
Recommended
Recommended
More Related Content
Similar to Chapter 1Major Characteristics of U.S.Health Care Delive.docx
Similar to Chapter 1Major Characteristics of U.S.Health Care Delive.docx (16)
More from walterl4
More from walterl4 (20)
Recently uploaded
Recently uploaded (20)
Chapter 1Major Characteristics of U.S.Health Care Delive.docx
- 1. Chapter 1 Major Characteristics of U.S. Health Care Delivery INTRODUCTION The United States has a unique system of health care delivery. For the purposes of this discussion, “health care delivery” and “health services delivery” can have slightly different meanings, but in a broad sense, both terms refer to the major components of the system and the processes that enable people to receive health care. In a more restricted sense, the terms refer to the act of providing health care services to patients. The reader can identify which meaning is intended by paying attention to context. In contrast to the United States, most developed countries have national health insurance programs that are run by the government and financed through general taxes. Almost all of the citizens in such countries are enti- tled to receive health care services that include routine and basic health care. These countries have what is commonly referred to as universal
- 2. access. All American citizens, on the other hand, are not entitled to routine 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 1 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 2 Chapter 1 • Major Characteristics of U.S. Health Care Delivery and basic health care services. Although the U.S. health care delivery sys- tem has evolved in response to concerns about cost, access, and quality, the system has been unable to provide universally a basic package of health care at an affordable cost. One barrier to universal coverage is the unneces- sary fragmentation of the U.S. delivery system, which is perhaps its central feature (Shortell et al., 1996); however, the enormous challenge of expand- ing access to health care while containing overall costs and maintaining expected levels of quality continues to intrigue academics, policy makers, and politicians. To make learning the structural and conceptual bases for the delivery of health services easier, this book is organized by the systems framework, which is presented at the end of this chapter. One of the main
- 3. objectives of Chapter 1 is to provide a broad understanding of how health care is deliv- ered in the United States. The following overview introduces the reader to several concepts that are treated more extensively in later chapters. The U.S. health care delivery system is complex and massive. Interestingly, it is not actually a system in the true sense, although it is called a system when its various features, com- ponents, and services are referenced. Hence, it may be somewhat mislead- ing to talk about the American health care delivery “system” (Wolinsky, 1988, p. 54), but the term will nevertheless be used throughout this book. Organizations and individuals involved in health care range from edu- cational and research institutions, medical suppliers, insurers, payers, and claims processors to health care providers. Total employment in various health delivery settings is almost 14.4 million, including professionally active doctors of medicine (MDs), doctors of osteopathy (DOs), active nurses, dentists, pharmacists, and administrators. Approximately 382,000 physical, occupational, and speech therapists provide rehabilitation services. The vast array of institutions includes 5,700 hospitals, 15,900 nursing
- 4. homes, almost 2,900 inpatient mental health facilities, and 11,000 home health agencies and hospices. Close to 800 programs include basic health services for migrant workers and the homeless, community health centers, black lung clinics, human immunodeficiency virus (HIV) early interven- tion services, and integrated primary care and substance abuse treatment programs. Various types of health care professionals are trained in 144 medical and osteopathic schools, 56 dental schools, 109 schools of pharmacy, and more than 1,500 nursing programs located throughout the country. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 2 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. Subsystems of U.S. Health Care Delivery 3 There are 201.7 million Americans with private health insurance coverage, 40.3 million Medicare beneficiaries, and 38.3 million Medicaid recipients. Health insurance can be purchased from approxi- mately 1,000 health insurance companies and 70 Blue Cross/Blue Shield plans. The managed care sector includes approximately 405 licensed health maintenance organizations (HMOs) and 925 preferred
- 5. provider organizations (PPOs). A multitude of government agencies are involved with the financing of health care, medical and health services research, and regulatory oversight of the various aspects of the health care deliv- ery system (Aventis Pharmaceuticals, 2002; Bureau of Primary Health Care, 1999; National Center for Health Statistics, 2007; U.S. Bureau of the Census, 1998; U.S. Census Bureau, 2007; Bureau of Labor Statistics, 2008). SUBSYSTEMS OF U.S. HEALTH CARE DELIVERY The United States does not have a universal health care delivery system enjoyed by everyone. Instead, multiple subsystems have developed, either through market forces or the need to take care of certain population seg- ments. Discussion of the major subsystems follows. Managed Care Managed care is a system of health care delivery that (1) seeks to achieve efficiency by integrating the basic functions of health care delivery, (2) employs mechanisms to control (manage) utilization of medical services, and (3) determines the price at which the services are purchased and, conse- quently, how much the providers get paid. It is the most
- 6. dominant health care delivery system in the United States today and is available to most Americans (for more details on managed care, please refer to Chapter 9). The employer or government is the primary financier of the managed care system. Instead of purchasing coverage from a traditional insurance company, the financier contracts with a managed care organization (MCO), such as an HMO or a PPO, to offer a selected health plan to employees. In this case, the MCO functions like an insurance company and promises to provide health care services contracted under the health plan to the enrollees of the plan. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 3 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 4 Chapter 1 • Major Characteristics of U.S. Health Care Delivery The term enrollee (member) refers to the individual covered under the plan. The contractual arrangement between the MCO and the enrollee— including the collective array of covered health services that the enrollee is entitled to—is referred to as the health plan (or “plan” for
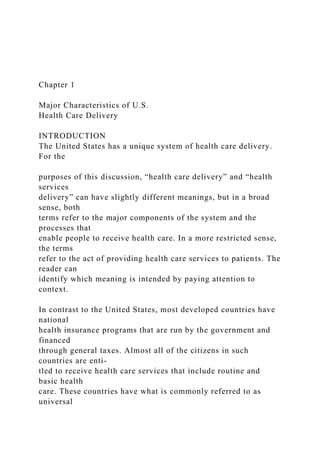
- 7. short). The health plan uses selected providers from whom the enrollees can choose to receive routine services. Primary care providers or general practitioners typically manage routine services and determine appropriate referrals for higher level or specialty services, often earning them the name of gate- keeper. The choice of major service providers, such as hospitals, is also limited. Some of the services may be delivered through the plans own hired physicians, but most are delivered through contracts with providers such as physicians, hospitals, and diagnostic clinics. Although the employer finances the care by purchasing a plan from an MCO, the MCO is then responsible for negotiating with providers. Providers are typically paid either through a capitation (per head) arrange- ment, in which providers receive a fixed payment for each patient or employee under their care, or a discounted fee. Providers are willing to dis- count their services for MCO patients in exchange for being included in the MCO network and being guaranteed a patient population. Health plans rely on the expected cost of health care utilization, which always runs the risk of costing more than the premiums collected. By underwriting this risk, the plan assumes the role of insurer.
- 8. Figure 1.1 illustrates the basic functions and mechanisms that are nec- essary for the delivery of health services within managed care. The key functions of financing, insurance, delivery, and payment make up the quad- function model. Managed care arrangements integrate the four functions to varying degrees. Military The military medical care system is available free of charge to active- duty military personnel of the U.S. Army, Navy, Air Force, and Coast Guard and also to certain uniformed nonmilitary services such as the Public Health Service and the National Oceanographic and Atmospheric Association (NOAA). It is a well-organized, highly integrated system. It is comprehensive and covers preventive as well as treatment services that are provided by salaried health care personnel, many of whom are themselves in the military or uniformed services. This system combines public health 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 4 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.
- 9. Subsystems of U.S. Health Care Delivery 5 with medical services. Routine ambulatory care is provided close to the military personnel’s place of work at the dispensary, sick bay, first-aid sta- tion, or medical station. Routine hospital services are provided at base dis- pensaries, in sick bays aboard ship, and at base hospitals. Complicated hospital services are provided in regional military hospitals. Long-term care is provided through Veterans Administration (VA) facilities to certain retired military personnel. Although patients have little choice regarding how services are provided, in general, the military medical care system provides high-quality health care. Families and dependents of active-duty or retired career military per- sonnel are either treated at the hospitals or dispensaries or are covered by Employers Government–Medicare, Medicaid Individual self-funding FINANCING Insurance companies Blue Cross/Blue Shield Self-insurance
- 10. INSURANCE Insurance companies Blue Cross/Blue Shield Third-party claims processors PAYMENT Physicians Hospitals Nursing homes Diagnostic centers Medical equipment vendors Community health centers DELIVERY (Providers) Access Risk underwriting Capitation or discounts Utilization controls Integration of functions through managed care (HMOs, PPOs) Figure 1.1 Managed Care: Integration of Functions 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 5
- 11. © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 6 Chapter 1 • Major Characteristics of U.S. Health Care Delivery TRICARE, a program that is financed by the military. This insurance plan permits the beneficiaries to receive care from private medical care facilities as well as military ones. The VA health care system is available to retired veterans of previous military service, with priority given to those who are disabled. The VA sys- tem focuses on hospital care, mental health services, and long- term care. It is one of the largest and oldest (1946) formally organized health care sys- tems in the world. Its mission is to provide medical care, education and training, research, contingency support, and emergency management for the Department of Defense medical care system. It provides health care to more than 5.5 million persons at over 1,100 sites, including 153 hospitals, 732 ambulatory and community-based clinics, 135 nursing homes, 209 counseling centers, 47 domiciliaries (residential care facilities), 73 home health care programs, and various contract care programs. The VA budget
- 12. is over $30 billion, and it employs a staff of 263,350 as of 2007 (National Center for Veterans Analysis and Statistics, 2007). The entire VA system is organized into 22 geographically distributed Veterans Integrated Service Networks (VISNs). Each VISN is responsible for coordinating the activi- ties of the hospitals, outpatient clinics, nursing homes, and other facilities located within its jurisdiction. Each VISN receives an allocation of federal funds and is responsible for equitable distribution of those funds among its hospitals and other providers. VISNs are also responsible for improving efficiency by reducing unnecessarily duplicative services, by emphasizing preventive services, and by shifting services from costly inpatient care to less costly outpatient care. Subsystem for Vulnerable Populations Vulnerable populations, particularly those who are poor and uninsured or of minority and immigrant status, live in geographically or economically disadvantaged communities and receive care from “safety net” providers. These providers include health centers, physicians’ offices, and hospital outpatient and emergency departments; of these, health centers are expressly designed to serve the underserved. Consistent with their unique
- 13. role and mission, safety net providers offer comprehensive medical and enabling (e.g., language translation, transportation, outreach, nutrition and health education, social support services, case management, and child care) services targeted to the needs of vulnerable populations. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 6 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. Subsystems of U.S. Health Care Delivery 7 For example, for over 30 years, federally funded health centers have pro- vided primary and preventive health services to rural and urban underserved populations. The Bureau of Primary Health Care (BPHC), located in the Health Resources and Services Administration in the Department of Health and Human Services (DHHS), provides federal support for community- based health centers that include programs for migrant and seasonal farm workers and their families, homeless persons, public housing residents, and school-aged children. These services facilitate regular access to care for patients who are predominantly minority, low-income, uninsured, or receiv- ing Medicaid. By the end of calendar year 2002, the nationwide
- 14. network of 843 reporting health centers delivered essential primary and preventive care at more than 3,500 sites, serving more than one fifth (more than 11 million) of the nation’s 50 million underserved persons (Bureau of Primary Health Care, 2002). Health centers have contributed to significant improvements in health outcomes for the uninsured and Medicaid populations and have reduced disparities in health care and health status across socioeconomic and racial/ethnic groups (Politzer et al., 2003; Shi et al., 2001). In addition to health centers, government health insurance programs, such as Medicare, Medicaid, and State Children’s Health Insurance Program (SCHIP), provide vulnerable populations with access to health care services. Medicare is one of the largest sources of health insurance in the coun- try, serving nearly 39 million people, who are either 65 years old or older and who are suffering from certain disabilities or are diagnosed with end- stage renal disease. Managed by the Health Care Financing Administration (HCFA), another division within the DHHS, Medicare is composed of three parts, Part A, Part B, and most recently Part D. Part A and Part B were the original divisions of the Medicare program. Part A covers
- 15. health care received in hospitals, nursing facilities, hospice care, and some home health care with no monthly premiums, while Part B covers doctors’ ser- vices and other outpatient care not included in Part A with an additional monthly premium, which in 2008 cost about $96.40 per month. Part D, or the Medicare Prescription Drug Plan, provides coverage for brand-name and generic prescription drugs at pharmacies involved in the program. The program is designed to protect those in Medicare burdened with very high drug costs or unexpected prescription bills in the future. In addition, Medicaid, the third largest source of health insurance in the country, provides coverage for low-income women, children, elderly 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 7 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 8 Chapter 1 • Major Characteristics of U.S. Health Care Delivery people, and individuals with disabilities, covering 12% of the U.S. popula- tion. The program offers these vulnerable populations health insurance and
- 16. long-term care for older Americans and individuals with disabilities and also provides additional coverage for low-income Medicare recipients for services not provided in the Medicare Part A Plan, such as outpatient care and prescription drugs. Finally, with the growing uninsured population, the government has taken the initiative to provide insurance to children in uninsured families through SCHIP. Established in 1997, it expands coverage to children in families who do not qualify for Medicaid but who have a modest income, although each state has its own rules of eligibility. For little or no cost, the insurance pays for the child’s physician visits, immunizations, hospitaliza- tions, and emergency room visits. America’s safety net, however, is by no means secure, and the avail- ability of safety net providers varies from community to community. Vulnerable populations residing in communities without safety net providers have to forego care or seek care from hospital emergency depart- ments if one is nearby. Safety net providers face enormous pressure from the increasing number of uninsured and poor in their communities. The inability to shift costs for uncompensated care onto private insurance has
- 17. become a significant problem as revenues from Medicaid, the primary source of third-party financing for core safety net providers, are restricted. Integrated Delivery Over the last decade, the hallmark of the U.S. health care industry has been organizational integration to form integrated delivery systems (IDSs) or networks. An IDS represents various forms of ownership and other strategic linkages among hospitals, physicians, and insurers. Its objective is to have one health care organization deliver a range of services. An IDS can be defined as a network of organizations that provides or arranges to pro- vide a coordinated continuum of services to a defined population and that is willing to be held clinically and fiscally accountable for the outcomes and health status of the population. From the standpoint of integration, the major participants or players in the health care delivery system are physi- cians, hospitals, and insurers. The key strategic position that physicians, hospitals, and insurers hold gives rise to different forms of IDSs (see Chapter 9). 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 8 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR
- 18. DISTRIBUTION. Characteristics of the U.S. Health Care System 9 CHARACTERISTICS OF THE U.S. HEALTH CARE SYSTEM The health care system of a nation is influenced by external factors, including the political climate, stage of economic development, techno- logic progress, social and cultural values, the physical environment, and population characteristics such as demographic and health trends. It fol- lows, then, that the combined interaction of these environmental forces influences the course of health care delivery in the United States. This sec- tion summarizes the basic characteristics that differentiate the U.S. health care delivery system from that of other countries. There are eight main areas of distinction (see Exhibit 1.1). No Central Governing Agency; Little Integration and Coordination The U.S. health care system stands in conspicuous contrast to the health care systems of other developed countries. The centrally controlled universal health care system that most developed countries have authorizes the financing, payment, and delivery of health care to all
- 19. residents. The U.S. system, however, is not centrally controlled and therefore has a variety of payment, insurance, and delivery mechanisms, and health care is financed both publicly and privately. Private financing, which is predomi- nantly through employers, accounts for approximately 55% of total health care expenditures; the government finances the remaining 45% (National Center for Health Statistics, 2002). Exhibit 1.1 Main Characteristics of the U.S. Health Care System • No central governing agency and little integration and coordination • Technology-driven delivery system focusing on acute care • High on cost, unequal in access, average in outcome • Delivery of health care under imperfect market condition • Legal risks influence practice behaviors • Government as subsidiary to the private sector • Market justice vs. social justice: conflict throughout health care • Multiple players and balance of power • Quest for integration and accountability • Access to health care services is selectively
- 20. based on insurance coverage 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 9 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 10 Chapter 1 • Major Characteristics of U.S. Health Care Delivery Centrally controlled health care systems are less complex. They are also less costly because they can manage total expenditures through global budgets and can govern the availability and utilization of services. Because the United States has such a large private system of financing as well as delivery, the majority of hospitals and physician clinics are private busi- nesses, independent of the government. Nevertheless, the federal and state governments in the United States play an important role in health care delivery. They determine public sector expenditures and reimbursement rates for services provided to Medicaid and Medicare patients. The govern- ment also formulates standards of participation through health policy and regulation, which means that providers must comply with the standards established by the government in order to deliver care to Medicaid and
- 21. Medicare patients. Certification standards are also regarded as minimum standards of quality in most sectors of the health care industry. Technology Driven and Focusing on Acute Care The United States has been the hotbed of research and innovation in new medical technology. Growth in science and technology often creates a demand for new services despite shrinking resources to finance sophisti- cated care. Other factors contribute to increased demand for expensive technological care: Patients assume that current technologies offer the best care; physicians want to try the latest gadgets. Even hospitals compete on the basis of having the most modern equipment and are often under pres- sure to recoup capital investments made in technology by using it. Legal risks for providers and health plans alike may also play a role in the reluc- tance to deny new technology. Although technology has ushered in a new generation of successful interventions, the negative outcomes resulting from its overuse are many. For example, the cost of highly technical interventions adds to the rising costs of health care, making it more difficult for employers to extend insur- ance to part-time workers or for insurance companies to lower their premi-
- 22. ums. Because there are limited resources to invest in the American health care system, it is essential to think twice before assuming that the best solu- tion always involves technology. Considering the broad benefits of primary care in preventing acute conditions that ultimately require technological intervention, it seems essential to strive for a balanced investment in both high- and low-technology medicine. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 10 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. Characteristics of the U.S. Health Care System 11 High on Cost, Unequal in Access, and Average in Outcome The United States spends more than any other developed country on health care (primarily medical care), and costs continue to rise at an alarm- ing rate. Despite spending such a high percentage (13%) of the nation’s gross domestic product on health care, many U.S. residents have limited access to even the most basic care (Anderson et al., 2003). Access means the ability of an individual to obtain health care services when needed. In the United States, access is restricted to those
- 23. who (1) have health insurance through their employers, (2) are covered under a government health care program, (3) can afford to buy insurance out of their own private funds, and (4) are able to pay for services pri- vately. Health insurance is the primary means for ensuring access. In 2000, the number of uninsured Americans—those without private or pub- lic health insurance coverage—was estimated to be 40.5 million or 16.8% of the U.S. population (National Center for Health Statistics, 2002). For consistent basic and routine care, commonly referred to as primary care, the uninsured are unable to see a physician unless they can pay the physi- cian’s fees. Those who cannot afford to pay generally wait until health problems develop, at which point they may be able to receive services free of charge in a hospital emergency department. Uninsured Ameri- cans therefore are able to obtain medical care for acute illness. Hence, one can say that the United States does have a form of universal cata- strophic health insurance even for the uninsured (Altman & Reinhardt, 1996, p. xxvi). It is well acknowledged that the absence of insurance inhibits the patient’s ability to receive well-directed, coordinated, and continuous
- 24. health care through access to primary care services and, when needed, referral to specialty services. Experts generally believe that the inadequate access to basic and routine primary care services is the main reason that the United States, in spite of being the most economically advanced country, lags behind other developed nations in measures of population health such as infant mortality and overall life expectancy. Imperfect Market Conditions Under national health care programs, patients have varying degrees of choice in selecting their providers; however, true economic market forces 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 11 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 12 Chapter 1 • Major Characteristics of U.S. Health Care Delivery are virtually nonexistent. In the United States, even though the delivery of services is largely in private hands, health care is only partially governed by free market forces. The delivery and consumption of health care in the United States do not quite meet the basic tests of a free market.
- 25. Hence, the system is best described as a quasi-market or an imperfect market. The fol- lowing key characteristics of free markets help explain why U.S. health care is not a true free market. In a free market, multiple patients (buyers) and providers (sellers) act independently. In a free market, patients should be able to choose their provider based on price and quality of services. If it were this simple, patient choice would determine prices by the unencumbered interaction of supply and demand. Theoretically, at least, prices are negotiated between payers and providers; however, in many cases, the payer is not the patient but an MCO, Medicare, or Medicaid. Because prices are set by agencies external to the market, they are not freely governed by the forces of supply and demand. For the health care market to be free, unrestrained competition must occur among providers on the basis of price and quality. Generally speak- ing, free competition exists among health care providers in the United States. The consolidation of buying power into the hands of private health plans, however, is forcing providers to form alliances and IDSs on the sup- ply side. As explained earlier, IDSs are networks that offer a
- 26. range of health care services. In certain geographic sectors of the country, a single giant medical system has taken over as the sole provider of major health care services, restricting competition. As the health care system continues to move in this direction, it appears that only in large metropolitan areas will there be more than one large integrated system competing to get the busi- ness of the health plans. A free market requires that patients have information about the avail- ability of various services. Free markets operate best when consumers are educated about the products they are using, but patients are not always well informed about the decisions that need to be made regarding their care. Choices involving sophisticated technology, diagnostic methods, interven- tions, and pharmaceuticals can be difficult and often require physician input. Acting as an advocate, primary care providers can reduce this infor- mation gap for patients. Recently, health care consumers have taken the ini- tiative to educate themselves with the use of Internet resources for 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 12 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.
- 27. Characteristics of the U.S. Health Care System 13 gathering medical information. Pharmaceutical product advertising is also having an impact on consumer expectations and increasing awareness of available medications. In a free market, patients have information on price and quality for each provider. Current pricing methods for health care services further con- found free market mechanisms. Hidden costs make it difficult for patients to gauge the full expense of services ahead of time. Item-based pricing, for example, refers to the costs of ancillary services that often accompany major procedures such as surgery. Patients are usually informed of the surgery’s cost ahead of time but cannot anticipate the cost of anesthesiolo- gists and pathologists or hospital supplies and facilities, thus making it extremely difficult to ascertain the total price before services have actually been received. Package pricing and capitated fees can help overcome these drawbacks by providing a bundled fee for a package of related services. Package pricing covers services bundled together for one episode of care, which is less encompassing than capitation. Capitation covers
- 28. all services an enrollee may need during an entire year. In recent years, the quality of care has received much attention. Performance rating of health plans has met with some success; however, apart from sporadic news stories, the public generally has scant informa- tion on the quality of health care providers. In a free market, patients must directly bear the cost of services received. The purpose of insurance is to protect against the risk of unfore- seen major events. Because the fundamental purpose of insurance is to meet major expenses when unlikely events occur, having insurance for basic and routine health care undermines the principle of insurance. Health insurance coverage for minor services such as colds, coughs, and earaches amounts to prepayment for such services. There is a moral hazard that after enrollees have purchased health insurance they will use health care services to a greater extent than if they were without health insurance. Even certain referrals to higher level services may be foregone if the patient has to bear the full cost of these services. In a free market for health care, patients as consumers make decisions about the purchase of health care services. The main factors that severely limit the patient’s ability to make health care purchasing
- 29. decisions have already been discussed. At least two additional factors limit the ability of patients to make decisions. First, decisions about the utilization of health 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 13 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 14 Chapter 1 • Major Characteristics of U.S. Health Care Delivery care are often determined by need rather than price-based demand. Need has generally been defined as the amount of medical care that medical experts believe a person should have to remain or become healthy (Feldstein, 1993, p. 74–75). Second, the delivery of health care can result in creation of demand. This follows from self-assessed need that, coupled with moral hazard, leads to greater utilization. This creates an artificial demand because prices are not taken into consideration. Practitioners who have a financial interest in additional treatments also create artificial demand (Hemenway & Fallon, 1985), commonly referred to as provider- induced demand.
- 30. Government as Subsidiary to the Private Sector In most other developed countries, the government plays a central role in the provision of health care. In the United States, however, the pri- vate sector plays the dominant role. This can be explained to some degree by the American tradition of reliance on individual responsibility and a commitment to limiting the power of the national government. As a result, government spending for health care has been largely confined to filling in the gaps left open by the private sector. These gaps include environ- mental protections, support for research and training, and care of vulnera- ble populations. Market Justice versus Social Justice: Conflict Throughout Health Care Market justice and social justice are two contrasting theories that gov- ern the production and distribution of health care services in the United States. The principle of market justice places the responsibility for the fair distribution of health care on the market forces in a free economy. Medical care and its benefits are distributed on the basis of people’s willingness and ability to pay (Santerre & Neun, 1996, p. 7). In contrast, social justice emphasizes the well-being of the community over that of the
- 31. individual; thus, the inability to obtain medical services because of a lack of financial resources would be considered unjust. A just distribution of benefits must be based on need, not simply one’s ability to purchase them in the market- place. In a partial public and private health care system, the two theories often work well hand in hand, contributing ideals from both theories; how- ever, market justice principles tend to prevail. As mentioned before, Americans generally prefer market solutions to government intervention in 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 14 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. Characteristics of the U.S. Health Care System 15 health care financing and delivery. Unfortunately, market justice results in the unequal allocation of health care services, neglecting critical human concerns that are not confined to the individual but have broader, negative impacts on society (see Chapter 2 for contrast between market and social justice). Multiple Players and Balance of Power
- 32. The U.S. health services system involves multiple players. The key players in the system have been physicians, administrators of health service institutions, insurance companies, large employers, and the gov- ernment. Big business, labor, insurance companies, physicians, and hos- pitals make up the powerful and politically active special interest groups represented before lawmakers by high-priced lobbyists. Each player has a different economic interest to protect. The problem is that the self- interests of each player are often at odds. For example, providers seek to maximize government reimbursement for services delivered to Medicare and Medicaid patients, but the government wants to contain cost increases. The fragmented self-interests of the various players produce counteract- ing forces within the system. One positive effect of these opposing forces is that they prevent any single entity from dominating the system. In an environment that is rife with motivations to protect conflicting self-interests, achieving comprehensive system-wide reforms is next to impossible, and cost containment remains a major challenge. Conse- quently, the approach to health care reform in the United States is char- acterized as incremental or piecemeal and is sometimes
- 33. regressive when administrations change followed by its ripple effect on government health agencies. Quest for Integration and Accountability Currently in the United States, there is a drive to use primary care as the organizing hub for continuous and coordinated health services. Although this model gained popularity with the expansion of managed care, the model’s development stalled before reaching its full potential. The envisioned role for primary care would include integrated health care by offering comprehensive, coordinated, and continuous services with a seam- less delivery. Furthermore, the model emphasizes the importance of the patient–provider relationship and how it can best function to improve the 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 15 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 16 Chapter 1 • Major Characteristics of U.S. Health Care Delivery health of each individual and thus strengthen the population. Integral to
- 34. the relationship is the concept of accountability. Accountability on the provider’s behalf means ethically providing quality health care in an effi- cient manner. On the patient’s behalf, it means safeguarding one’s own health and using available resources sensibly. Access to Health Care Services Is Selectively Based on Insurance Coverage Unlike countries with national health plans providing universal access, the United States’ access to health care services is limited. Access is granted only to individuals who (1) have health insurance through their employers, (2) are covered under a government health care program, (3) can afford to buy insurance with their own private funds, and (4) can pay for services privately. Although the United States offers some of the best medical care in the world, this care is often available only to individuals with health insurance plans that provide adequate coverage or sufficient resources to pay for the procedures themselves. In addition, there is a relatively large population of uninsured in the country. In 2006, 47 million people (15.8% of the population) were unin- sured, meaning they were not covered by any type of insurance program, public nor private (DeNavas-Walt et al., 2006). This statistic
- 35. does not include individuals in the population who are underinsured or only inter- mittently insured in a given year. The uninsured have limited options when seeking medical care. They can either (1) pay physicians out of pocket that are typically at higher rates than those paid by insurance plans, (2) access federally funded health centers, or (3) obtain treatment for acute illnesses at a hos- pital emergency department for which hospitals do not receive direct payments unless patients have the ability to pay. The Emergency Medical Treatment and Labor Act of 1986 requires screening and evaluation of every patient, necessary stabilizing treatment, and admitting when nec- essary, regardless of ability to pay. Unfortunately, the inappropriate use of emergency departments results in cost-shifting, where patients able to pay for services, privately insured individuals, employers, and the gov- ernment ultimately cover the costs provided to the uninsured in the emer- gency room. Also, the lack of insurance restricts the patients’ capability 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 16 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION.
- 36. Health Care Systems of Other Developed Countries 17 to receive well-directed, coordinated, and continuous health care through access to primary care services, and when necessary, referral to specialty services. Legal Risks Influence Practice Behaviors Americans as a society are quick to engage in lawsuits. Motivated by prospects of enormous jury awards, people are easily prompted to drag alleged offenders into the courtroom because of the slightest perceptions of incurred harm. Because private health care providers are increasingly becoming more susceptible to litigations, risk of malpractice lawsuits is a serious consideration in the practice of medicine. As a form of protection, most providers engage in what is known as defensive medicine by prescrib- ing additional diagnostic tests, scheduling checkup appointments, and maintaining abundant documentation on cases. Many of these efforts are unnecessary and only drive up costs and inefficiency. HEALTH CARE SYSTEMS OF OTHER DEVELOPED COUNTRIES Most Western European countries have national health care programs
- 37. that provide universal access. There are three basic models for structuring national health care systems. In a system under National Health Insurance, such as Canada, the government finances health care through general taxes, but the actual care is delivered by private providers. In the context of the quad-function model (see Figure 1.1), National Health Insurance requires a tighter consolidation of the financing, insurance, and payment functions, which are coordinated by the government. Delivery is characterized by detached private arrangements. In a national health system, such as the one in Great Britain, in addition to financing a tax-supported national health insurance program, the govern- ment also manages the infrastructure for the delivery of medical care. Under such a system, most of the medical institutions are operated by the government. Most health care providers, such as physicians, are either gov- ernment employees or are tightly organized in a publicly managed infra- structure. In the context of the quad-function model, a National Health System requires a tighter consolidation of all four functions, typically by the government. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 17
- 38. © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 18 Chapter 1 • Major Characteristics of U.S. Health Care Delivery In a socialized health insurance system, such as in Germany, health care is financed through government-mandated contributions by employers and employees. Health care is delivered by private providers. Private not-for-profit insurance companies, called sickness funds, are responsible for collecting the contributions and paying physicians and hospitals (Santerre & Neun, 1996, p. 134). In a socialized health insur- ance system, insurance and payment functions are closely integrated, and the financing function is better coordinated with the insurance and payment functions than it is in the United States. Delivery is character- ized by independent private arrangements. The government exercises overall control. Canada Canada’s National Health Insurance system, referred to as Medicare, was initially established in the Medical Care Act of 1966, providing 50/50
- 39. cost sharing for provincial or territorial medical insurance plans. The sys- tem provides universal coverage with free care at the point of contact and is publicly funded through taxes, although it is privately run. Most doctors are private practitioners who are paid fee-for-service and submit service claims directly to the health insurance plan for payment. The federal government is responsible for establishing the constitution that determines how health care is run, whereas provincial and territorial governments administer and deliver heath care services and health insurance plans. In 1984, the addition of the Canadian Health Act solidified and defined five principles and crite- ria for territorial and provincial governments to meet in order to receive full funding for health insurance plans. Care must be (1) available to all eligible residents of Canada, (2) comprehensive in coverage, (3) accessible without financial and other barriers, (4) portable within the country and while trav- eling abroad, and (5) publicly administered. Canada’s health care system relies heavily on primary care physicians, who account for 51% of active physicians in the country. These physicians serve two key functions. First, they provide first contact health care services, and second, they coordinate patient health care services across the system to ensure continuity. Primary
- 40. physicians arrange patient access to specialists, hospital admissions, and diagnostic testing and prescription drug therapy. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 18 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. Health Care Systems of Other Developed Countries 19 Great Britain In Great Britain, universal health coverage is provided by the National Health Service (NHS), which is publicly funded and run, relying on the belief that every citizen is entitled to health care. Through this system, all basic services, visits to primary care physicians and specialists, inpatient care, or x-ray and pathology services are free, whereas other costs are cov- ered by the patient in full or subsidized by the government. Additionally, the purchase of private health insurance is also a choice for individuals with 7 million, or 12%, of the population covered by these plans. The system comes with serious problems that vary in severity across the region involving fund- ing, service, and staff. One of the largest concerns plaguing the NHS is referred to as “health tourism,” which is when individuals go
- 41. into the country to get treated, escaping monetary fees and costing the agency almost £200 million each year. There are also long wait times for care, especially elective procedures, with 41.2% reporting a wait period of 12 or more weeks to see a specialist or receive surgical care, and much of the equipment used is out- dated, as there is little funding directed towards technological innovations. Germany Germany follows the Socialized Health Insurance system with the statutory health insurance (GKV) providing organizational framework for the delivery of public health care. Employees and employers are required to provide 50/50 contributions toward the system if the employed earns below a specific level of income (40,500 Euros per year in 2004). The health plan also covers the spouse and children (until a certain age) of the employee. If income is above the limit, the individual is given a choice between private health insurance or the state insurance. Over 90% of the population is cov- ered by the national health insurance—the remainder is insured privately. Although this system prevents the growth of an uninsured population, it is met with mixed opinions. In 2003, the German health ministry concluded
- 42. that the system suffers from lack of competition, superfluous, insufficient, or inappropriate care, and shrinking revenue, and an aging population. Table 1.1 presents selected features of the national health care pro- grams in Canada, Germany, and Great Britain and compares them with those in the United States. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 19 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 20 Chapter 1 • Major Characteristics of U.S. Health Care Delivery Ta bl e 1. 1 He alt h Ca re
- 58. d re lat ive va lue sc ale . 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 20 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. Systems Framework 21 SYSTEMS FRAMEWORK A system consists of a set of interrelated and interdependent compo- nents designed to achieve some common goals. The components are logi- cally coordinated. Even though the various functional components of the health services delivery structure in the United States are at best only loosely coordinated, the main components can be identified with a systems model. The systems framework used here helps one understand
- 59. that the structure of health care services in the United States is based on some foun- dations, provides a logical arrangement of the various components, and demonstrates a progression from inputs to outputs. The main elements of this arrangement are system inputs (resources), system structure, system processes, and system outputs (outcomes). In addition, system outlook (future directions) is a necessary element of a dynamic system. This sys- tems framework has been used as the conceptual base for organizing later chapters in this book (see Figure 1.2). System Foundations The current health care system is not an accident. Historical, cultural, social, and economic factors explain its current structure. These factors also affect forces that shape new trends and developments and those that impede change. Chapters 2 and 3 provide a discussion of the system foundations. System Resources No mechanism for the delivery of health services can fulfill its primary objective without the necessary human and nonhuman resources. Human resources consist of the various types and categories of workers
- 60. directly engaged in the delivery of health services to patients. Such personnel— including physicians, nurses, dentists, pharmacists, other professionals trained at the doctoral level, and numerous categories of allied health pro- fessionals—usually have direct contact with patients. Numerous ancillary workers, such as those involved in billing and collection, marketing and public relations, and building maintenance, often play an important but indirect supportive role in the delivery of health care. Health care managers are needed to manage and coordinate various types of health care services. This book discusses primarily the personnel engaged in the direct delivery 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 21 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 22 Chapter 1 • Major Characteristics of U.S. Health Care Delivery of health care services (Chapter 4). The nonhuman resources include med- ical technology (Chapter 5) and health services financing (Chapter 6). Resources are closely intertwined with access to health care.
- 61. For instance, in certain rural areas of the United States, access is restricted because of a shortage of certain categories of health professionals. Development and diffusion of technology also determine the caliber of health care to which people may have access. II. SYSTEM RESOURCES Human Resources “Health Care Providers and Professionals” (Chapter 4) Nonhuman Resources “Technology and Its Effect” (Chapter 5) “Financing and Reimbursement Methods” (Chapter 6) IV. SYSTEM OUTCOMES Issues and Concerns “Health Care Cost, Access, and Quality” (Chapter 12) Change and Reform “Policy Issues in Health Care Delivery” (Chapter 13) III. SYSTEM PROCESSES The Continuum of Care “Outpatient Services and Primary Care” (Chapter 7) “Inpatient Facilities and Services”
- 62. (Chapter 8) “Managed Care and Health Networks” (Chapter 9) Special Populations “Long-Term Care Services” (Chapter 10) “Medically Underserved Groups” (Chapter 11) V. SYSTEM OUTLOOK “Health Care Delivery in the Future” (Chapter 14) E N V I R O N M E N T T R E N D S F U T
- 63. U R E I. SYSTEM FOUNDATIONS Cultural Beliefs and Values, Historical Developments “Foundation of US Health Care Delivery” (Chapter 2) “Historical Overview of US Health Care Delivery” (Chapter 3) System Features Figure 1.2 Systems Framework 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 22 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. Systems Framework 23 System Processes The system resources influence the development and change in physi- cal structures, such as hospitals, clinics, and nursing homes. These struc- tures are associated with distinct processes of health services delivery, and the processes are associated with distinct health conditions. Most health care services are delivered in noninstitutional settings, which
- 64. are mainly associated with processes referred to as outpatient care (Chapter 7). Institutional health services (inpatient care) are predominantly associated with acute care hospitals (Chapter 8). Managed care and integrated systems (Chapter 9) represent a fundamental change in the financing (including payment and insurance) and delivery of health care. Even though managed care represents an integration of the resource and process elements of the systems model, it is discussed as a process for the sake of clarity and conti- nuity of the discussions. Special institutional and community- based set- tings have been developed for long-term care (Chapter 10) and mental health (Chapter 11). System Outcomes System outcomes refer to the critical issues and concerns surrounding what the health services system has been able to accomplish, or not accom- plish, in relationship to its primary objective. The primary objective of any health care delivery system is to provide to an entire nation cost-effective health services that meet certain established standards of quality. The previ- ous three elements of the systems model (foundations, resources, and processes) play a critical role in fulfilling this objective.
- 65. Access, cost, and quality are the main outcome criteria for evaluating the success of a health care delivery system (Chapter 12). Issues and concerns regarding these cri- teria trigger broad initiatives for reforming the system through health pol- icy (Chapter 13). System Outlook A dynamic health care system must look forward. In essence, it must project into the future the accomplishment of desired system outcomes in view of anticipated social, cultural, and economic changes. Chapter 14 dis- cusses these future perspectives. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 23 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. 24 Chapter 1 • Major Characteristics of U.S. Health Care Delivery CONCLUSION The United States has a unique system of health care delivery, but the system lacks universal access; therefore, continuous and comprehensive health care is not enjoyed by all Americans. Health care
- 66. delivery in the United States is characterized by a patchwork of subsystems developed either through market forces or the need to take care of certain population segments. These include managed care, the military and VA systems, the system for vulnerable populations, and the emerging IDSs. No country in the world has a perfect system. Most nations with a national health care program have a private sector that varies in size. The systems framework provides an organized approach to an understanding of the various components of the U.S. health care delivery system. REFERENCES Altman, S. H., and U. E. Reinhardt. 1996. Introduction: Where does health care reform go from here? An uncharted odyssey. In S. H. Altman and U. E. Reinhardt (eds.). Strategic Choices for a Changing Health Care System (pp. xxi–xxxii). Chicago: Health Administration Press. Anderson, G. F., et al. 2003. It’s the prices, stupid: Why the United States is so different from other countries. Health Affairs 22 (3):89–105. Aventis Pharmaceuticals. 2002. HMO-PPO Digest: Managed Care Digest Series. Bridgewater, NJ: Aventis Pharmaceuticals. Bureau of Labor Statistics. March 12, 2008. Health Care. U.S.
- 67. Department of Labor. Retrieved July 11, 2008, from http://www.bls.gov/oco/cg/cgs035.htm. Bureau of Primary Health Care. 1999. Primary Care Programs Directory. McLean, VA: National Clearinghouse for Primary Care Information. Bureau of Primary Health Care. 2002. BPHC-UDS Annual Report. Rockville, MD: Bureau of Primary Health Care, Health Resources and Services Administration. National Center for Health Statistics. 2002. Health, United States, 2002. Hyattsville, MD: Department of Health and Human Services. National Center for Health Statistics. 2007. Health, United States, 2007. Hyattsville, MD: Department of Health and Human Services. National Center for Veterans Analysis and Statistics. 2007. FY07 VA Information Pamphlet. Washington, DC: Department of Veterans Affairs. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 24 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. References 25
- 68. Politzer, R. M., et al. 2003. The future role of health centers in improving national health. Journal of Public Health Policy 24 (3):296–306. Santerre, R. E., and S. P. Neun. 1996. Health Economics: Theories, Insights, and Industry Studies. Chicago: Irwin. Shi, L., et al. 2001. The impact of managed care on vulnerable populations served by community health centers. Journal of Ambulatory Care Management 24 (1):51–66. Shortell, S. M., et al. 1996. Remaking health care in America: Building organized delivery systems. Hospital Health Network 70 (6):43–44, 46, 48. U.S. Bureau of the Census. 1998. Statistical Abstract of the United States: 1998, 118th ed. Washington, DC: Bureau of the Census. U.S. Census Bureau. 2007. Current Populations Report (pp. 60– 233). Income, Poverty, and Health Insurance Coverage in the United States: 2006. Washington, DC: Government Printing Office. Wolinsky, F. D. 1988. The Sociology of Health: Principles, Practitioners, and Issues, 2nd ed. Belmont, CA: Wadsworth Publishing Company. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 25 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR
- 69. DISTRIBUTION. 63800_CH01_Final.qxd:Shi 2/9/09 12:54 PM Page 26 © Jones and Bartlett Publishers, LLC. NOT FOR SALE OR DISTRIBUTION. << /ASCII85EncodePages false /AllowTransparency false /AutoPositionEPSFiles true /AutoRotatePages /None /Binding /Left /CalGrayProfile (Dot Gain 20%) /CalRGBProfile (sRGB IEC61966-2.1) /CalCMYKProfile (U.S. Web Coated 050SWOP051 v2) /sRGBProfile (sRGB IEC61966-2.1) /CannotEmbedFontPolicy /Error /CompatibilityLevel 1.4 /CompressObjects /Off /CompressPages true /ConvertImagesToIndexed true /PassThroughJPEGImages false /CreateJDFFile false /CreateJobTicket false /DefaultRenderingIntent /Default /DetectBlends false /DetectCurves 0.1000 /ColorConversionStrategy /LeaveColorUnchanged /DoThumbnails false /EmbedAllFonts true /EmbedOpenType false /ParseICCProfilesInComments true /EmbedJobOptions true
- 70. /DSCReportingLevel 0 /EmitDSCWarnings false /EndPage -1 /ImageMemory 1048576 /LockDistillerParams false /MaxSubsetPct 100 /Optimize false /OPM 1 /ParseDSCComments true /ParseDSCCommentsForDocInfo true /PreserveCopyPage true /PreserveDICMYKValues true /PreserveEPSInfo true /PreserveFlatness true /PreserveHalftoneInfo true /PreserveOPIComments true /PreserveOverprintSettings true /StartPage 1 /SubsetFonts false /TransferFunctionInfo /Preserve /UCRandBGInfo /Preserve /UsePrologue false /ColorSettingsFile (None) /AlwaysEmbed [ true ] /NeverEmbed [ true ] /AntiAliasColorImages false /CropColorImages true /ColorImageMinResolution 300 /ColorImageMinResolutionPolicy /Warning /DownsampleColorImages false /ColorImageDownsampleType /Average /ColorImageResolution 300 /ColorImageDepth 8 /ColorImageMinDownsampleDepth 1
- 71. /ColorImageDownsampleThreshold 1.50000 /EncodeColorImages true /ColorImageFilter /FlateEncode /AutoFilterColorImages false /ColorImageAutoFilterStrategy /JPEG /ColorACSImageDict << /QFactor 0.15 /HSamples [1 1 1 1] /VSamples [1 1 1 1] >> /ColorImageDict << /QFactor 0.15 /HSamples [1 1 1 1] /VSamples [1 1 1 1] >> /JPEG2000ColorACSImageDict << /TileWidth 256 /TileHeight 256 /Quality 30 >> /JPEG2000ColorImageDict << /TileWidth 256 /TileHeight 256 /Quality 30 >> /AntiAliasGrayImages false /CropGrayImages true /GrayImageMinResolution 300 /GrayImageMinResolutionPolicy /OK /DownsampleGrayImages false /GrayImageDownsampleType /Average /GrayImageResolution 300 /GrayImageDepth 8 /GrayImageMinDownsampleDepth 2 /GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true /GrayImageFilter /FlateEncode /AutoFilterGrayImages false
- 72. /GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict << /QFactor 0.15 /HSamples [1 1 1 1] /VSamples [1 1 1 1] >> /GrayImageDict << /QFactor 0.15 /HSamples [1 1 1 1] /VSamples [1 1 1 1] >> /JPEG2000GrayACSImageDict << /TileWidth 256 /TileHeight 256 /Quality 30 >> /JPEG2000GrayImageDict << /TileWidth 256 /TileHeight 256 /Quality 30 >> /AntiAliasMonoImages false /CropMonoImages true /MonoImageMinResolution 1200 /MonoImageMinResolutionPolicy /OK /DownsampleMonoImages false /MonoImageDownsampleType /Average /MonoImageResolution 1200 /MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000 /EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode /MonoImageDict << /K -1 >> /AllowPSXObjects false /CheckCompliance [ /None
- 73. ] /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile (None) /PDFXOutputConditionIdentifier () /PDFXOutputCondition () /PDFXRegistryName () /PDFXTrapped /False /Description << /CHS <FEFF4f7f75288fd94e9b8bbe5b9a521b5efa76840020004100640 06f006200650020005000440046002065876863900275284e8e9a d88d2891cf76845370524d53705237300260a853ef4ee54f7f7528 0020004100630072006f0062006100740020548c0020004100640 06f00620065002000520065006100640065007200200035002e00 3000204ee553ca66f49ad87248672c676562535f00521b5efa7684 00200050004400460020658768633002> /CHT <FEFF4f7f752890194e9b8a2d7f6e5efa7acb76840020004100640 06f006200650020005000440046002065874ef69069752865bc9a
- 77. 0bb38c11cb97c0020c791c131d569b2c8b2e4002e0020c774b807a c8c0020c791c131b41c00200050004400460020bb38c11cb29400 20004100630072006f0062006100740020bc0f002000410064006f 00620065002000520065006100640065007200200035002e00300 020c774c0c1c5d0c11c0020c5f40020c2180020c788c2b5b2c8b2e 4002e> /NLD (Gebruik deze instellingen om Adobe PDF-documenten te maken die zijn geoptimaliseerd voor prepress-afdrukken van hoge kwaliteit. De gemaakte PDF-documenten kunnen worden geopend met Acrobat en Adobe Reader 5.0 en hoger.) /NOR <FEFF004200720075006b0020006400690073007300650020006 9006e006e007300740069006c006c0069006e00670065006e0065 002000740069006c002000e50020006f007000700072006500740 0740065002000410064006f006200650020005000440046002d00 64006f006b0075006d0065006e00740065007200200073006f006 d00200065007200200062006500730074002000650067006e0065 007400200066006f00720020006600f80072007400720079006b0 06b0073007500740073006b007200690066007400200061007600 20006800f800790020006b00760061006c0069007400650074002 e0020005000440046002d0064006f006b0075006d0065006e0074 0065006e00650020006b0061006e002000e50070006e006500730 02000690020004100630072006f00620061007400200065006c00 6c00650072002000410064006f006200650020005200650061006 40065007200200035002e003000200065006c006c006500720020 00730065006e006500720065002e> /PTB <FEFF005500740069006c0069007a00650020006500730073006 1007300200063006f006e00660069006700750072006100e700f5 0065007300200064006500200066006f0072006d0061002000610 0200063007200690061007200200064006f00630075006d006500 6e0074006f0073002000410064006f00620065002000500044004 60020006d00610069007300200061006400650071007500610064 006f00730020007000610072006100200070007200e9002d00690 06d0070007200650073007300f500650073002000640065002000 61006c007400610020007100750061006c0069006400610064006
- 79. 005000440046002d0064006f006b0075006d0065006e007400200 06b0061006e002000f600700070006e0061007300200069002000 4100630072006f0062006100740020006f0063006800200041006 4006f00620065002000520065006100640065007200200035002e 00300020006f00630068002000730065006e006100720065002e> /ENU (Use these settings to create Adobe PDF documents best suited for high-quality prepress printing. Created PDF documents can be opened with Acrobat and Adobe Reader 5.0 and later.) >> /Namespace [ (Adobe) (Common) (1.0) ] /OtherNamespaces [ << /AsReaderSpreads false /CropImagesToFrames true /ErrorControl /WarnAndContinue /FlattenerIgnoreSpreadOverrides false /IncludeGuidesGrids false /IncludeNonPrinting false /IncludeSlug false /Namespace [ (Adobe) (InDesign) (4.0) ] /OmitPlacedBitmaps false /OmitPlacedEPS false /OmitPlacedPDF false /SimulateOverprint /Legacy >> << /AddBleedMarks false
- 80. /AddColorBars false /AddCropMarks false /AddPageInfo false /AddRegMarks false /ConvertColors /ConvertToCMYK /DestinationProfileName () /DestinationProfileSelector /DocumentCMYK /Downsample16BitImages true /FlattenerPreset << /PresetSelector /MediumResolution >> /FormElements false /GenerateStructure false /IncludeBookmarks false /IncludeHyperlinks false /IncludeInteractive false /IncludeLayers false /IncludeProfiles false /MultimediaHandling /UseObjectSettings /Namespace [ (Adobe) (CreativeSuite) (2.0) ] /PDFXOutputIntentProfileSelector /DocumentCMYK /PreserveEditing true /UntaggedCMYKHandling /LeaveUntagged /UntaggedRGBHandling /UseDocumentProfile /UseDocumentBleed false >> ] >> setdistillerparams << /HWResolution [2400 2400] /PageSize [504.000 720.000] >> setpagedevice
- 81. Faculty Contact Cary Stanger [email protected] Course Description Prerequisite: A writing course. Recommended: WRTG 291. An investigation of U.S. history from the end of World War II to the events of September 11, 2001. The goal is to identify events, individuals, movements, and technological developments; synthesize primary and secondary resources; and analyze the significance of social, cultural, and political events. Topics include social turmoil, the Cultural Revolution, the role of the United States in the world, economic trends, military conflicts, consumerism, political and public scandals, and globalization. Course Introduction World War II profoundly changed the United States. It contributed to ending the Great Depression and made the United States a global power with worldwide interests and commitments. This course investigates the United States during its development into a prosperous and powerful nation in the years following 1945. Issues such as the cold war, Vietnam, and the civil rights movement will be addressed with both primary and secondary source readings. Course Outcomes After completing this course, you should be able to • identify key events, individuals, movements, and technological developments to formulate and effectively communicate an integrated historical perspective
- 82. • synthesize multi-modal primary and secondary resources to articulate the complexity of historical concepts and viewpoints • comprehend and evaluate the significance of historical context to interpret the development of the United States in the post-World War II era • comprehend and analyze the significance of the social, cultural, and political events of the post-World War II era in the United States to interpret current issues Course Materials Click to access your course materials information (http://webapps.umuc.edu/UgcmBook/BPage.cfm? C=HIST%20365&S=6380&Sem=2188) Grading Information You are responsible for the following graded items: Weekly Discussions 35% University of Maryland University College • Adelphi • Syllabus • HIST 365 6380 RECENT AMERICA: 1945 TO THE PRESENT (2188) HIST-365 Fall 2018 Section 6380 3 Credits 08/20/2018 to 10/14/2018
- 83. http://webapps.umuc.edu/UgcmBook/BPage.cfm?C=HIST 365&S=6380&Sem=2188 Research Project - Paper Topic & Proposal 10% Research Project - Annotated Bibliography 20% Research Project - Final Paper 35% TOTAL 100% Late Policy - No late work will be accepted in this class. Extra Credit Policy - No extra credit will be offered in this class. Please note: Submitting proof of successful completion of the plagiarism prevention tutorial no later than the first week of the term (23:59 E.S.T. Saturday August 25th) will entitle you to a bonus point. That will result in your calculated grade being advanced a single point in your adjusted grade total which is often enough to result in a letter grade change. Credit will not be retroactive. Project Descriptions I. Discussion Participation (35% of final grade) - See schedule of assignments There will be weekly discussions except for the final week of
- 84. the semester. Each discussions takes place in two parts, a preliminary response in the form of a coherent, integrated essay of one to two typed pages taking into account all facets of the discussion question. Remember to write a literate, documented essay. Bullet point memorandum will be denied all credit. History takes into account evidence from multiple sources and reflects evidence of different points of view. Your initial response is due no later than Wednesday at 23:59 E.S.T. and your follow up posting is due no later than Saturday at 23:59 E.S.T. On Thursday, I award three points for timely completion of part I. On Sunday I add the two final points for providing a response to a previous posting by any member of the class. This prevents adding two simultaneous postings at the end of the week. To complete this class successfully, students are expected to be engaged on an ongoing basis. Each completed discussion is valued at up to five points. II. Research Project (65% of final grade) The research paper assignment makes up a total of 65% of the final grade and consists of three sections: topic/thesis, annotated bibliography, and final paper. Each section of this assignment builds on the previous ones and will assist you in completing the final paper which is to be submitted by the end of week 8 in place of a final examination. A. Paper Topic and Proposal (10% of final grade) - Due Week 2 With written approval from the instructor, select a topic from within the historical parameters of this course (the United States during the period of 1945 to 2001) that is relevant
- 85. to the course outcomes. During the first week of the term you should send an individual e-message indicating the topic you are interested in. Your topic cannot be too broad such as the Vietnam War. Approval will assist you to define a manageable but original research topic. Without written authorization, anything subsequently submitted will not receive credit. You will perform preliminary research and create a working thesis statement with the understanding that it may be slightly modified later in the research process. Your topic/thesis is due by the end of week 2 and must show that you've done some preliminary research. A proposal is tantamount to a thesis is what you intend to prove or disprove by your research. It is not a recitation of events but a meaningful analysis. The proposal must be in the form of a written statement from which it is clearly evident that you have begun your research and developed a framework for the entire project. Do not provide this in outline form. Historians are devoted to lucid articulation, not scanning a column of numbers or crossword puzzle clues. B. Annotated Bibliography (20% of final grade) - Due Week 5 Write an annotated bibliography. This will list and describe a minimum of 10 primary and secondary sources, with specific requirements detailed below, that you may use in your paper.
- 86. The annotated bibliography should involve a variety of primary and secondary sources, including at least two primary sources and articles from at least two academic journals; it should not include encyclopedias of any kind, printed or electronic (especially including Wikipedia), dictionaries, or non-professional websites. A non-professional web site includes commercial information or information designed for a general public. Government depositories and academic journals (check the UMUC library web page) are expected in all circumstances. Each annotation should include a full, properly formatted Chicago style citation, 1-2 paragraphs detailing the basic argument of the work, the type of evidence used to prove the thesis, and an explanation of the value of the information to your paper. Professional historians always utilize the University of Chicago graduate school citation standards first associated with Kate Turabian (A Manual for Writers...) This very detailed form of documenting research enables the whoever reads your work can find the exact reference(s) upon which your original conclusions are based. You can type Chicago style citation into your url and numerous websites will provide information and examples. C. Final Paper (35% of final grade) - Due Week 8 Submit a finished paper that includes a title page, endnotes pages (if used) and bibliography (without annotations). This paper will be 7-8 double-spaced pages (excluding the title page, endnotes pages, and the bibliography), with one-inch margins, times new roman font size 12, and either footnotes or endnotes (Chicago Style). Do not use parenthetical notes. If you're not sure about what this means, ask your
- 87. instructor. The finished paper will use both primary and secondary sources to increase the plausibility of the clearly stated, analytical thesis. It will be carefully structured, composed, and proofread, with all required components included in the correct order. You need a minimum of 7 sources to be eligible for a grade of C; 10 sources to be eligible for an A. Note the specific requirements for primary and secondary sources. Please note that the History Department places great importance on individual research in upper level classes. There is no final examination. Your term project takes the place of a final examination and is due no later than Sunday October 14, 2018 at 23:59 E.S.T. Academic Policies Academic Policies and Guidelines ACADEMIC INTEGRITY As a member of the University of Maryland University College (UMUC) academic community that honors integrity and respect for others you are expected to maintain a high level of personal integrity in your academic work at all times. Your work should be original and must not be reused in other courses. CLASSROOM CIVILITY Students are expected to work together cooperatively, and treat fellow students and faculty with respect, showing professionalism and courtesy in all interactions. Please review the Code of Civility for more guidance on interacting in UMUC classrooms:
- 88. https://www.umuc.edu/students/support/studentlife/conduct/cod e.cfm (https://www.umuc.edu/students/support/studentlife/conduct/cod e.cfm). POLICIES AND PROCEDURES https://www.umuc.edu/students/support/studentlife/conduct/cod e.cfm UMUC is committed to ensuring that all individuals are treated equally according to Policy 040.30 Affirmative Action, Equal Opportunity, and Sexual Harassment (https://www.umuc.edu/policies/adminpolicies/admin04030.cfm ). Students with disabilities who need accommodations in a course are encouraged to contact the Office of Accessibility Services (OAS) at [email protected] (mailto:[email protected]), or call 800-888-UMUC (8682) or 240-684-2287. The following academic policies and procedures apply to this course and your studies at UMUC. 150.25 Academic Dishonesty and Plagiarism (https://www.umuc.edu/policies/academicpolicies/aa15025.cfm) – UMUC defines academic dishonesty as the failure to maintain academic integrity. All charges of academic dishonesty will be brought in accordance with this Policy. Note: In this course, your instructor has access to use Turnitin.com, a tool that helps to evaluate the originality of student work. Your instructor may use Turnitin or other resources to check the authenticity of your work and the accuracy of your
- 89. use of sources. To learn more about Turnitin, the feedback it provides, and your options regarding the storage of your work in the Turnitin database go to the UMUC guides at umuc.edu/library/libresources/turnitin- students.cfm (https://www.umuc.edu/library/libresources/turnitin.cfm) and http://sites.umuc.edu/library/libresources/turnitin.cfm#studentco pyright (http://sites.umuc.edu/library/libresources/turnitin.cfm). If you have questions about academic integrity or how to cite your sources go to the UMUC Academic Integrity Resources page at http://www.umuc.edu/current-students/learning- resources/academic-integrity/resources.cfm (http://www.umuc.edu/current-%20students/learning- resources/academic- integrity/resources.cfm). 151.00 Code of Student Conduct (https://www.umuc.edu/policies/studentpolicies/stud15100.cfm) 170.40 170.41 170.42 The following policies describe the requirements for the award of each degree: Degree Completion Requirements for the Graduate School (https://www.umuc.edu/policies/academicpolicies/aa17040.cfm) Degree Completion Requirements for a Bachelor’s Degree (https://www.umuc.edu/policies/academicpolicies/aa17041.cfm) Degree Completion Requirements for an Associate’s Degree (https://www.umuc.edu/policies/academicpolicies/aa17042.cfm) 170.71 Policy on Grade of Incomplete
- 90. (https://www.umuc.edu/policies/academicpolicies/aa17071.cfm) - The mark of I is exceptional and considered only for certain courses. Students who have completed 60% of their coursework with a grade of B or better for graduate courses or C or better for undergraduate courses and request an I before the end of the term. The mark of I is not available for noncredit courses. 170.72 Course Withdrawal Policy (https://www.umuc.edu/policies/academicpolicies/aa17072.cfm) - Students must follow drop and withdrawal procedures and deadlines available at https://www.umuc.edu/ (https://www.umuc.edu/) under Academic Calendar. 130.80 Procedures for Review of Alleged Arbitrary and Capricious Grading (https://www.umuc.edu/policies/academicpolicies/aa13080.cfm) – appeals may be made on final course grades as described herein. 205.06 Calculation Of Grade-Point Average (GPA) for Inclusion on Transcripts and Transcript Requests (https://www.umuc.edu/policies/academicpolicies/aa20506.cfm) – Note: Undergraduate and Graduate Schools have different Grading Policies (i.e. The Graduate School does not award the grade of D). See Course Syllabus for Grading Policies. https://www.umuc.edu/policies/adminpolicies/admin04030.cfm mailto:[email protected] https://www.umuc.edu/policies/academicpolicies/aa15025.cfm https://www.umuc.edu/library/libresources/turnitin.cfm http://sites.umuc.edu/library/libresources/turnitin.cfm
- 91. http://www.umuc.edu/current- students/learning- resources/academic-integrity/resources.cfm https://www.umuc.edu/policies/studentpolicies/stud15100.cfm https://www.umuc.edu/policies/academicpolicies/aa17040.cfm https://www.umuc.edu/policies/academicpolicies/aa17041.cfm https://www.umuc.edu/policies/academicpolicies/aa17042.cfm https://www.umuc.edu/policies/academicpolicies/aa17071.cfm https://www.umuc.edu/policies/academicpolicies/aa17072.cfm https://www.umuc.edu/ https://www.umuc.edu/policies/academicpolicies/aa13080.cfm https://www.umuc.edu/policies/academicpolicies/aa20506.cfm GRADING According to UMUC’s grading policy, the following marks are used: Undergraduate Graduate A 90-100 90-100 B 80-89 80-89 C 70-79 70-79* D 60-69 N/A** F 59 or below 69 or below FN Failure-Non attendance Failure-Non attendance G Grade Pending Grade Pending P Passing Passing S Satisfactory Satisfactory U Unsatisfactory Unsatisfactory I Incomplete Incomplete
- 92. AU Audit Audit W Withdrew Withdrew * The grade of "B" represents the benchmark for The Graduate School. Students must maintain a Grade Point Average (GPA) of 3.0 or higher. Classes where final grade of C or F places a student on Academic Probation must be repeated. ** The Graduate School does not award the grade of D. COURSE EVALUATION SURVEY UMUC values its students' feedback. You will be asked to complete an online evaluation toward the end of the term. The primary purpose of this evaluation process is to assess the effectiveness of classroom instruction in order to provide the best learning experience possible and make continuous improvements to every class. Responses are kept confidential. Please take full advantage of this opportunity to provide your feedback. LIBRARY SUPPORT Extensive library resources and services are available online, 24 hours a day, seven days a week at https://www.umuc.edu/library/index.cfm (https://www.umuc.edu/library/index.cfm) to support you in your studies. The UMUC Library provides research assistance in creating search strategies, selecting relevant databases, and evaluating and citing resources in a variety of formats via its Ask a Librarian service at https://www.umuc.edu/library/libask/index.cfm (https://www.umuc.edu/library/libask/index.cfm). EXTERNAL LINK DISCLAIMER This course may contain links to external sites neither owned
- 93. nor maintained by UMUC. UMUC bears no responsibility for the accuracy, legality, or content of external sites or for that of subsequent links. In addition, the terms of use, security policies, and privacy policies may differ from those of UMUC. Contact the external site for answers to questions regarding its content, terms of use, and policies. LEARNING MANAGEMENT SYSTEM SUPPORT To successfully navigate the online classroom new students are encouraged to view the Classroom Walkthrough under Help in the upper right menu of the LEO classroom. Those requiring technical assistance can access [email protected] Support directly in LEO under the Help menu. Additional technical support is available 24 hours a day, seven days a week via self-help and live chat at https://www.umuc.edu/help (https://www.umuc.edu/help) or by phone toll-free at 888-360- UMUC (8682). https://www.umuc.edu/library/index.cfm https://www.umuc.edu/library/libask/index.cfm https://www.umuc.edu/help SYLLABUS CHANGES All items on this syllabus are subject to change at the discretion of the Instructor and the Office of Academic Affairs. Class & Assignment Schedule Students can access their complete list of assignments and their corresponding due dates within the Assignments section of the classroom by navigating to the Assignments section of the class from the main
- 94. navigation bar. Follow the link below, and then click Assignments, for a video demonstration on how to utilize this feature. Classroom Walkthrough Videos Link (http://www.umuc.edu/students/leo/videos.cfm) Students also have access to a calendar tool on the course homepage within the classroom. Class Schedule Important Note: Except for the final term project which takes the place of a comprehensive examination, all assignments are due Wednesday and Saturday at 11:59 E.S.T. For those not accustomed to the global clock, 11:59 PM is equivalent to 23:59 PM. The final term project will be due on Sunday, October 14th at 23:59 E.S.T. Week/Dates Assignments Due Date Week 1 8/20-8/25 Topic: WWII to Cold War Read: Week 1 Learning Resources Do: Week 1 Discussion Submit individual e-mail message to instructor defining topic for research project Saturday, 8/25 at 11:59 pm ET Week 2 8/26-9/1
- 95. Topic: 1950s - Domestic & Foreign Policy Issues Read: Week 2 Learning Resources Do: Week 2 Discussion Research Project - Paper Topic & Proposal due Saturday, 9/1 at 11:59 pm ET Week 3 9/2-9/8 Topic: 1960s - Kennedy/Johnson Read: Week 3 Learning Resources Do: Week 3 Discussion Saturday 9/8 at 11:59 pm ET Week 4 9/9-9/15 Topic: Vietnam/Civil Rights Read: Week 4 Learning Resources Do: Week 4 Discussion Saturday 9/15 at 11:59 pm ET Week 5 9/16-9/22
- 96. Topic: 1970s - Nixon, Ford, and Carter Read: Week 5 Learning Resources Research Project - Annotated Bibliography due Saturday 9/22 at 11:59 pm ET http://www.umuc.edu/students/leo/videos.cfm Week 6 9/23-9/29 Topic: 1980s - Reagan/Bush Read: Week 6 Learning Resources Do: Week 6 Discussion Saturday, 9/29 at 11:59 pm ET Week 7 9/30-10/6 Topic: 1990s - Clinton Read: Week 7 Learning Resources Do: Week 7 Discussion Saturday, 10/6 at 11:59 pm ET
- 97. Week 8 10/7-10/14 Topic: 2001 to present Read: Week 8 Learning Resources Research Project - Final Paper due Sunday, 10/14 at 11:59 pm ET HIST 365 6380 Recent America: 1945 to the Present (2188) HIST-365Faculty ContactCourse DescriptionCourse IntroductionCourse OutcomesCourse MaterialsGrading InformationProject DescriptionsAcademic PoliciesClass & Assignment Schedule Name: Adedotun Adereti Course : HIIT 102 Date: September 14, 2018
- 98. The healthcare delivery system in the United States is unique and complex, when compared to other developed countries that has national healthcare for their citizens. In these countries, the government provides the citizens with access to routine and basic health care (Shi, 2019) while that is not available in the U.S. There are so many factors that influence the U.S healthcare delivery system, some of these factors are political climate, stage of economy development, technological advancement, social and cultural influence. There are major characteristics of the U.S healthcare delivery system which are as follows; No central governing agency and little integration and coordination The healthcare system in the United states is complex because there is no centralized control system. Lack of centralization in the United states health care system makes health care to be expensive as it can not be managed by global budget. Due to the large private sector involvement in the US health care system, most of the Doctor’s office and hospitals are privately owned and independent of the government. The federal and state government have huge impact in the US healthcare delivery system, public sector expenses and reimbursement for Medicaid and Medicare patients are determined by both federal and state government. In contrast to the US healthcare system, other developed countries have a centralized Healthcare system that makes financing and delivery of health care available to all citizens. Technology-driven delivery system focusing on acute care The United States has been the most advanced in medical technology. Progress in science and technology generates a demand for new services though there is a shrink in the resources to finance healthcare (Shi, 2019). There are other factors that contributes to increase in the demand for expensive care in the US health care system; Some patients believe that modern technologies offer better care, some physician office
- 99. would want to try new technology and some medical institution like hospital believe that having the latest technology allows them to compete in the healthcare market. These factors hike up the cost of care because hospitals, physician office are now pressured to recover the capital invested in obtaining the technologies thereby leading to increase in the cost of healthcare. Advance medical technology has ushered in new and successful medical interventions but there are consequences linked to these advanced technologies being over used. For instance, the high cost of medical intervention has caused inflation in the cost of healthcare, which has made it difficult for employers to offer part-time workers insurance benefit (Shi, 2019). High on Cost, Unequal in Access, and Average in Outcome The United States spend 13% of gross domestic product (GDP) on healthcare which is mostly medical care which is not the case in other developed countries. Not everyone in the US has access to healthcare when in need of preventive care. Healthcare is only available to those who have health care benefits through their employers, covered by government healthcare programs such as Medicaid and Medicare, those who can afford to pay out of personal funds and those who can pay for the care and services they obtained. The only way to get access to healthcare is by buying an health insurance out of pocket or getting one through your employer and this leads to the high cost of healthcare, uninsured people do not have access to routine and basic care which is also known as primary care except they pay the fee charged by the physician and those that cannot afford it, have to wait till the health challenges gets worse at which point they can obtain free care. In the absence of insurance, patients are unable to receive adequate care that is needed which has led to increase in mortality rate in the US, though the US is one of the most advanced economies, they are behind in the healthcare provided for her citizens. (Shi, 2019) Imperfect Market Condition: The US healthcare delivery is mostly in private hands but is
- 100. partially governed by free market forces (Shi, 2019). There are key characteristics of a free market which prove that the US healthcare market is not free.In a freemarket, many patient (buyers) and providers(sellers) act autonomously, Patient should be able to choose their provider with price and services rendered being the determinant. For free healthcare market, there must be unrestricted competition among providers based on their prices and the quality service they render. Free market works well when information about care services and products are made available to patients which is not the case in the US; Patient don’t have information about other expense that comes with the care obtained. For instance, the of recovery care and anesthesiology is not made available to patient who is about to undergo a procedure. Government as Subsidiary to the private Sector: In the US health care market, the private sector dominates unlike other countries where government provides the health care for residents. The gaps left opened by the private sector in the US healthcare market is covered up by the government. (Shi, 2019) Market Justice versus Social Justice: Conflict throughout Health Care There are two opposite theories that controls production and distribution of health care in the US. The market justice’s principle puts the responsibility of reasonable distribution of health care on market forces in a free market (Shi, 2019). In market justice, medical care and its benefit are made available based on the ability of people to pay out of their personal funds. In the just distribution principle, the distribution of health care is based on the need of the health care not the ability to pay. Multiple Players and Balance of power There are numerous key players in the healthcare system of the United States. Insurance companies, labor, physicians, big businesses and hospital consist of the powerful group that are represented by high price lobbyist before law makers. Conflicts arises when interest of each player contradicts the other. For