burns, and thermal burns.65
Reflex hyposecretion of tears can be conceptually divided into reflex
sensory block (damage to the afferent arm) and reflex motor block
(damage to the efferent, or secretomotor arm). Reflex sensory block
occurs with any reduction in ocular surface sensation and leads to
decreased reflex-induced lacrimal secretion and decreased blink rate,
which increases tear evaporation.10,66
Causes of decreased ocular
surface sensation leading to dry eye include topical anesthetic use,67
contact lens wear,68,69
diabetes mellitus,17,70–73
aging, and neurotrophic
keratitis.
As shown by studies utilizing topical anesthesia, interruption of the
afferent stimulus of tear production, or sensory loss (denervation),
results in decreased tear secretion and reduced blink rate.67,74
Damage
to afferent sensory fibers occurs after incisional corneal surgery (pene-
trating or anterior lamellar keratoplasty, radial keratotomy, and limbal
cataract incision) and after damage to the first division of the trigemi-
nal ganglion from trauma, tumor, herpes simplex, or zoster, resulting in
reduced tear production. LASIK and photorefractive keratectomy result-
ing in decreased corneal sensation and blink rate are recognized as
precipitating causes of dry eye.66,75–77,78
Systemic medications are a
Fig. 4-23-1 Dry eye classification. (With permission from Lemp MA.The 1998 Castroviejo Lecture. New strategies in the treatment of dry-eye states. Cornea 1999;18:625–32.)
Contact lens
Rheumatoid arthritis
Systemic lupus erythematosus
Wegener's granulomatosis
Systemic sclerosis
Primary biliary cirrhosis
Other autoimmune diseases
primary secondary
Sarcoid
HIV
Graft vs. host
Xerophthalmia
ablation
Other diseases
Posterior blepharitis
Obstructive meibomian
gland disease
Anterior blepharitis
Sjögren's syndrome Non-Sjögren tear deficiency
Lacrimal obstruction Reflex Oil deficient Lid related Surface changeLacrimal disease
Trachoma, cicatricial pemphigoid
Erythema multiforme
Burns
Neuro-paralytic keratitis
Contact lens
VIIth nerve palsy
Absent glands
Distichiasis
Blink
abnormalities
Aperture
abnormalities
Lid surface
incongruity
Xerophthalmia
Congenital alacrima
acquired primary
lacrimal gland disease
Tear deficient EvaporativeDry eye – keratoconjunctivitis sicca
DRY EYE CLASSIFICATION
TABLE 4-23-1 MEDICATIONS ASSOCIATED WITH DRY EYE SYNDROME
Mechanism of Action Class Medications
Anticholinergic Antimuscarinics Tolterodine tartrate (Detrol)
Scopolamine
Antihistamines (sedating
compounds are
associated with greater
dryness)
Chlorpheniramine (Chlor-
Trimeton)
Diphenhydramine (Benadryl)
Promethazine (Phenergan)
Anti-parkinsonian Benzotropine (Cogentin)
Trihexyphenidyl (Artane)
Antidepressants
MAO inhibitors
Amitriptyline (Elavil)
Nortriptyline (Pamelor)
Imipramines (Tofranil)
Doxepin (Sinequan)
Phenelzine
Antipsychotics Chlorpromazine (Thorazine)
Thioridazine (Mellaril)
Fluphenazine (Prolixin)
Antimanics Lithium
Antiarrhythmics Disopyramide (Norpace)
Mexiletine (Mexitil)
Antiadrenergic Alpha-agonists Clonidine (Catapres)
Methyldopa (Aldomet)
Beta-blockers Propranolol (Inderal)
Metoprolol (Lopressor)
Diuretic Thiazides Hydrochlorothiazide
Other NSAIDs Ibuprofen (Advil)
Naproxen (Naprosyn, Aleve)
Cannabinoids Marijuana
3. 4
276
CORNEAANDOCULARSURFACEDISEASES
the meibomian gland orifices remain anterior to the mucocutaneous
junction, whereas in cicatricial MGD the meibomian gland orifices are
drawn posteriorly onto the lid and tarsal mucosa.
Exposure
Excessive exposure of the ocular surface leads to increased evaporative
loss of tears; thus, any disorder that results in increased ocular expo-
sure can cause evaporative dry eye. Psychological, psychiatric, mechani-
cal, neurological, or traumatic impairment of eyelid function may
result in impaired or reduced blinking, lagophthalmos, or an increased
palpebral fissure width, resulting in an evaporative dry eye. Evaporative
dry eye can be seen in thyroid eye disease secondary to proptosis or lid
retraction.
Mucin Deficiency
Local conjunctival damage from cicatrizing disease or surgical trauma
results not only in aqueous tear deficiency, but also in depopulation of
mucin-producing goblet cells and creation of anatomical abnormalities
of the conjunctiva leading to improper tear distribution. Although
uncommon in incidence, trachoma, pemphigoid, erythema multiforme/
Stevens–Johnson syndrome, and chemical and thermal burns can
result in severe DES characteristically resistant to aqueous tear replace-
ment therapy.
Extrinsic Causes
Vitamin A deficiency can result in extensive goblet cell loss and dys-
function, leading to an unstable tear film and severe dry eye (xeroph-
thalmia).91–94
Preservatives in many eye drops (especially benzalkonium
chloride) can lead to ocular surface toxicity and a dry eye state that may
be reversible if eye drops are switched to nonpreserved formulations.
Contact lens wear is commonly associated with dry eye symptoms.
Pre-lens tear film thinning time and pre-lens lipid layer thickness is
reduced in contact lens wearers with dry eye symptoms, and may lead
to higher evaporative loss.95
Ocular allergies can cause a variety of cor-
neal and conjunctival irregularities with decrease in tear film stability
and consequent dry eye.
OCULAR MANIFESTATIONS
Regardless of the cause, most forms of dry eye share similar symptoms,
interpalpebral surface damage, tear instability, and tear hyperosmolar-
ity. Typical complaints include burning, itching, foreign body sensation,
stinging, dryness, photophobia, ocular fatigue, and redness. Although
symptoms are usually nonspecific, careful attention to details will help
refine the diagnosis.
Patients commonly describe a diurnal pattern with aqueous tear
deficiency with progression of symptoms over the day and decompensa-
tion in particular environmental conditions such as low humidity in
airline cabins, climate control, and the use of video display termi-
nals.52,96
Conversely, night-time exposure, floppy eyelid syndrome, and
inflammatory conditions often present with worst discomfort upon
awakening.
Meibomian gland disease creates an unstable tear film resulting in
intermittent visual blurring and a gritty or sandy sensation. DES in
diabetes and other corneal neuropathies may exhibit little or no dis-
comfort and create high risk for keratolysis.
Common signs of DES include conjunctival injection, decreased tear
meniscus, photophobia, increased tear debris, and loss of corneal sheen
found more commonly in the exposed interpalpebral fissure. Paradoxi-
cal epiphora in DES is usually a result of reflex tearing. Greater risk
for external infections exists secondary to decreased tear turnover
and desiccation of the surface epithelium. Instability of the surface
epithelium and disordered mucin production may lead to painful and
recurrent filamentary keratitis. Although keratinization may occur
uncommonly in chronic DES, vitamin A deficiency also should be
suspected.
Patients who have SSTD tend to have more severe symptoms and
more serious findings than do NSTD patients. Sterile ulceration of the
cornea in SSTD can be peripheral or paracentral; both thinning and
perforation of these ulcers can occur (Fig. 4-23-2). Acute lacrimal
enlargement may be seen in SSTD but should be differentiated from
benign lymphoepithelial lesion (Mikulicz’s disease), which results from
infiltration of the gland without surface findings.97
(patients without a defined connective tissue disease) or secondary
(patients who have a confirmed connective tissue disease).81,82
Primary
SSTD refers to aqueous tear deficiency combined with symptoms of dry
mouth, presence of autoantibodies to Ro(SSA) or La(SSB) antigens,
decreased salivary secretion, and presence of lymphocytic foci on minor
salivary gland biopsy. Secondary SSTD is associated with rheumatoid
arthritis, systemic lupus erythematosus, polyarteritis nodosa, Wegen-
er’s granulomatosis, systemic sclerosis, primary biliary cirrhosis, and
mixed connective tissue disease.10,82
Both subtypes of SSTD feature
progressive lymphocytic infiltration of the lacrimal and salivary glands
and can be associated with severe and painful ocular and oral discom-
fort. The pathogenesis of the tear deficit in SSTD is infiltration of the
lacrimal gland by B and CD4 lymphocytes (with some CD8 lym-
phocytes) and by plasma cells, with subsequent fibrosis.
Revised American-European consensus diagnostic and classification
criteria for Sjögren’s syndrome were published in 2002.82
One point is
given for at least one positive response or positive result in each of the
following categories:
•Ocular symptoms: daily dry eye symptoms for more than 3 months,
ocular irritation, use of artificial tears more than 3 times per day
•Oral symptoms: daily dry mouth symptoms for more than 3
months, presence of swollen salivary glands, frequent drinking of
liquids to aid in swallowing
•Ocular signs: Schirmer I test (without anesthetic) ≤ 5 mm in 5 min-
utes, rose bengal score ≥4 according to the van Bijsterveld scoring
system
•Histopathology: biopsy of minor salivary gland showing inflamma-
tion with lymphocytic foci
•Oral signs: reduced salivary flow ≤1.5 ml in 5 minutes, parotid
sialography showing salivary duct dilation without obstruction,
salivary scintigraphy showing signs of decreased saliva production
•Autoantibodies: presence of anti-Ro(SSA) antibody, presence of
anti-La(SSB) antibody.
For a diagnosis of primary Sjögren’s syndrome, either four of the six
categories (including either histopathology or autoantibodies) or three
of the four objective categories (ocular signs, histopathology, oral signs,
and autoantibodies) must be met. For diagnosis of secondary Sjögren’s
syndrome, in patients with a defined connective tissue disease,
the presence of one symptom (ocular or oral) plus two of the three
objective categories (ocular signs, histopathology, and oral signs) must
be met.
Evaporative Dry Eye
Excessive evaporation that occurs in specific periocular disorders can
cause dry eye disease with or without concurrent aqueous tear defi-
ciency. Evaporation leads to both loss of tear volume and a dispropor-
tionate loss of water, resulting in tear hyperosmolarity. Environmental
conditions such as high altitude, dryness, or extreme heat accelerate
evaporative tear loss even in normal eyes. Causes of evaporative dry
eye can be intrinsic (disease affecting lid structures or dynamics) or
extrinsic.10
Meibomian Gland Disease and Blepharitis
Meibomian gland dysfunction (MGD) leads to both decreased secretion
and abnormal composition of the tear film lipid layer. The abnormal
composition leads to meibomian gland blockage and reduced effective-
ness in the tear film. The resulting ocular surface and eyelid inflamma-
tion perpetuates a cycle of inflammation, scarring, hyperkeratosis,
stenosis, and further MGD.
Often associated, bacterial colonization by normal lid commensals
(Staphylococcus aureus, Propionobacterium acnes, and coagulase-
negative staphylococci) acts directly by altering secreted lipids and
indirectly by causing inflammation. Esters and lipases produced by
these commensals act on secreted lipids in the tear film, producing
soaps that manifest as ‘meibomian foam.’83,84
An association is also
seen with dermatologic conditions such as seborrheic dermatitis, atopic
dermatitis, and acne rosacea, a disorder resulting in vascular dilation,
telangiectasias, and plugging of sebaceous glands of both facial and
eyelid skin. Secondary MGD can occur with use of 13-cis retinoic acid
(isotretinoin) for treatment of acne,85–87
ingestion of polychlorinated
biphenyls in contaminated cooking oil,88–90
and with cicatricial changes
in conditions such as chemical/thermal burns, trachoma, pemphigoid,
erythema multiforme/Stevens–Johnson syndrome, acne rosacea, vernal
keratoconjunctivitis, and atopic keratoconjunctivitis.10
In simple MGD,
4. DryEye
4.23
277
diagnosis of DES, and a result of 6–10 mm of wetting suggests a dry eye
problem.104
Hamano et al. developed the phenol red thread test to obviate the
disadvantages of Schirmer’s test by eliminating the need for anesthe-
sia.105
Three millimeters of a fine dye-impregnated 75 mm cotton
thread is placed under the lateral one-fifth of the inferior palpebral lid
margin for 15 seconds; alkalinity changes its color to bright orange
from tear contact. Asian populations show a lessened wet-length
response with diminishing racial differences with advancing age.106
Hyperosmolarity is a common endpoint for all DES. Its measure-
ment can be a sensitive and specific indicator.104
Its use has been lim-
ited to specialized research centers due to the need for expensive
equipment, but new commercially available devices may make this test
more widely used in the future. Other rarely performed tests for
reduced tear function include fluorophotometry for decreased protein
content, lysozyme levels, ocular ferning, impression cytology, and
lactoferrin assays. Noninvasive imaging of the tear film using menis-
cometry, lipid layer interferometry, high-speed videography, optical
coherence tomography, and confocal microscopy has been advocated as
well.107–111
Other Tests
Corneal sensation may be qualitatively assessed with a cotton wisp, but
quantification requires an instrument such as the Cochet–Bonnet aes-
thesiometer. The tear clearance test measures tear turnover with serial
tear collection after instillation of a standardized volume of dye.103,112
Serological tests, including antinuclear, anti-Ro, and anti-La antibodies,
should be performed in patients suspected of having autoimmune DES.
A definitive diagnosis of Sjögren’s syndrome requires minor salivary or,
rarely, lacrimal gland biopsy. Neither clinical presentation nor individ-
ual ancillary tests alone are sufficient for an accurate diagnosis of DES.
Because of the therapeutic importance of appropriate categorization of
patients, Pflugfelder et al. combined standard subjective examination
with ancillary tests in the evaluation of SSTD, NSTD, inflammatory
MGD, and atrophic MGD patients.113
Clinically important results were
identified and compiled into an algorithm that helps differentiate DES
patients with available tests (Fig. 4-23-4).
TREATMENT
Significant advances have been made in treating the many facets of dry
eye, but it remains a disorder of long-term maintenance rather than
permanent cure. Current therapy focuses on restoring a normal ocular
surface through tear supplementation as well as inhibition of aberrant
inflammation seen in chronic DES. Since the tear film is a highly inte-
grated unit, addressing each component is central to the successful
treatment of DES.
Aqueous Tear Deficiency
As the first line of treatment, artificial tears increase available tears
and, through dilution, reduce tear hyperosmolarity. Commercial artifi-
cial tears differ in electrolyte composition, thickening agents (methyl-
cellulose, hydroxypropyl methylcellulose, polyvinyl alcohol), physiologic
buffering, tonicity, and preservative system. Individual patient prefer-
ences involve such disparate concerns as cost, comfort, visual blurring,
and ease of use. Preserved tears (i.e. benzalkonium chloride) can be
toxic in moderate or severe dry eye, are poorly tolerated, and harmful.
For patients with significant dry eye, single-dose, nonpreserved tear
preparations are the mainstay of therapy with bottled tear products
a reasonable alternative when preserved with relatively nontoxic
compounds. These less toxic preservatives include polyquaternium-1,
sodium chlorite, and sodium perborate.114
Some artificial tear prepara-
tions are formulated to be hypo-osmotic, with the goal of balancing the
hyperosmolarity of the tear film in dry eye. Artificial tear ointments are
effective for longer-lasting control of symptoms, especially during sleep,
but visual blurring limits their daytime usefulness. In addition, some
ointments contain lanolin and parabens, which can be poorly tolerated
by patients with severe dry eye. Autologous serum tears contain trophic
factors and other proteins useful in ocular surface maintenance.114
These can be useful as a preservative-free, biological tear substitute, but
their preparation is labor-intensive.
Punctal occlusion retards tear drainage, thereby increasing tear vol-
ume on the ocular surface and lowering tear osmolarity. Occlusion may
be achieved irreversibly by cauterization or semi-permanently with the
DIAGNOSIS AND ANCILLARY TESTING
Diagnostic Dye Evaluation
Fluorescein is a large molecule unable to traverse normal corneal epi-
thelial tight junctions. In advanced DES, these junctions are disrupted,
allowing characteristic diffuse subepithelial or punctate staining. Rose
bengal, a derivative of fluorescein, in a 1% solution or impregnated
strips, stains devitalized epithelial cells (Fig. 4-23-3).98
Alternatively,
lissamine green stains for cell death or degeneration, as well as cell-to-
cell junction disruption, but does not irritate the eye.99
Tear Film Stability
Tear film instability may be a result of either tear deficiency or evapora-
tive DES. In the tear breakup time (TBUT) test, described by Norn and
revised by Lemp and Holly, fluorescein dye is instilled and the time
interval is measured between a complete blink to the first appearance
of a dry spot in the precorneal tear film.100
TBUTs shorter than 10
seconds indicate tear film instability.
Measurement of Tear Production
The most common means of measuring tear production has been
Schirmer’s test, the details of which were first published in 1903.101
Jones later advocated the use of topical anesthesia combined with a
Schirmer’s test strip for 5 minutes to reduce the stimulating effect of
the filter paper strip – the ‘basal’ tear secretion test.102
Inconsistencies
in its application limit repeatability in DES, but it still enjoys wide-
spread use.103
With these caveats in mind, the following general guide-
lines are recommended (when topical anesthesia is used): a 5-minute
test that results in less than 5 mm of wetting confirms the clinical
Fig. 4-23-2 Patient age 73 with rheumatoid arthritis and secondary Sjögren’s
syndrome.
Fig. 4-23-3 Dry eye syndrome with rose bengal staining.
5. 4
278
CORNEAANDOCULARSURFACEDISEASES
the ocular surface by tear supplementation alone. DES-induced ocular
surface inflammation disrupts the epithelial and mucin layers, further
exacerbating tear film breakdown. Suppression of inflammation creates
a supportive environment for reversal of DES-induced cellular chang-
es.118,119
Topical cyclosporine A has been shown to increase tear produc-
tion in a subset of patients through inhibition of lacrimal gland
inflammation and suppression of DES-induced ocular surface
inflammation.120–122
Judicious use of low-dose topical corticosteroids
has been shown to reduce inflammation and allow normal reparative
mechanisms to restore the natural equilibrium of the ocular sur-
face.123,124
Control of these reactive epithelial changes restores normal
cell morphology, cell-to-cell interactions, and critical mucin production
and clearly has a role in the global treatment of all forms of DES.
Essential fatty acids cannot be synthesized by humans and must be
consumed in the diet. The typical Western diet contains a ratio of
omega-6 to omega-3 fatty acids of approximately 25 to 1.114
Omega-6
fatty acids are precursors to arachidonic acid and proinflammatory
molecules, including PGE2 and LTB4. Omega-3 fatty acids inhibit syn-
thesis of these inflammatory mediators and decrease production of IL-1
and TNF-α.125,126
Supplementing the diet with omega-3 fatty acids has
been shown to decrease both signs and symptoms of dry eye.127
Omega-
3 fatty acids include eicosapentaenoic acid (EPA), docosahexaenoic acid
(DHA), and alpha-linolenic acid (ALA). EPA and DHA are believed to
be primarily responsible for the beneficial health effects of omega-3
fatty acids. Fish oil contains high levels of EPA and DHA, and flaxseed
oil contains high levels of ALA. While ALA is converted by the body
into EPA and DHA, this process is not efficient, so much higher quanti-
ties of flaxseed oil must be consumed to achieve equivalent EPA and
DHA levels from smaller quantities of fish oil.128,129
A number of drugs (mostly topical and a few systemic) are currently
being evaluated in clinical trials aimed at providing new treatment
options for patients with DES.130,131
Success with this research should
provide patients with many more treatment options in the future and
has the potential to improve quality of life for patients suffering with
DES.132
KEY REFERENCES
The Definition and Classification of Dry Eye Disease: Report of the Definition and Classification
Subcommittee of the International Dry Eye WorkShop (2007). The Ocular Surface 2007;5:
75–92.
The Epidemiology of Dry Eye Disease: Report of the Epidemiology Subcommittee of the
International Dry Eye WorkShop (2007). The Ocular Surface 2007;5:93–107.
Ang RT, Dartt DA, Tsubota K. Dry eye after refractive surgery. Curr Opin Ophthalmol 2001;12:
318–22.
use of nonabsorbable plugs. Occlusion with collagen plugs provides
temporary relief (3 days to 6 months) and may identify those at risk for
epiphora prior to permanent occlusion. Epiphora in the setting of one
functional punctum is uncommon.
Secretagogues, agents that stimulate lacrimal gland secretion,
require functional glandular tissue. Oral pilocarpine (Salagen) and
cevimeline (Evoxac) are M3 cholinergic agonists approved for use in dry
mouth that also stimulate tear secretion.32,115,116
Their effect tends to be
greater in oral rather than ocular dryness. Systemic cholinergic side-
effects such as sweating reduce patients’ acceptance. Various nutri-
tional supplements are also touted for DES but without clear
confirmation of their efficacy.
Evaporative Dry Eye
Primary treatment of MGD involves improving the quality and quan-
tity of native meibomian gland secretions. Lid hygiene, in the form of
warm compresses and lid massage, is effective in improving meibomian
gland secretion. Lid scrubs with dilute detergents decrease the sebor-
rheic or bacterial load, thereby breaking the proinflammatory cycle
of MGD. Systemic tetracyclines have been shown to decrease local
inflammation and improve meibomian gland function after several
weeks. The antibacterial effect also contributes to a decrease in meibo-
mian lipid breakdown products in the tear film. Topical erythromycin
or azithromycin applied to the eyelid margins are alternatives for
patients who are unable to tolerate tetracycline derivatives. A number
of lipid-like tear substitutes have become commercially available,
which have been used with some success.117
Correction of eyelid abnormalities that increase exposure of the
ocular surface, such as lower lid ptosis and lagophthalmos, can stabilize
a decompensated ocular surface. In severe cases, a partial or complete
tarsorrhaphy or a conjunctival flap may be necessary to prevent decom-
pensation of the cornea. The use of humidifiers, moisture chambers,
glasses, or goggles increases periocular humidity and decreases surface
evaporative pressure. New high-Dk (oxygen permeability), high-water-
content contact lenses and new polymer lenses, accompanied by proper
tear supplementation and hygiene, are effective in treating DES
patients with poor corneal wetting. In patients with severe dry eye,
scleral contact lenses can promote lubrication and slow evaporation of
tears from the ocular surface.
Ocular Surface Inflammation
Ocular surface inflammation and its consequential cellular changes are
not only a common endpoint of all DES, but also prevent restoration of
Fig. 4-23-4 Diagnostic algorithm for ocular irritation.
(With permission from Pflugfelder SC,Tseng SC, Sanabria O, et al.
Evaluation of subjective assessments and objective diagnostic tests for
diagnosing tear-film disorders known to cause ocular irritation. Cornea
1998;17:38–56.)
No
Yes
Consider nontear
film related problems
Fluorescein tear break-up time 10 sec
1. Schirmer 1 5 mm in one or both eyes
2. Aqueous tear deficiency pattern on fluorescein clearance test
3. Grid distortion by xeroscope
Symptoms of ocular irritation
Tear film instability
Yes
Meibomian gland disease
NoYes
Yes No
Meibomian gland pathologic signs
1. Orifice metaplasia
2. Acinar atrophy
3. Reduced expressible meibum
Aqueous tear deficiency
1. Absence of nasal-lacrimal reflex
2. Presence of serum autoantibodies
3. van Bijsterveld rose bengal staining score 3
4. Exposure zone fluorescein staining score 3
Sjögren
syndrome
Non-Sjögren
syndrome
ALGORITHM FOR OCULAR IRRITATION
6. DryEye
4.23
279
Solomon A, Dursun D, Liu Z, et al. Pro- and anti-inflammatory forms of interleukin-1 in the
tear fluid and conjunctiva of patients with dry-eye disease. Invest Ophthalmol Vis Sci
2001;42:2283–92.
Stern ME, Gao J, Siemasko KF, et al. The role of the lacrimal functional unit in the pathophysiology
of dry eye. Exp Eye Res 2004;78:409–16.
Sullivan DA, Hammitt KM, Schaumberg DA, et al. Report of the TFOS/ARVO Symposium on global
treatments for dry eye disease: an unmet need. Ocul Surf 2012;10:108–16.
Tseng SC, Tsubota K. Important concepts for treating ocular surface and tear disorders. Am J
Ophthalmol 1997;124:825–35.
Vitali C, Bombardieri S, Jonnson R, et al. Classification criteria for Sjögren’s syndrome: a revised
version of the European criteria proposed by the American-European Consensus Group.
Ann Rheum Dis 2002;1:554–8.
Wilson SE. Laser in situ keratomileusis-induced (presumed) neurotrophic epitheliopathy.
Ophthalmology 2001;108:1082–7.
Barabino S, Chen Y, Chauhan S, et al. Ocular surface immunity: homeostatic mechanisms and
their disruption in dry eye disease. Prog Retin Eye Res 2012;31:271–85.
Begley CG, Chalmers RL, Abetz L, et al. The relationship between habitual patient-reported
symptoms and clinical signs among patients with dry eye of varying severity. Invest
Ophthalmol Vis Sci 2003;44:4753–61.
Fox RI, Michelson P. Approaches to the treatment of Sjögren’s syndrome. J Rheumatol Suppl
2000;61:15–21.
Lemp MA. The 1998 Castroviejo Lecture New strategies in the treatment of dry-eye states. Cornea
1999;18:625–32.
Rolando M, Zierhut M. The ocular surface and tear film and their dysfunction in dry eye disease.
Surv Ophthalmol 2001;45(Suppl 2):S203–10.
Schaumberg DA Sullivan DA, Buring JE, et al. Prevalence of dry eye syndrome among US women.
Am J Ophthalmol 2003;136:318–26.
Schein OD, Hochberg MC, Munoz B, et al. Dry eye and dry mouth in the elderly: a population-
based assessment. Arch Intern Med 1999;159:1359–63.
Schein OD, Munoz B, Tielsch JM, et al. Prevalence of dry eye among the elderly. Am J Ophthalmol
1997;124:723–8.
Access the complete reference list online at