1. The document provides an overview of the CooperSurgical Fetal Monitor model F9, including its buttons and functions, components, benefits, and guidelines for use and care.
2. It describes the monitor's touchscreen display, large color monitor, ultrasound transducer, and software features for transferring data.
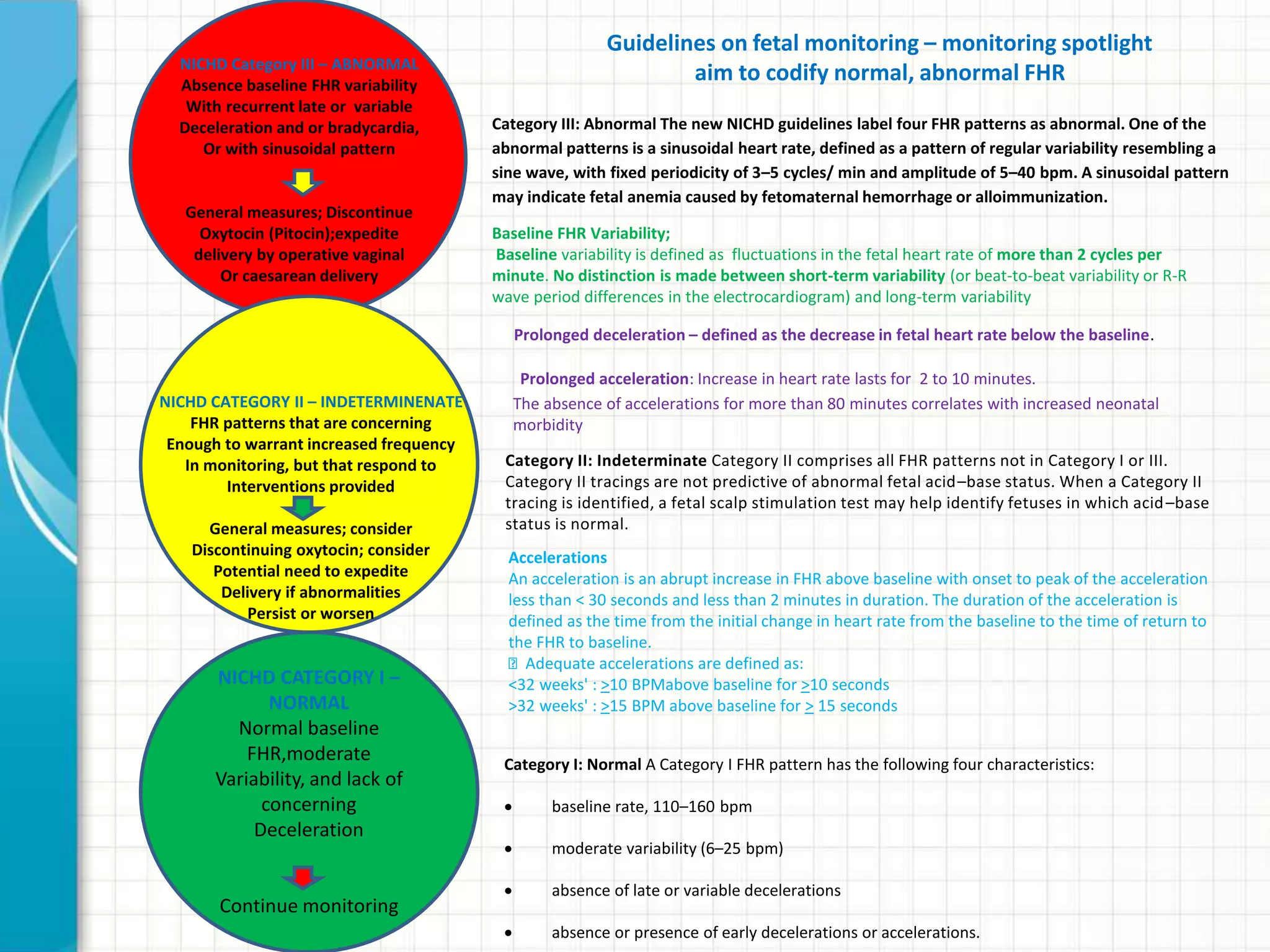
3. The document also outlines the National Institute of Child Health and Human Development categories for normal, indeterminate, and abnormal fetal heart rate patterns and general measures for each category.