
Recommended
Recommended
More Related Content
Similar to Crime Scene Investigations Workgroup Chair Major Susan .docx
Similar to Crime Scene Investigations Workgroup Chair Major Susan .docx (20)
More from vanesaburnand
More from vanesaburnand (20)
Recently uploaded
Recently uploaded (20)
Crime Scene Investigations Workgroup Chair Major Susan .docx
- 1. Crime Scene Investigations Workgroup Chair Major Susan Barker, Miami-Dade Police MDPD Bomb Squad FBI Hazardous Material Response Unit Jackson Memorial Hospital Trauma Unit Miami PD Crime Scene Section
- 2. Broward County SO Crime Scene Bureau MDPD Crime Lab Miami-Dade Fire Rescue Urban Search & Rescue Fla Nat. Guard 44th Civil Support Team Miami-Dade Medical Examiner’s Office
- 3. Module 4 - SLP DISTRIBUTIVE JUSTICE The goal of the Session Long Project is to identify and evaluate the ethical principles used in resolving ethical dilemmas, and to apply the principles to specific ethical issues that may have professional, sociological, economic, legal or political implications. Often times a patient needs a lot of resources prior to being discharged from the hospital. Some organizations use discharge planners or case managers to aid in acquiring these resources. The topic of this SLP is about Jenna, a young woman who could not be discharged home until the issue of resources to care for her was resolved. This story demonstrates that resource allocation decision making is inherently complex, a process that is dynamic, multidimensional, and iterative. After reading the article, "The relational nature of case manager resource allocation decision making: An illustrated case" by Fraser, Estabrooks, and Strang and doing additional research, please respond to the questions listed below: 1. Provide a brief summary of Jenna's case. What was her medical condition? What was her prognosis? Why was it important for her to go home? Did she get to go home? If so, how did that impact her recovery? 2. What were the resources that Jenna needed to go home? What barriers did her case manager encounter in acquiring these resources? 3. Discuss the theory of relational ethics as it applies to this case. What is it? How does it impact the allocation of resources? Think about your own discipline of study, how does this theory apply to acquiring scare resources? Provide an example. 4. Based on what you have read about this case and resource allocation, do you agree with the statement "that resource allocation decision making is inherently complex, a process that is dynamic, multidimensional, and iterative"? Why or why not? What are your views on the fairness of the process? Was it done
- 4. in a fair manner in this case? Did Jenna get preferential treatment because of her case manager? If there was no one advocating for her, what do you think the outcome would have been? SLP Assignment Expectations 1. You will be expected to provide a scholarly basis for your response. 2. Your opinions must be justified with evidence from the literature. 3. References should be cited properly in the text of your essay (either in parentheses or as footnotes), as well as at the end. 4. Several (3-5) scholarly references should be cited for this assignment. 5. Please limit your response to 3 pages maximum, not including title and reference pages. 6. Be sure to apply critical thinking skills to your assignment write-up. Your paper will be evaluated based on the rubric criteria. Please be sure to provide citations of sources consulted in preparing your paper in the body of the actual document itself (i.e. in addition to furnishing a reference list). Remember, any statement that you make that is not common knowledge or that originates from your synthesis or interpretation of materials you have read must have a citation associated with it. For guidelines on in-text citations, visit the following web site: http://owl.english.purdue.edu/handouts/research/r_apa.html Module 4 - Case DISTRIBUTIVE JUSTICE Case Assignment One of the most difficult dilemmas to resolve relates to the allocation of valuable, but scarce resources. Setting standards by which resources are allocated is not an easy task. We hear about patients every day that don't make it because there aren't enough organs for those on the list. Please read the article:
- 5. History of deceased organ donation, transplantation, and organ procurement organizations by Howard, Cornell, and Cochran. After reading the article and doing additional research, please respond to the following questions. 1. Discuss some of the earliest examples of transplantation. Do you think these early experiments made it easier for it to become so commonplace today? What lessons can we learn from the early pioneers? 2. Discuss the process of using organs from deceased patients. What are at least two ethical principles that apply to this process? Be sure to address distributive justice as one of your choices. What are the ethical issues that may arise? What are some instances where the dead donor rule has been violated? 3. Briefly discuss the origins of organ procurement organizations (OPO). What role do they play in organ donations? What ethical issues do you see with these organizations? What are the rules and regulations that govern these organizations? 4. We tend to think of organ transplantation as pertaining to healthcare alone. Provide some examples of how your specific discipline might impact some aspect of organ donation. For example, how might a public health agency impact the process or rules and regulations for organ donation? Use the information in the modular background readings as well as resources you find through ProQuest or other online sources. Please be sure to cite all sources and provide a reference list at the end of the paper. Submit the paper as a WORD document through the link provided for the assignment. Assignment Expectations 1. Discuss Mr. Krampitz's case from the perspective of distributive justice and the allocation of scarce resources. 2. Limit your responses to three pages, not including title and reference pages. 3. Be sure to incorporate module and course concepts into your discussion. 4. Be sure to apply critical thinking skills in your write-up.
- 6. 5. Provide several (3-5) scholarly references to support your discussions and be certain to properly cite all references. Please be sure to provide citations of sources consulted in preparing your paper in the body of the actual document itself (i.e. in addition to furnishing a reference list). Remember, any statement that you make that is not common knowledge or that originates from your synthesis or interpretation of materials you have read must have a citation associated with it. For guidelines on in-text citations, visit the following web site: http://owl.english.purdue.edu/handouts/research/r_apa.html Your paper will be evaluated based on the following criteria. Ethics Mod 4 discussion Ethics and Organ Transplantation Actions for 'Ethics and Organ Transplantation' Previous Next Hide Description Your comments will be graded on how well they meet the Discussion Requirements posted under “Before You Begin.” The rationing of scarce healthcare resources is a subject that is both politically sensitive and raises a number of ethical dilemmas for those charged with making treatment decisions. The ethical dilemma is health care is how to balance the precepts of autonomy, beneficence, and distributive justice. Rationing may affect 3 dimensions of coverage: the share of the population covered; the services covered; and the extent to which services are covered (Teutsch & Rechel, 2012). The U.S. spends 50% more per capita on health care than any other country while achieving worse health than many (Teutsch & Rechel, 2012). Poorly coordinated insurance mechanisms leave 19% of the population uninsured (Teutsch & Rechel, 2012). Until passage of the Patient Protection and Affordable Care Act (PPACA) in 2010, health care was effectively a privilege, not a right (Teutsch & Rechel, 2012). While PPACA seeks to rectify
- 7. this, by 2019 five percent of non-elderly U.S. residents will likely remain uninsured (Tuetsch & Rechel, 2012). There are some who believe the U.S. healthcare system is broken and in desperate need of a radical change—the very change that the passage of the ACA represents. It could be argued that the ACA will only worsen the rationing of healthcare services in the United States. What is your position on this matter? Is the rationing of healthcare a bad thing or a necessary action? What ethical dilemmas might be associated with the rationing of healthcare services and how could they be effectively addressed? Please support your positions/arguments with credible evidence. Reference Teutsch, S. & Rechel, B. (2012). Ethics of resource allocation and rationing medical care in a time of fiscal restraint – U.S. and Europe. Public Health Review, 34(1). Module 4 - Home DISTRIBUTIVE JUSTICE Modular Learning Outcomes Upon successful completion of this module, the student will be able to satisfy the following outcomes: · Case · Discuss the ethical issues related to healthcare rationing and organ transplantation. · Identify and discuss the origins of organ procurement organizations (OPOs). · Discuss the early beginnings of transplantation and lessons learned. · SLP · Examine and resolve ethical dilemmas related to resource allocation. · Discuss the theory of relational ethics as it relates to resource allocation. · Discussion
- 8. · Discuss ethical dimensions of resource allocation and rationing in healthcare. What ethical guidelines should influence resource allocation in healthcare? Module Overview Rationing According to Chris Hackler, in health care, we see rationing in one of three practices: · Limit the amount money spent on health care is an example of the allocation of financial resources; · Distribution of scarce organs for transplantation is an example of the distribution of scarce goods; and · The practice of triage in the emergency room is an example of prioritizing services. Managed Care and Rationing While the managed care concept has been around since the early 1900s, it wasn't until the Nixon administration that we saw the birth of the HMO and proliferation of "managed care." As you are well aware, Managed Care is a financing philosophy that emphasizes the cost effective delivery of health care. This approach to health care delivery has raised a number of ethical questions, one of which is whether managed care organizations (MCO) ration health care services due to the costs of such care, and the obligation and desire to be profitable. This approach has placed providers in the unenviable position of gatekeepers. Providers are required to consider the costs of health care services being recommended; specially, in Health Maintenance Organizations where the providers receive annual bonuses based on the savings they created during the year by not referring patients to specialists and/or specialty care. The effect of these bonus arrangements has been obvious. There is a built in incentive to under-treat or limit care. Also, the providers have been prevented from acting as advocates for their patients; instead, they are agents for the MCOs. Organ Transplantation According to the United Network of Organ Sharing (UNOS), every 14 minutes a new name is added to the transplant waiting
- 9. list. Although the number of issues are great, the number one issue related to organ transplantation is the shortage of organ donors. The implications become clear when one recognizes that there simply are insufficient number of donors and organs to effectively treat those in need. In America, organ donations are made through a volunteer system. While pre-mortem donation is legally accepted in the United States, family members of a potential donor are always asked for permission before organs are removed. In many countries, "presumed consent" is the accepted practice. With presumed consent, physicians and hospitals remove and transplant needed organs unless the decedent has expressly objected prior to his death. As technology advances and medicine obtains better results from certain transplant procedures, ethical issues arise in the context of transplantation for patients with histories of drug or alcohol abuse. For example, should a recovering alcoholic receive a liver transplant? Should a smoker receive a lung transplant? Should an obese patient receive a heart transplant? Take a look at the assigned readings and let see if we can answer some of the questions raised. Please click on this link for a news report regarding a Dutch reality program involving a kidney donation:http://www.usatoday.com/life/television/2007-06-01- kidneys_N.htm PSDA - The Patient Self Determination Act of 1991 requires health care organizations receiving federal money (Medicare or Medicaid) to inform their in-patients, in writing, about their rights to make health care decisions including the right to accept or refuse proposed treatment and the right to complete state permitted "advance directives." As medical technology advances and improves, and patients gain a better understanding of their rights, patients and families have and continue to insist on receiving life-sustaining treatment that may be considered as "futile" by health care professionals.
- 10. FUTILITY - According to Charles Weijer (Medical Futility, 1999) the term medical futility was coined in 1990 as a response to demands by patients and families for treatment thought to be inappropriate. Medical Futility is a professional judgment that takes precedence over the patient's self-determination and autonomous rights. Some define "medical futility" as a medical determination that a therapy or treatment is of no value to a patient and consequently should not be prescribed or provided. It has been argued that treatments that merely preserve permanent unconsciousness or that cannot end dependence on intensive medical care should be considered as futile. (L. J. Schneiderman, "Medical Futility: Its meaning and Ethical Implications", 1990) Some health care providers view "futility" as legal practitioners and scholars view pornography: They may not be able to define it but they know it when they see it. Jacobellis v. State of Ohio (1964) Cardio-Pulmonary Resuscitation and Do Not Resuscitate We see futility raised in cases involving Cardio-Pulmonary Resuscitation and Do Not Resuscitate orders. CPR was originally intended for use in cases involving reversible cardiac arrests. The current practice appears to be the use of CPR in all cases unless there is a contrary order. DNR was intended to avoid aggressive attempts to revive patients where death was anticipated and inevitable. Patients and families; however, have demanded that CPR be performed at all times, even when health care providers believe it to be futile. Research of the PSDA will lead to the conclusion that Cardiopulmonary resuscitation and emergency cardiac care are meant to reverse premature death. They should restore the process of living, not prolong the process of dying. When people reach the end of life, continued resuscitative efforts are inappropriate, futile, undignified and demeaning to both the patient and the rescuers. Persistent Vegetative State (PVS)
- 11. The question of futility is also raised in cases involving patients in a persistent vegetative state (PVS). These patients receive treatment that is effective, but does nothing more than "maintain" a patient in PVS. As mentioned in module one, bioethics was placed on the map with the Karen Ann Quinlan case, where the parents of a young woman in a drug induced coma sought termination of life-support treatment. The Quinlan case initiated discussions about when to stop treatment. What if the patient or family members have unrealistic expectations and demands with respect to treatment? Where patient and family cultural and religious beliefs demand continued or discontinued treatment, the physician's ethical obligations are clearly invoked. Module 4 - Background DISTRIBUTIVE JUSTICE Required Reading Delmonico, F. L., Domínguez-Gil, B., Matesanz, R., & Noel, L. (2011). Organ transplantation 1: A call for government accountability to achieve national self-sufficiency in organ donation and transplantation. The Lancet, 378(9800), 1414-8. Retrieved from http://search.proquest.com/docview/900104741?accountid=1437 5 Doig, C. & Rocker, G. (2003). Retrieving organs from non- heart-beating organ donors: a review of medical and ethical issues. Canadian Journal of Anesthesia, 50(10), 1069- 1076.http://www.springerlink.com/content/xq622m7g54h87301/ Fraser, Kimberly D,R.N., PhD., Estabrooks, Carole,R.N., PhD., Allen, Marion,R.N., PhD., & Strang, Vicki,R.N., PhD. (2010). The relational nature of case manager resource allocation decision making: An illustrated case. Care Management Journals, 11(3), 151-6. Frunza, M., Frunza, S., Catalin, V. B., & Grad, O. (2010). Altruistic living unrelated organ donation at the crossroads of ethics and religion. a case study. Journal for the Study of Religions and Ideologies, 9(27), 3-24. Retrieved
- 12. from http://search.proquest.com/docview/816629192?accountid =14375 Howard, Richard J,M.D., PhD., Cornell, Danielle L,R.N., B.S.N., & Cochran, L. (2012). History of deceased organ donation, transplantation, and organ procurement organizations. Progress in Transplantation, 22(1), 6-16; quiz 17 Miller, F. G., & Truog, R. D. (2008). Rethinking the ethics of VITAL ORGAN DONATIONS. The Hastings Center Report, 38(6), 38-46. Retrieved from http://search.proquest.com/docview/222366351?accountid=1437 5 Optional Reading Benning, T. M., Breugelmans, E., Dellaert, B. G., & C. (2012). Consumers' evaluation of allocation policies for scarce health care services: Vested interest activation trumps spatial and temporal distance. Marketing Letters, 23(3), 531-543 Denny, B. & Kienhuis, M. (2011). Using crisis theory to explain the quality of life of organ transplant patients. Progress in Transplantation, 21(3), 182-189 Hoy, H., Alexander, S., & Frith, K. (2011). Effect of transplant education on nurses' attitudes toward organ donation and plans to work with transplant patients. Progress in Transplantation, 21(4), 317-321 Spicer, J. (2008, Nov. 21). Distributive justice. Practice Nurse, 36(9), 45-48. Websites Moon, L. (2002). Organ Allocation. Retrieved fromhttp://www.miracosta.edu/home/lmoon/allocate.html. Consent forms for Research must include several elements
- 13. Identify ResearchThe subject’s involvement must be identified as researchThe research must be describedThe purpose of the research must be explained RisksRisks and consequences of the research activity must be clearly set forth BenefitsThe benefits of the proposed research must be explained AlternativesIf the investigations is clinical, the diagnostic and therapeutic alternatives must be described Research RecordsThe mechanism and process of protecting privacy and maintaining confidentiality of records and data must be described CompensationThe availability of compensation for participation must be explainedThe availability of treatment in the event of injury must be explained Contact PersonThe consent form must clearly identify the
- 14. person to contact with questions, concerns, inquiries, or in the event of injury Individual RightsThe right of the individual to refuse participation or withdraw from the research must be explained Ethics mod 5 discussion Consent to Terminate Care Actions for 'Consent to Terminate Care' Previous Next Hide Description Your comments will be graded on how well they meet the Discussion Requirements posted under “Before You Begin.” In Belgium, where euthanasia has been legal for people over the age of 18 since 2002, the government is considering an amendment to the law to include children. This is something that no other developed country has permitted (Belgium). The same bill would offer the right to die to adults with early dementia (Belgium). Advocates argue that euthanasia for children, with the consent of their parents, is necessary to give families an option in a desperately painful situation (Belgium). However, opponents have questioned whether children can reasonably decide to end their own lives (Belgium). In the last decade, the number of reported cases per year has risen from 235 deaths in 2003 to 1,432 in 2012, the last year for which statistics are available (Belgium). Doctors typically give patients a powerful sedative before injecting another drug to stop their heart. Only a few countries have legalized euthanasia or anything approaching it. In the Netherlands, euthanasia is legal under specific circumstances and for children over the age of 12 with parental consent (there is an understanding that infants, too, can be euthanized, and that doctors will not be prosecuted if they act appropriately) (Belgium). Elsewhere in
- 15. Europe, euthanasia is only legal in Luxembourg. In the U.S., Oregon is the only state that legalized physician-assisted suicide. Assisted suicide, where doctors help a patient to die but do not actively kill them, is allowed in Switzerland. Is it ethical for healthcare professionals to support the practice of assisted suicide/euthanasia? Regardless of your personal view on the topic, please provide an argument which supports, and then opposes the practice of assisted suicide/euthanasia. Be certain to support your positions with credible evidence. Reference Belgium considering controversial new euthanasia law for children. (October 31, 2013) Associated Press. Retrieved from:http://www.foxnews.com/health/2013/10/31/belgium- considering-controversial-new-euthanasia-law-for-children/ Module 5 - SLP CONSENT AND RESEARCH The ultimate goal of the Session Long Project is to identify and evaluate the ethical principles used in resolving ethical dilemmas, and to apply the principles to specific ethical issues that may have professional, sociological, economic, and legal or political implications. Select a national (government) healthcare agency and discuss the ethical practices that it applies to experimentation and research. SLP Assignment Expectations 1. Identify the practice along with a companion theory. 2. Are these practices enough to ensure safe and ethical research? If not what should be added to them? 3. Limit your responses to a maximum of three pages, not including title and reference pages. 4. Be sure to provide scholarly support for your discussion. 5. Several (3-5) scholarly references should be cited for this assignment. Be sure to properly cite all references. 6. Apply critical thinking skills within the write-up for this
- 16. assignment. Your paper will be evaluated based on the rubric criteria. Please be sure to provide citations of sources consulted in preparing your paper in the body of the actual document itself (i.e. in addition to furnishing a reference list). Remember, any statement that you make that is not common knowledge or that originates from your synthesis or interpretation of materials you have read must have a citation associated with it. For guidelines on in-text citations, visit the following web site: http://owl.english.purdue.edu/handouts/research/r_apa.html Module 5 - Case CONSENT AND RESEARCH Assignment Overview For this Case Assignment, you are part of a medical research team and are tasked with gaining informed consent from potential participants. The study will seek to test an experimental drug with patients suffering from late-stage leukemia. The sample will be divided into a control group and the experimental group. Participants in the control group will be given a placebo, which could increase the progression of their disease. The sample will be composed of children. Case Assignment Discuss how you would go about seeking the consent of participants. · What questions would you expect from their parents/guardians? · How much information should you share with the children? · Should this type of study involve children given the risks of speeding the progression of the disease? Assignment Expectations 1. Apply critical thinking skills within the write-up for this assignment, especially with regard to #2 and #3 above. 2. Limit your responses to a maximum of three pages, not including title and reference pages.
- 17. 3. Provide scholarly support for your justifications. Be sure to properly cite all references. Your paper will be evaluated based on the rubric criteria. Module 5 - Home CONSENT AND RESEARCH Modular Learning Outcomes Upon successful completion of this module, the student will be able to satisfy the following outcomes: · Case · Examine the ethical implications of "consent." · SLP · Select a national healthcare agency and discuss the ethical standards that apply to experimentation and research. · Discussion · Discuss whether healthcare personnel should be involved in assisted suicide from an ethical perspective. Module Overview Human Experimentation The Nuremberg Code of 1946 was the first publicly written international document providing a code of ethics relating to research on human subjects. The Code represented an absolute commitment to the doctrine of informed consent. "The voluntary consent of the human subject is absolutely essential." Also, the duty and responsibility for ascertaining the quality of consent rests "upon each individual who initiates, directs, or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity." Trials of War Criminals before the Nuremberg Military Tribunal under Control Council Law No. 10 (Vol. 2) (Washington, D.C.,: U.S. Government Printing Office, 1949). While the Nuremberg Code focused on the responsibility of the individual engaging in research activities, the United States Federal Government has placed responsibility on institutions as well as the individual. By 1970, the first federal guidelines
- 18. designed to protect human research subjects were issued by what is now the Department of Health and Human Services. Federal regulations now require that all research projects funded by the DHHS be reviewed by local institutional review boards (IRB). The IRB is said to be the central mechanism through which the regulatory goal of protecting the rights and welfare of subjects of research is carried out. Informed Consent Medical procedures and experimentation required the expressed written consent of patients and participants. Consent sometimes called informed consent involves obtaining permission to proceed with procedures or experimentation after the patient/participant was informed of the risks, procedures, benefits, and safeguards that are in place to protect the best interest of the patient/participant. The matter of consent can raise legal and ethical challenges if the patient/participant is mentally handicapped or otherwise incapacitated. Those lacking the cognitive faculties to understand the information may rely upon caretakers. End-of-life End-of-life decisions can be difficult for family members of those incapacitated and not expected to recover. When does life end? Who should decide when life should end? Should medical professionals rely on the subjective opinions of family members in making the decision? Codes of Ethics National organizations that serve individuals working in the human services or health-related fields offer codes of ethics for their members. The codes of ethics typically build on common virtues that promote the best interests of clients and patients. The virtues can be reduced to “Do no harm.” The codes cover the scope of practice and include guidelines for consent and for end-of-life decisions. The codes of ethics can be obtained on organizational websites. Click for a PowerPoint presentation on federal regulations regarding consent forms.
- 19. Module 5 - Background CONSENT AND RESEARCH Required Reading Atac, A., et al. (2005). A Study of the Opinions and Behaviors of Physicians with Regard to Informed Consent and Refusing Treatment. Military Medicine, 170(7), 566-71. Brudney, D. (2009, Mar./Apr.). Choosing for another: beyond autonomy and best interests. The Hastings Center Report. 39(2), 31-38. Dickman, R. L. (2000, March). Bending the rules to get a medication. American Family Physician 61 (5), 1563. http://www.aafp.org/afp/2000/0301/p1563.html Erlen, J. A. (2010). Informed consent: Revisiting the issues. Orthopaedic Nursing, 29(4), 276-80. Retrieved from Lambert, V., & Glacken, M. (2011). Engaging with children in research: Theoretical and practical implications of negotiating informed consent/assent. Nursing Ethics, 18(6), 781-801. doi: http://dx.doi.org/10.1177/0969733011401122 Miller, F. G., & Wertheimer, A. (2011). The fair transaction model of informed consent: An alternative to autonomous authorization. Kennedy Institute of Ethics Journal, 21(3), 201- 18. Retrieved from Waller, B. N., & Repko, R. A. (2008). Informed consent: Good medicine, dangerous side effects.Cambridge Quarterly of Healthcare Ethics, 17(1), 66-74. Websites GAO Highlights (2005). Un-compensated Care. Retrieved fromhttp://www.gao.gov/new.items/d05743t.pdf. CRJ 548 – Crime Scene Investigation and Management DRNC Scenario This scenario corresponds with Course Objective I (see below).
- 20. Objective I: Definitively identify and assess crime scene requirements as to special needs and support logistics, to include, but not limited to, the needs and materials to establish proper search procedures and patterns, identify hazardous materials and situations, and considerations specific to mass crime scenes. Students will have a knowledge of the proper methods of crime scene photography as well as crime scene mapping and sketching and skills such as triangulation of crime scenes. The following story is a fictional account of an incident occurring during the mythical Democratic- Republican National Convention (DRNC) event in Miami, Florida. The story is loosely based on an amalgamation of real life occurrences. The names of all the characters in the story are fictional. Background Miami-Dade Police has been designated as the lead local agency and lead operational planner for the event security. Since this event meets the criteria of a National Special Security Event (NSSE), the U.S. Secret Service has been designated as the lead coordinating agency with overarching statutory authority
- 21. for the planning and execution of the event. U.S. Secret Service Supervisory Special Agent Samantha Salerno has been appointed as the lead agent in-charge for the event. Due to the influx of tens of thousands of delegates, visitors, and protestors, it is expected that the forensic processing and evidence retention for a mass number of assaults, larcenies and other crimes will increase considerably during the week of the event. It is clear that a multi-agency approach such as the ones used for the 2003 FTAA Conference, the 2004 Presidential Debates, and the Super Bowls of 2007 and 2010 must be employed for this large-scale special event as well. Neither the Miami Police Department (MPD), nor the Miami- Dade Police Department (MDPD) have the forensic assets adequate to handle such a large-scale event by themselves. It would take some degree of shared responsibility between MPD and MDPD, as well as some of the 30+ other incorporated areas such as Miami Beach, Hialeah, and Coral Gables. In addition to the local and federal agencies already mentioned, crime scene and forensic units from Florida’s Regional Domestic Security Task Force
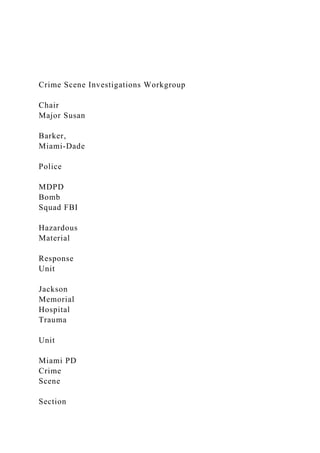
- 22. (RDSTF - Region 7) have been detached to this event. These include, but are not limited to the Bomb Squads of Broward and Palm Beach Counties, as well as the crime scene units from both of those Region 7 counties. Other key players for the DRNC include the Federal Bureau of Investigations (FBI), the Bureau of Alcohol Tobacco & Firearms (ATF), the Department of Homeland Security (DHS), the Department of Energy (DOE), and the Florida National Guard’s 44th Civil Support Team. For the DRNC special event, a multi-agency Crime Scene Investigations Workgroup has been created under the Security & Public Safety Subcommittee. This workgroup is comprised of personnel from the Miami-Dade Police Crime Lab, the Broward County Sheriff’s Office Crime Scene Investigations Bureau, the City of Miami PD Crime Scene Section, Jackson Memorial Hospital, the FBI’s Hazardous Material Response Unit, the Miami-Dade Police Bomb Squad, the ATF’s explosive ordnance investigators, the Miami-Dade Medical Examiner’s Office, the 44th Civil Support Team of the Florida National Guard, and Miami-Dade Fire Rescue’s Urban Search & Rescue Team (see
- 23. the DRNC Crime Scene Investigations Workgroup Org Chart provided). The Crime Scene Investigations Workgroup created several multi-agency teams specifically designed to respond to mass casualty chemical, biological, radiological, nuclear, or explosive (CBRNE) incidents occurring during the event. One such team was the Joint Hazard Response Team (JHRT). The JHRTs are comprised of multi-disciplinary experts from MDPD, MPD, ATF, FBI, and the 44th CST (see the JHRT org chart provided). Another multi-agency team specifically created for the DRNC was the Joint Forensic Investigation Team (JFIT). The difference between the JHRTs and the JFITs is that the former responds to bombing and WMD incidents before, or during the threat, while the latter respond after the bombing or threat has become apparent. Simply stated, JHRTs are first responders and assessors of CBRNE incidents, while the JFITs are responsible for post-blast investigations. However, it should be noted that many of the same expert personnel serve on both the JHRT and JFIT teams.
- 24. In addition to these two event-specific teams, the South Florida Joint Terrorism Task Force (JTTF) is also involved in the DRNC security planning before the event, as well as investigative response during and after the event. The JTTF is a long-standing multi-agency investigative group that is headed by the FBI, and supported with personnel by the local law enforcement agencies. Table 1 provides a brief explanation of what each of these multi-jurisdictional organizations provide. Jurisdictional Authority While the U.S. Secret Service has been designated as the lead coordinating agency for the DRNC event, there are other jurisdictional issues that need to be aware of. Miami-Dade Police have jurisdictional authority for crimes occurring within Miami-Dade County. The same holds true for Broward County and Palm Beach County respectively. In other words, jurisdictional issues during the DRNC event will be no different than during regular times. One important jurisdictional issue has to do with the investigation of bombings. If the explosion is determined to be a result of a terrorist incident, the FBI has the authority as the lead investigative agency.
- 25. Non-terror related bombings are relegated to the ATF. Of course, immediately after a bomb explodes, it is almost impossible to determine whether it was due to a terrorist, or a non-terrorist act. Typically, that is determined later during the investigation, as the pieces of the puzzle start to point to one direction or another. Since there is so much uncertainty during the first few hours of a bombing incident, both the FBI and the ATF respond, along with the local bomb squads and crime scene investigation units. That is why both the JHRTs and the JFITs are comprised of ATF and FBI agents. Table 1 Multi-Agency Group Permanent or Ad Hoc? Mission Comprised of Southeast Florida
- 26. Regional Domestic Security Task Force (RDSTF – Region 7) Permanent This is a multi-jurisdictional agency that is headed by the Florida Department of Law Enforcement (FDLE) and whose mission is to coordinate the flow of resources (funding as well as equipment), the flow of Miami-Dade Police, Miami PD, Broward County Sheriff’s Office, Ft. Lauderdale PD, Palm Beach County Sheriff’s Office, Monroe County Sheriff’s Office, FBI, ATF, Florida National Guard, Florida Highway Patrol,
- 27. information, and the coordination of a multiple jurisdictional response to terrorist incidents. Regional hospitals, and the Emergency Management departments of the four counties in Region 7. South Florida Joint Terrorism Task Force (JTTF) Permanent This group is headed by the FBI. Its mission is to coordinate all terrorism-related investigations in the South Florida area. The JTTF also manages the Southeast Florida Fusion Center, which serves as a data collection, and intelligence
- 28. dissemination function. FBI, ATF, FDLE, MDPD, Miami PD, Broward Sheriff’s Office, Ft. Lauderdale PD, Palm Beach County Sheriff’s Office, and other local police departments. Joint all-Hazards Response Teams (JHRTs) Ad Hoc for the DRNC event only This ad hoc team is responsible for mitigating chemical, biological, radiological, nuclear, and explosive (CBRNE) threats before they occur, and responding to an incident which
- 29. has already occurred in order to minimize the effects of the threat. Bomb squad and Hazmat technicians from the following agencies: Miami-Dade Police, Miami PD, Broward County Sheriff’s Office, Ft. Lauderdale PD, Palm Beach County Sheriff’s Office, Monroe County Sheriff’s Office, FBI, ATF, Florida National Guard, Miami-Dade Fire Rescue Dept., Broward Fire-Rescue… Joint Forensic Investigation Team (JFIT) Ad Hoc for
- 30. the DRNC event only This ad hoc team is responsible for post-blast investigations that may occur during the DRNC event. Crime scene investigations and forensic laboratory assets of the above listed agencies. Scenario The DRNC is a five-day event that takes over a year to plan for. The epicenter of the convention is located at the American Airlines Arena (also known as the “Triple A”) in Downtown Miami. A buffer zone has been erected around the arena, as well as the entire Bayside and Bayfront Park areas, and the Intercontinental Hotel. The area inside the buffer zone is considered as the “security zone” and is where the delegates who attend the convention will have free access. The security zone extends to the waters
- 31. of Biscayne Bay, and includes the entire Port of Miami. Entry into the secure zone is strictly monitored at four locations along the buffer zone perimeter. Only persons with the proper credentials are allowed into the security zone. Two of the four entry/exit gates are located at the AAA, and the west gate into the Intercontinental Hotel grounds. The other two access points into the secure zone are from the dockyard at the east side of the AAA, and the pier at the east side of the Intercontinental Hotel. These two access points are for pre-screened ferry boats that help to shuttle the delegates from the hotel to the AAA arena. All persons (including on-duty law enforcement personnel) must be screened prior to entry into the security zone. The screening involves a multi-stop queue whereby all vehicles and persons entering the security zone are subjected to an X-ray examination (VACIS machine for vehicles), magnetometers, explosive detection K-9s, and a physical pat down search. In addition, SWAT team counter-snipers are placed at high locations at various places in order to prevent any terrorist bombers (and their vehicles) from getting access into the security zone. This
- 32. screening process is one of the strictest and most elaborate in the world, yet it is not completely infallible. There have been several accounts of people getting past the security gates, into the security zone during previous Super Bowls and political conventions. So far, the intruders have been non-terrorists. One week prior to the start of the DRNC in early August, a team of 40 K-9 officers and their dogs swept every inch of the AAA and its surrounding property. These K-9 officers came from all parts of Florida, as well as a few federal agencies from Washington, D.C. Immediately after sweeping certain areas in and around the AAA, security guards were posted on a 24-hour basis to make sure that no explosive devices would be placed after the sweep. Once the K-9 team’s commander felt comfortable that the areas had been secured, a guard would be posted and then the K-9s would go onto somewhere else to sweep another critical area (such as the Intercontinental Hotel). The police were not the only ones who were getting ready the week prior to the start of the DRNC event. It appears that some adversarial groups were getting ready as well. Five days before the DRNC, the
- 33. Bomb Management Center (located at the Broward County Emergency Operations Center) received a barrage of suspicious device calls (i.e., bombs) at various locations in Miami-Dade County. The Miami- Dade Bomb Squad responded to seven different calls in which backpacks had been abandoned in the Downtown Miami area (outside the exclusionary area). One of them turned out to be the belongings of a homeless person who slept under the Metrorail station in Overtown. However, the other six turned out to be elaborate hoax devices. All six of these devices were determined by the bomb techs to be inert, and posed no danger of explosion. Nevertheless, the fact that so many hoax devices were turning up during the week prior to the DRNC was somewhat troublesome. That week, Tim Johnson the FBI Supervisory Special Agent, and lead worker of the Miami JTTF, called an impromptu meeting at the South Florida Fusion Center, located in Broward County to discuss the recent rash of hoax bomb calls. Also present at the meeting were Mary Straight (Fusion Center Chief Analyst), Detective Mike Warner (MDPD and JTTF member), Detective Frank Gomez (City of Miami PD, and JTTF member), Detective Josh Marcussen (Broward
- 34. Sheriff’s Office, and JTTF member), and Detective Fred White (Palm Beach SO, and JTTF member). Sergeant James Boyd of the Miami-Dade PD Bomb Squad was also invited and asked to debrief the JTTF investigators regarding the hoax devices. At the onset of the meeting, Tim Johnson asked Sergeant Boyd to describe the six hoax devices that were found at various locations around Downtown. Sergeant Boyd reported that in his opinion, all six hoax devices were very similar in composition, and were likely constructed by the same person. Next, Mary Straight reported that in five of the six hoax bomb cases had been captured on video from the pole cameras in the Downtown area. Several months before the DRNC, pole video cameras were placed at almost every corner of Downtown Miami. These high resolution cameras covered almost every conceivable angle in the Downtown area, and could be zoomed in to get a fairly clear picture of individual peoples’ faces. It is fairly well known within law enforcement and security realms that hired personnel cannot conceivably monitor every possible angle that these cameras reached. However, some new software advances had made the task
- 35. of video surveillance much better in that the software was programed to sense when items had been left behind by suspects. If after 10 seconds the item had not been recovered by a person, then the alarm at the video monitoring station would sound, and the attention of the security monitor would be brought to that screen. This was an excellent surveillance tool that had been first used at a large scale special event during the 2007 Super Bowl in Miami. Mary passed out printed handouts of close-up screen capture photos of the two subjects who had dropped off the hoax devices in five out of the six cases. Mary stated, “we have run these two through our facial recognition software, and compared them to all of our data banks, but we don’t have any matches so far. All I can tell you so far is that these guys are white males, about 5’ 6” and both weighing about 140 pounds.” “Geez...these two guys look almost like the two Boston Marathon bombers,” stated Johnson. They’re dressed the same, and even their faces are similar. If I didn’t know better, I would say that those two had
- 36. been resurrected.” “Well...they haven’t been resurrected, but it looks like these two guys have resurrected the idea,” remarked Mary. “We don’t have any other leads on these two at the moment...and we don’t know if they’re just Anarchist hoaxers who are doing this to spread our bomb squad resources thin, or whether these guys are serious bombers. There’s no way to tell right now.” Sergeant Boyd interrupted, “yeah...even though these were all hoax devices, let’s not discount the possibility that these subjects are real bombers who are placing these hoax devices to see how we respond to them. Every time that we go to a bomb call, we are always wary that someone is watching us and our procedures.” “Agreed,” said Johnson. “We need to have a couple of surveillance teams on the ground in case these guys show up again. If we find them...we’ll tail them for a while and try to find out if they’re working alone, or as part of a larger group. I already have Detective Phil Herrera’s surveillance team on standby in Downtown Miami from 7 a.m. to 7 p.m., and Tom Sullivan’s
- 37. team from the Tampa JTTF is handling the evening shift.” Detective Mike Warner asked, “Tim...what are your thoughts of putting out a press release to the public with these guys’ picture on it like they did up in Boston for the Marathon bombers?” “Mike, we may have to that eventually, but I think it’s premature at this point. Even if a concerned citizen who knows their identity reported them to us, we don’t have much in the way of criminal charges against them.” “That’s true, but at least we can nail them on State charges related to the building and possession of hoax devices,” replied Warner. “You make a good point Mike, but let’s try to find them with our surveillance teams first...and if we don’t do it within the next two days, then we’ll release the information and pictures to the public and try that route. If we do the press release now, these two guys will know that we’re looking for them, and they may take off to who knows where. So far, none of the devices contained any explosives, so I don’t view this as an imminent threat to the public.”
- 38. Warner responded, “OK...I see your point, and I agree with what you’re saying. However, if by Monday morning we haven’t found these guys, then I think we need to alert the public.” Warner turned to Sergeant Boyd and asked, “Jim, we’ll need your Bomb Squad on standby all weekend, in case we find these guys and they lead us to their stash of bomb making materials.” “No problem Mike. In fact, all six of my guys are already assigned to ad hoc J-HRT teams and their days off have been cancelled until the DRNC is over,” replied Sergeant Boyd. With that, the meeting at the South Florida Fusion Center concluded. Five Days Later (Monday, the first day of the DRNC event) It was early Monday morning...the first day of the DRNC event in Downtown Miami. Supervisory Special Agent Tim Johnson called another meeting of the JTTF. Johnson started the meeting, “alright…so far the surveillance teams or the cameras have not picked up on the two subjects that we’ve been looking for. I think it’s time to release the subjects’ pictures to the public and seek their assistance.”
- 39. Detective Warner interrupted, “Tim, I just got a text message from the Bomb Squad sergeant. He said that his bomb squad got called out late Sunday night for five separate suspicious package calls at various Metrorail stations. According to Jim Boyd, so far his teams have rendered safe three out of the five, and this time no hoax devices...all of them turned out to be real bombs.” Johnson stated, “it sounds like we have some real live bombers on our hand. Mary, do we have anything on video this time?” Analyst Mary Straight answered, “yes we do…as a matter of a fact, that’s how one of the calls for the Bomb Squad came from. We have a video of the same two guys...wearing the same clothing as last week…dropping off a backpack at the train level of the Overtown Metrorail station. Unfortunately, by the time we got a hold of the surveillance team on the ground, the two guys disappeared and we have nothing on their location or direction of travel.” “Well I guess it’s time to release the information to the public,” said Johnson. “Tim...I just got additional information from the Bomb Squad
- 40. sergeant. He’s now telling me that two other devices have detonated...one south in the Vizcaya Metrorail station, and another north of Downtown, in the Earlington Heights Metrorail. Apparently, there have been many casualties…as many as 100 dead or injured…it’s too early to say,” said Detective Warner. “OK...I’m hearing the same thing from my sources,” stated Detective Frank Gomez (City of Miami PD). “Over a hundred casualties...mostly Metrorail commuters…It looks like many of the injured at the Vizcaya station are being transported to South Miami Hospital. The injured persons from the Earlington Heights explosion are being transported to Jackson Memorial Hospital’s trauma unit.” “OK...it sounds like we have at least five…maybe seven different crime scenes…not counting the two hospitals,” stated Detective Warren. “I’ll get a hold of Major Susan Barker, who’s in charge of the joint forensic teams that have assembled for the event. They’re going to have their hands full with so many different crime scenes. I hope she has enough people on her teams.” “Mary...can you please get a hold of our Joint Information Center (JIC) and give them the press release
- 41. that we put together last week?” Mary Straight nodded in agreement, but then said, “are you sure you want to release this information right now? You realize that the reporters are going to ask a lot of questions, and they are sure to ask why we didn’t release the information last week, when we first had it.” “Mary, I realize that we will come under a lot of scrutiny for not having released the pictures earlier...but let me deal with that later. Right now we need to find these two guys as soon as possible.” Assignment Instructions For this assignment, you are to write a 1200- to 2000-word essay. Your essay must identify and assess crime scene requirements as to special needs and support logistics, to include, but not limited to, the needs and materials to establish proper search procedures and patterns, identify hazardous materials and situations, and considerations specific to mass crime scenes. Consider how you would handle these related multiple crime scenes as if you were in Major Susan Barker’s shoes.
- 42. Resources (available in the course Doc Sharing area): (PDF) tee Task Force Org Chart (PDF)