Mental Illness, Crime and Stigma: Recovery and Support for Forensic Clients and Their Families
•
3 likes•1,194 views

This document discusses stigma faced by forensic clients with mental illness who commit crimes. It begins by defining forensic clients as those found not criminally responsible due to mental illness. It describes how stigma develops in society and is especially strong for forensic clients due to a double stigma of mental illness and criminality. The document outlines how stigma impacts recovery and community reintegration for forensic clients and their families by decreasing treatment adherence and social engagement. It recommends promoting recovery-oriented practices, education to decrease ignorance, and support for families to help reduce this stigma.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Mental Illness, Crime and Stigma: Recovery and Support for Forensic Clients and Their Families
Similar to Mental Illness, Crime and Stigma: Recovery and Support for Forensic Clients and Their Families (20)
More from The Royal Mental Health Centre
More from The Royal Mental Health Centre (20)
Recently uploaded
Recently uploaded (20)
Mental Illness, Crime and Stigma: Recovery and Support for Forensic Clients and Their Families
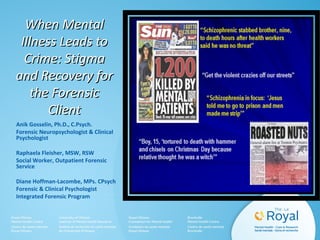
- 1. When MentalWhen Mental Illness Leads toIllness Leads to Crime: StigmaCrime: Stigma and Recovery forand Recovery for the Forensicthe Forensic ClientClient Anik Gosselin, Ph.D., C.Psych. Forensic Neuropsychologist & Clinical Psychologist Raphaela Fleisher, MSW, RSW Social Worker, Outpatient Forensic Service Diane Hoffman-Lacombe, MPs. CPsych Forensic & Clinical Psychologist Integrated Forensic Program
- 3. Agenda What it means to be a forensic client / non criminally responsible (NCR) Difference between NCR & antisocial / psychopathy How stigma develops in a society, the double stigma attached to the label “forensic client” The impact for the family What to do to decrease stigma, promote recovery and successful community reintegration 3
- 4. Integrated Forensic Program (IFP) Mandate The IFP provides specialized services -in assessment, treatment, rehabilitation and community reintegration -to persons with severe mental illness who have come into conflict with the criminal justice system -within a safe, therapeutic and recovery oriented environment 4
- 5. Forensic Services • Secure Assessment Inpatient Units: 24 beds • Secure Rehab & Transition Inpatient Units: 81 beds • Secure Mental Health: 4 beds • Outpatient Services: approx. 1500 clients ORB clients (FIRST, FITT, Transitional Housing) Brief Assessment Unit (BAU) out-of-custody General Forensic Clinic: includes general outpatients and Chrysalis Day Program Mental Health Court, Mental Health Court Clinic, OCDC Specialized Clinics: Sexual Behaviours, Anger Disorders, Family Court Clinic (Child Welfare & Youth) 5
- 6. Court-Ordered Assessments & Ontario Review Board (ORB) Clients • In-custody Fitness Assessments: 37 • Out-of-custody Fitness Assessments: 11 • In-custody NCR Assessments: 62 • Out-of-custody NCR Assessments: 18 • 201 ORB clients – 191 NCR – 10 unfit – 81 inpatients – 120 outpatients 6
- 7. Criminal Code of Canada Section 16 • Defence of Mental Disorder – no person is criminally responsible for an act committed or an omission made while suffering from a mental disorder that rendered a person incapable of appreciating the nature and quality of the act or omission or of knowing that is was wrong 7
- 8. Criteria for NCR finding • The person committed a crime • The person was suffering from a mental disorder • The mental disorder was a factor at the time of the crime – Not able to appreciate the nature and quality – Or not knowing that is was wrong i
- 9. NCR vs Antisocial & Psychopathy • Antisocial Personality Disorder: a pervasive pattern of disregard for and violation of the rights of others • Construct of psychopathy is defined by personality traits & behaviours (4 facets: interpersonal, affective, lifestyle, antisocial) • Able to appreciate the nature and quality of the act • Know that it was wrong (legally & morally) • Not psychotic; no loss of contact with reality • Choice of action; actions not driven by illness 9
- 13. THE STIGMATHE STIGMA OF MENTALOF MENTAL ILLNESSILLNESS By Anik Gosselin, Ph.D.,By Anik Gosselin, Ph.D., C.Psych.C.Psych.
- 14. WHAT IS STIGMA? Socially discrediting attribute, behaviour or reputation (Goffman, 1963) •3 functions: – Exploitation/domination (e.g., racism) – Enforcement of social norms (e.g., smoking, obesity) – Evolutionary purpose (e.g., mental illness, AIDS) •Public Stigma: Negative attitudes held by public about people with devalued characteristics •Self-Stigma: Internalization of these public attitudes
- 15. PROGRESSIVE MODEL OF SELF-STIGMA (Corrigan & Rao, 2012) AWARENESS •“The public believes people with mental illness are weak” AGREEMENT •“That’s right. People with mental illness are weak.” APPLICATION •“I am mentally ill so I must be weak.” HARM •“Because I am weak, I am not worthy or able.” WHY TRY… The person gives up trying… (to hold a job, to have friends, to get help) because its not gonna change anything “I am not worthy and beyond help”
- 16. THE WHY-TRY EFFECT(Corrigan et al., 2009) Stereotypes Blame Dangerousness Incompetence Fewer behaviours in pursuit of goals! Decreased participation in evidence- based treatments Public Stigma Self-Stigma Awareness Agreement Application Social Mediators Self-esteem Self-efficacy
- 17. EFFECTS OF STIGMA ON THE TARGETED INDIVIDUALS • Depression, demoralization, shame (Lucksted et al., 2011) • Social avoidance, distancing (Link et al., 2004) • Increase in symptom intensity (Livingston & Boyd, 2010) • Increase in hospitalization, decrease in engagement (Kvrgic et al., 2013) • Decrease in hope and in quality of life (Mittal et al., 2012) • Decrease in treatment adherence and in help‐seeking (Vogel et al., 2013) • Poor self‐esteem and self‐efficacy
- 18. STIGMA IN FORENSICS– AN ADDITIONAL CHALLENGE TO RECOVERY • The forensic label: a double stigma ‘I am violent and mentally ill; I scare people, I am not worthy of love; I have to hide’ • Challenges for health care providers: – Building trust – Impact of learned helplessness → non‐engagement in therapeutic process • Housing difficulties
- 19. HOW TO FIGHT STIGMA? Policy and law changes ‒ Ex: make discrimination illegal (e.g., refusing a job or housing based on history of mental illness) Decrease ignorance and preconceived ideas through education Shift from medical model to recovery model •Recovery Model: System that provides hope, treat people with dignity and respect and support everyone in finding their path to better mental health and well‐being –Living a satisfying, hopeful and contributing life, even when there are limitations caused by mental illness (as opposed to finding a cure) •Include Peer Support Workers in multidisciplinary teams Change societal attitudes at the national level
- 20. GUIDELINES FOR RECOVERY‐ORIENTED PRACTICE: HOPE, DIGNITY, INCLUSION* Organized in 6 dimensions of recovery oriented practice: 1)Creating a culture and language of hope 2)Recovery is personal 3)Recovery occurs in the context of one’s life 4)Responding to the diverse needs of everyone living in Canada 5)Working with First Nations, Inuit and Metis 6)Recovery is about transforming services and systems *http://www.mentalhealthcommission.ca/English/initiatives/RecoveryGuidelines
- 21. DISCLOSURE STRATEGIES for the stigmatized individual (Corrigan & Rao, 2012) Social Avoidance Stay away from people so they don’t have a chance to stigmatize me Secrecy Go out into the world – work and go to church, but tell no one about my illness Selective Disclosure Tell people about my illness who seem like they will understand Indiscriminant Disclosure Hide it from no one Broadcast Be proud - Let people know
- 22. Double Stigma – Forensic Patients and Their Families Family Members/Caregiver’s for this presentation includes mother, father, brother, sister, husband, wife, and a close friend or relative. 22
- 23. Double Stigma – Family/Caregiver’s Feelings • Most people with severe mental illness live with family members. • Ongoing stress can be detrimental to caregiver’s mental and physical wellbeing • Carries significant emotional turmoil • Question their coping abilities • Feelings of being trapped • Protective of their sick family member in spite of clear signs of personal danger. • Desensitized to violence and associated fears 23
- 24. Double Stigma –Family/Caregiver’s Experiences • Public and media stigmatization of people with mental illness • Dealing with media and legal proceedings difficult and not in most people’s skill repertoire • Adverse publicity and hostility often directed toward offenders’ family members • Guilt by association, ostracism, general abuse, and physical violence • Feelings of shame and suffering common due to media exposure • Result in losing friends and becoming isolated in their community. Lack support network • Unaware of social and medical services offered to either patient or family • Feeling stigmatized key challenge facing forensic caregivers • Causes ambivalence among family members towards the perpetrator • Change of the family unit • Negative reporting adversely affects the recovery process and community reintegration of both the individual with mental illness as well as their family 24
- 25. Double Stigma – Mental Illness & Crime How we can help families • Helping the person with mental health issues: • Deliver co-ordinated and integrated care for the person with mental health and forensic issues • Helping the families and caregivers: • Provide counselling referrals to the caregivers • Develop support groups for forensic families 25
- 26. Double Stigma – How can our society reduce the impact of stigma for families • Education and Contact with the stigmatized groups • Use Media to decrease public stigma • Reducing the stigma leads to early identification and early treatment of mental illness • Research needed to determine impact of providing education through media and other outlets on early detection and treatment efforts. 26
- 27. Double Stigma – Mental Illness & Crime Key Family Information & Support Resources in Ottawa • L’Apogee • The Oasis in Kanata • Canadian Mental Health Association • Mental Health Crisis Line • Montfort Renaissance • National Alliance on Mental Illness (NAMI) Family to Family Programs • Parent’s lifeline of Eastern Ontario (PLEO) • Psychiatric Survivors Ottawa (PSO) • The Royal - Education Series and Coping with Mental Illness Group • Schizophrenia Society of Ontario, Ottawa Chapter • Youth Services Bureau (YSB) 27
- 29. Thank youThank you to our clientsto our clients for sharing their storyfor sharing their story Sean CliftonSean Clifton Francis LaveauxFrancis Laveaux Michael StewartMichael Stewart
- 30. Q & A Special thanks to Martin Manseau and John Espadero for their precious help with the multimedia
Editor's Notes
- READ ANIK, RAPHAELA AND DIANE BIOS READ MOVIE DESCRIPTION PRESENT MOVIE SECTION 1
- NCR – 35 INPTS; 95 OUTPTS OTTAWA -
- NCR – 35 INPTS; 95 OUTPTS OTTAWA – Since january 2015 Absolute discharge 8; new NCR / unfit 23 (about 20%)
- INTRODUCE SECTION 2 OF THE MOVIE NCR PRESENT THE MOVIE
- This is a section of the movie that highlights how impairing Sean’s illness was…
- This section of the movie is important to highlight how Sean initiated his recovery
- This is a section of the movie when Sean is finally ready to live in the community…
- Who did not think when confronted with family, friends or colleagues battling mental illness: he is not even trying, or she needs a big kick in the you know where…. As implied in this cartoon, mental illness is an invisible wound, making it much harder to understand. One major societal challenge to recovery from mental illness is stigma, that unfortunately, often results in self stigma. In the forensic system, the stigma is double because our clients also committed offenses while ill and the public tends to be afraid of them.
- Functions of stigma are threefold: Exploitation/domination (e.g., exploitation of a specific group): Some groups must have less power and fewer resources for dominant groups to have more. Slavery, prejudice against women, ethnic minorities. Enforcement of social norms (ex: obesity, smoking, homosexuality): Function here is to increase conformity with norms, in order to make the deviant rejoin and conform to the group. Only applies to behaviour or identity perceived as voluntary. Evolutionary pressure to keep people “infected” apart. People rather stay away just in case. Ex: mental retardation, handicaps, physical illnesses such as cancer, skin disorders, AIDS, missing limbs, blindness and deafness & mental illnesses, etc.
- WHAT HAPPENS WHEN INTERNALIZATION OF PUBLIC ATTITUDES? Why try effect: a known and researched phenomenon. Creates the contrary to what we want to promote a healthy and productive society
- Public stigma creates different impacts related to self stigma and in turn decreases likelihood of healthy recovery oriented behaviours!!! Unfortunately, while it appears that stigma is the result of the society attempts to increase protection, it creates the contrary to what we want. We want good treatment and individuals battling mental illness who are hopeful they can be treated effectively to stay away from trouble and recover. Best chance at protecting a society.
- Stigma is pervasive and it subtly and sometimes less subtly isolates and rejects the targeted individuals. It results in the following:
- Often we see people ending up in the forensic system because the families, left with very limited resources (revolving door phenomenon) end up calling the police. We have people who committed murders but most crimes are not violent or against another person (e.g., stealing/shoplifting, disturbances, threats, loss of control, non compliance with rules). Landlords are reluctant to lease to our clients. Pls take the risk. When they are well treated and ready to return to live in the community, our clients are typically quiet, in bed at 9 pm, they don’t drink, the rent is paid automatically every month, they are the ideal tenants! We follow them closely when they are in the community for very long as well, so any sign of relapse results in re-hospitalisation until stable again.
- Stigma is an error of society and must first be addressed in the society The outreach groups have demonstrated a decrease in negative attitudes towards mental illness. Decrease ignorance and preconceived ideas example: how many times our clients are portrayed as terribly dangerous criminals and they have been living in community successfully, and being extremely prosocial and abiding by rules…once their illness is treated…we closely follow them, so usually what we see happening is rehospitalization, but reoffending is actually extremely rare (approx 8% according to a national trajectory study, compared to approx 40% after release from prison) and much lower than reoffending after release from jail/prison. The Guidelines for recovery oriented practice is a direct example of how policy changes societal attitude: other examples are with drinking and driving, or wearing seatbelt.
- In 2014 the Mental health commission of Canada oriented best practices towards recovery oriented practices so changing attitude and way of envisioning mental illness. It works! Think of the campaign to wear seatbelts… Less than 40 years ago, people all had their ashtrays during a presentation like today! Now it would be impossible to imagine such a thing! Def: 1 – recovery is possible for everyone, hope stimulates recovery. Acquiring capabilities to nurture hope is the starting point for building a mental health system geared to fostering recovery: recovery is fundamentally about hope 2-core to recovery orientation is each person is unique and have the right to determine their own paths to mental health and well being. Importance of putting people at the centre of mental health practices and have practitioners partner with them. 3-recovery journey occurs outside of the mental health system, fostering recovery necessitates understanding people within the context of their lives. Family friends, spiritual and cultural communities, workplaces etc all influence mental health and can play an important role in supporting recovery 4- recovery oriented practices encourage and enable respect for diversity and are culturally responsive, as well as responsive to all age groups and all subgroups (e.g., gay & lesbians, etc). 5- there is a common ground between recovery principles and indigenous understandings of wellness (Ex: promoting self determination and dignity, adopting a holistic and strength-based approach). Imp also to understand how recovery for indigenous people is uniquely shaped by Canada’s history of colonization. 6- Achieving a fully integrated recovery-oriented mental health system is an ongoing process that will take time to implement. Commitment to recovery needs to find expression in everything an organization does, including ensuring support for a workforce that has the skills and resources required to deliver recovery-oriented practice.
- Be careful not to make the person responsible for suffering from self stigma. However, for the individual suffering from self-stigma, what had been shown to be effective is disclosure. There are different phases of non-disclosure/disclosure, starting with…This is personal to the individual however and there is no need to necessarily get to the broadcast phase to free oneself from self stigma. What is important to remember and the take home message tonight is: fight stigma because stigma ultimately hurt everybody Thank you!
- There are specific problems and experiences of those families who have a close relative with severe mental illness who have been involved in the criminal justice system.
- INTRODUCE LAST SECTION OF THE MOVIE AND PRESENT LAST $ MIN OF THE MOVIE OUT OF MIND OUT OF SIGHT