
Recommended
Recommended
More Related Content
Similar to Stat 1023 Assignment 2 Example Assignment 2 - comments .docx
Similar to Stat 1023 Assignment 2 Example Assignment 2 - comments .docx (7)
More from susanschei
More from susanschei (20)
Recently uploaded
Recently uploaded (20)
Stat 1023 Assignment 2 Example Assignment 2 - comments .docx
- 1. Stat 1023 Assignment 2 Example Assignment 2 - comments This example (on the next page) is based on the media story, “The 6 most common regrets men and women have after sex” (http://globalnews.ca/news/991303/the- 6-most-common-regrets-men-and- women-have-after-sex/). The original research report that describes the study is called, “Sexual regret: Evidence for evolved sex differences”; I’ve posted the report as a separate file alongside this example in case you wish to look at it. If you do, you’ll notice that the report describes three (3) separate studies. The original media story only discussed the results and conclusions of Study 3. Consequently, my version of the media story also only deals with Study 3. Finally, for creative purposes, I’ve created some imaginary quotes from one of the authors; I certainly didn’t interview the author—these simply represent what I think the author might say based on the information in the original research report. I’m using the ‘abbreviated title’ of ‘Regrets’—notice that this is how I named my file as well (otherwise, I would have lost 3 marks!). Remember that the purpose of this example is to show you the type of detail and structure that your assignment should demonstrate. The application/description of course material in this example may not be correct; it is simply an example of format and level of
- 2. detail. While you read this example, refer back to the ‘Steps to complete this assignment’ so you understand how those steps translate into the completed assignment. http://globalnews.ca/news/991303/the-6-most-common-regrets- men-and-women-have-after-sex/ http://globalnews.ca/news/991303/the-6-most-common-regrets- men-and-women-have-after-sex/ Feeling regretful about your last sexual encounter? Your gender might matter! At a singles mixer last weekend where you missed the opportunity to get to know someone of the opposite sex a little more ‘intimately’? Are you feeling a little remorseful about your missed opportunity, and wondering whether the other person feels the same? Turns out, they probably don’t! According to a recent research study, males and females have different regrets when it comes to casual sex encounters. Researchers from UCLA and the University of Texas explored differences in how men and women respond to participating in and passing up opportunities for casual sex. “We expected males to regret passing up an opportunity for casual sex more than females, and females to
- 3. regret engaging in casual sex more than males….our data suggest we were right,” explains Martie Haselton, co-author of the study. Haselton further explains that these differences might result from evolutionary differences between the genders. That is, with females taking on the bulk of reproductive effort (think about those nine months a woman must spend pregnant if a sexual encounter results in conception!), casual sex opportunities that are acted on could come with a energy- and time-expensive cost. Males, on the other hand, have an evolutionary history that encourages more sexual encounters; consequently, males should worry about lost potential for reproduction in the form of ‘missed’ sexual encounters. Does this research suggest that—as a female or male—you’ll always regret casual sex encounters according to your gender? Not necessarily: Haselton and colleagues based their conclusions on an internet survey that relied on visitors to a news site to click on a survey asking them to think about their level of regret (from “I’m glad I did it” to “I regret it very much”) after their last time they had casual sex with someone, or, passed up a chance
- 4. to have casual sex with someone. Over 24000 individuals from a diverse background (in terms of age, sexual orientation, educational background, and current relationship status) did respond to the survey—a very large sample size. Even though they achieved diversity in their respondents, Haselton points out that they had little control over who was responding and whether they were being completely honest (we’re talking about sexual regret here!). “We recognize that internet surveys come with their own limitations—who knows who’s answering the survey! But, we still feel confident in the data collected,” elaborates Haselton. He points to the fact that survey was anonymous, so people responding should have no pressure to be dishonest about their sexual regrets and experiences. Finally, Haselton emphasizes that everyone will feel differently about their casual sex opportunities: “Some of us regret our actions deeply (and hopefully learn from them), some of us don’t. Those differences are okay and
- 5. what make us unique! As evolutionary psychologists, our research team is simply interested in how our evolutionary history might influence these differences.” Original Research Report: Galperin, A., Haselton, M.G., Frederick, D.A., Poore, J., von Hippel, W., Buss, D.M., and G.C. Gonzaga. 2012. Sexual regret: Evidence for evolved sex differences. Archives of Sexual Behavior 42(7): 1145-1161. Doi: 10.1007/s10508-012-0019-3 Knee osteoarthritis has doubled in prevalence since the mid-20th century Ian J. Wallacea, Steven Worthingtonb, David T. Felsonc, Robert D. Jurmaind, Kimberly T. Wrene, Heli Maijanenf, Robert J. Woodsg, and Daniel E. Liebermana,1 aDepartment of Human Evolutionary Biology, Harvard University, Cambridge, MA 02138; bInstitute for Quantitative Social Science, Harvard University, Cambridge, MA 02138; cClinical Epidemiology Unit, Boston University School of Medicine, Boston, MA 02118; dDepartment of Anthropology, San Jose State University, San Jose, CA 95192; eDepartment of Anthropology, University of Tennessee, Knoxville, TN 37996; fLaboratory of Archeology, University of Oulu, Oulu 90014, Finland; and gBattelle Memorial Institute, Natick, MA 01760
- 6. Edited by Osbjorn Pearson, University of New Mexico, Albuquerque, NM, and accepted by Editorial Board Member C. O. Lovejoy July 12, 2017 (received for review March 7, 2017) Knee osteoarthritis (OA) is believed to be highly prevalent today because of recent increases in life expectancy and body mass index (BMI), but this assumption has not been tested using long-term historical or evolutionary data. We analyzed long-term trends in knee OA prevalence in the United States using cadaver-derived skeletons of people aged ≥50 y whose BMI at death was docu- mented and who lived during the early industrial era (1800s to early 1900s; n = 1,581) and the modern postindustrial era (late 1900s to early 2000s; n = 819). Knee OA among individuals esti- mated to be ≥50 y old was also assessed in archeologically derived skeletons of prehistoric hunter-gatherers and early farmers (6000– 300 B.P.; n = 176). OA was diagnosed based on the presence of eburnation (polish from bone-on-bone contact). Overall, knee OA prevalence was found to be 16% among the postindustrial sample but only 6% and 8% among the early industrial and prehistoric samples, respectively. After controlling for age, BMI, and other variables, knee OA prevalence was 2.1-fold higher (95% confi- dence interval, 1.5–3.1) in the postindustrial sample than in the early industrial sample. Our results indicate that increases in lon- gevity and BMI are insufficient to explain the approximate dou- bling of knee OA prevalence that has occurred in the United States
- 7. since the mid-20th century. Knee OA is thus more preventable than is commonly assumed, but prevention will require research on additional independent risk factors that either arose or have become amplified in the postindustrial era. arthritis | aging | obesity | mismatch disease | evolutionary medicine Osteoarthritis (OA) is the most prevalent joint disease and aleading source of chronic pain and disability in the United States (1) and other developed nations (2). Knee OA accounts for more than 80% of the disease’s total burden (2) and affects at least 19% of American adults aged 45 y and older (3). Sub- stantial evidence indicates that knee OA is proximately caused by the breakdown of joint tissues from mechanical loading (4) and inflammation (5), but the deeper underlying causes of knee OA’s high prevalence remain unclear and poorly tested, hin- dering efforts to prevent and treat the disease. Two recent public health trends, however, are commonly assumed to be dominant factors (6, 7). First, because knee OA’s prevalence increases with age (8), the rise in life expectancy in the United States since the early 20th century is thought to have led to high knee OA levels among the elderly, with the presumption that, as people age, their senescing joint tissues accumulate more wear and tear from loading (9). Second, high body mass index (BMI) has become epidemic in the United States in recent decades and is a well- known risk factor for knee OA (8), probably because of the combined effects of joint overloading and adiposity-induced in- flammation (10). Whether increases in longevity and BMI are responsible for current knee OA levels has never been tested, but this assumption has led many to view the disease’s high preva-
- 8. lence as effectively unpreventable, since aging is untreatable, and the high BMI epidemic is intractable (8, 11). One underused yet potentially powerful way to identify and assess the risk factors responsible for current knee OA levels is to examine long-term changes in the disease’s prevalence by com- paring contemporary with historic and prehistoric populations (12). Epidemiological studies of present day populations are valuable but are limited in their ability to analyze risk factors that are now pervasive but used to be less common. It is difficult to find large samples of living Americans whose lifestyles, including physical activity levels and diet, resemble those of past genera- tions. Although many variables cannot be measured and thus controlled in epidemiological studies of people living in the past, a major benefit of analyzing populations over historical and evolutionary time is to assess known risk factors under different environmental conditions and thus bring to light the effects of risk factors that might not be apparent or testable in modern populations alone. Furthermore, although knee OA is known to be ancient (12), we know very little about changes in its preva- lence over time. Low levels of knee OA have been reported for some historic and prehistoric populations (13–17), suggesting that the disease’s prevalence has recently increased, but these studies used different diagnostic criteria than those used to di- agnose knee OA in living patients, used samples composed mostly of younger individuals, and did not account for BMI, complicating comparisons with modern epidemiological data. Here, we investigate long-term trends in knee OA prevalence
- 9. in the United States and evaluate the effects of longevity and Significance Knee osteoarthritis is a highly prevalent, disabling joint disease with causes that remain poorly understood but are commonly attributed to aging and obesity. To gain insight into the eti- ology of knee osteoarthritis, this study traces long-term trends in the disease in the United States using large skeletal samples spanning from prehistoric times to the present. We show that knee osteoarthritis long existed at low frequencies, but since the mid-20th century, the disease has doubled in prevalence. Our analyses contradict the view that the recent surge in knee osteoarthritis occurred simply because people live longer and are more commonly obese. Instead, our results highlight the need to study additional, likely preventable risk factors that have become ubiquitous within the last half-century. Author contributions: I.J.W., S.W., D.T.F., and D.E.L. designed research; I.J.W., R.D.J., K.T.W., H.M., and R.J.W. performed research; I.J.W. and S.W. analyzed data; and I.J.W., S.W., D.T.F., and D.E.L. wrote the paper. The authors declare no conflict of interest. This article is a PNAS Direct Submission. O.P. is a guest editor invited by the Editorial Board. Freely available online through the PNAS open access option. 1To whom correspondence should be addressed. Email: [email protected] This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10. 1073/pnas.1703856114/-/DCSupplemental.
- 10. 9332–9336 | PNAS | August 29, 2017 | vol. 114 | no. 35 www.pnas.org/cgi/doi/10.1073/pnas.1703856114 http://crossmark.crossref.org/dialog/?doi=10.1073/pnas.1703856 114&domain=pdf mailto:[email protected] http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/-/DCSupplemental http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/-/DCSupplemental www.pnas.org/cgi/doi/10.1073/pnas.1703856114 Jennifer Highlight Jennifer Sticky Note (highlight in yellow) Most original research articles (primary sources in science) provide a full title, list of authors, and the author(s)affiliations (i.e. what research centres, organizations, and/or universities/colleges they belong to) at the start of the report. Jennifer Highlight Jennifer Sticky Note (highlight in blue) Research articles tend to be quite long and detailed; as a result, it would be difficult to determine whether the research is useful/interesting to the reader without reading the entire report. So, the 'abstract' (sometimes labeled as such, other times not) provides a short summary of the research objective(s), methods, results, and conclusions. Reading the abstract (in this
- 11. article, it's the first 'paragraph' in bold fond) is a good place to start because it gives an overview of what the report is going to discuss. Jennifer Highlight Jennifer Sticky Note (highlight in purple) The first major section of a research report is the 'Introduction' (also known as background, literature review, and possibly other names). The introduction typically gives background information (with reference to previous research) necessary to understand the objectives and hypotheses of the study being described. Most introductions start from very general knowledge and move to more specific content, ending with a descriptive statement of the study's objectives, and hypotheses. In this particular report, the last paragraph of the introduction describes the objectives/procedure ("Here, we investigate long- term trends...."). Reading the introduction can be useful because researchers often define important concepts or terms that they will use throughout their report. For the purpose of our assignment, you might just skim the introduction to provide some context for the next section ("methods"). BMI on levels of the disease by comparing the prevalence of knee OA among people who lived during the early industrial era (19th to early 20th centuries) with that of people from the modern postindustrial era (late 20th to early 21st centuries). We studied knee OA in the largest available collections of cadaver- derived skeletal remains of people of documented age, BMI, sex,
- 12. and ethnicity. To further consider knee OA levels from an evo- lutionary perspective, we also analyzed knee OA in a large sample of archeological skeletons of prehistoric Native Ameri- can hunter-gatherers (6000–300 B.P.) and early farmers (900– 300 B.P.). Although BMI is undocumented for prehistoric skel- etons, the age at death and sex can be estimated, allowing us to assess the prevalence of knee OA among older individuals in these populations. The skeletal collections used in this study are, by necessity, samples composed of individuals who could not be randomly selected and for whom we lack comprehensive de- mographic and contextual information. Despite these limitations, these samples constitute the best available evidence for knee OA levels in the United States during earlier time periods to test if prevalence of the disease is higher today than in the past. Materials and Methods Study Samples. The early industrial and postindustrial samples studied in- cluded complete skeletons of people aged 50 y and older who lived in major urban areas in the United States (Table S1). All individuals were documented as being of either European-American or African-American ancestry. Early industrial individuals (n = 1,581) were inhabitants of Cleveland, Ohio and St. Louis, Missouri who died between 1905 and 1940. BMI at death was recorded for 84% of these skeletons (n = 1,334). Postindustrial individuals (n = 819) lived in Albuquerque, New Mexico and Knoxville, Tennessee and died between 1976 and 2015. BMI at death was recorded for
- 13. 64% of these skeletons (n = 525). All cadavers were acquired by academic institutions for the purposes of medical and anatomical education and research. Early in- dustrial cadavers were of individuals whose bodies were unclaimed at local morgues or became property of the state; postindustrial cadavers were gathered through body donation programs. Occupation was documented for only 23% of individuals (n = 544), but records indicate that differences between samples reflect shifts in the US workforce between early industrial and postindustrial times, with the early industrial sample comprising pri- marily highly physically active laborers and the postindustrial sample in- cluding more service sector workers with less physically demanding jobs (SI Text). Cause of death was documented for 80% of individuals (n = 1,918), and differences between samples evince the epidemiological transition be- tween early industrial and postindustrial times, with most deaths among early industrial individuals caused by infectious diseases, such as pneu- monia and tuberculosis, whereas most deaths among postindustrial indi- viduals were caused by noninfectious diseases, such as cancer and atherosclerotic heart disease (SI Text). Skeletons with knee joint articular surfaces that were severely damaged postmortem were excluded
- 14. from the study as were individuals with lower limb amputations. The prehistoric sample included skeletons from eight archeological sites (in Alaska, California, New Mexico, Kentucky, and Ohio) of people estimated to be aged 50 y and older who were hunter-gatherers (n = 116) and early farmers (n = 60) (Table S1). Only skeletons sufficiently preserved to examine both the right and left knees were included. Sex assignment was based on dimorphic characteristics of the pubis that have been shown to be 96% accurate (18). Individuals were estimated to be ≥50 y old based on age- related changes in the configuration of the auricular surface of the ilium (19). This method has been shown to correctly exclude individuals younger than 50 y of age with 100% accuracy (20). Unfortunately, esti- mating age precisely beyond 50 y is not possible with available osteo- logical methods, and it is not possible to estimate accurately BMI at death from skeletal remains. Knee OA Diagnosis. Diagnosis of knee OA was based on visual identification of the presence of eburnation on the articular surfaces of the right or left distal femur, proximal tibia, or patella. Eburnation is a sclerotic, ivory-like reaction of subchondral bone that occurs from bone-on-bone contact at
- 15. sites exposed by advanced cartilage erosion (12, 21). In pathology studies of skeletal re- mains, eburnation is considered pathognomonic for moderate to severe OA (12, 22–24). Although it was not possible to assess knee OA blinded to the skeleton’s collection of origin, eburnation can be identified with negligible interobserver variation (SI Text). To avoid false-positive diagnoses, individuals exhibiting knee eburnation but also osteological signs of non- OA arthritides, such as rheumatoid arthritis, calcium pyrophosphate deposition disease, and spondyloarthropathy, were excluded. Osteophytes, bone spurs that often form at the margins of osteoarthritic joints (22–25), were generally large and expansive on eburnated knees but were not used as a diagnostic criterion for knee OA because interobserver variation in identifying osteophytes in skeletal samples is high (26), and they can lead to false-positive diagnoses (12); also, arthroplasty prostheses were not used to diagnose the disease among postindustrial individuals. Knee OA prevalence estimates for our samples are therefore underestimates of total disease prevalence, because they do not include mild (or early) cases of knee OA [e.g., cases that would be classified as two on the Kellgren–Lawrence scale (25)] or cases of the disease where
- 16. arthroplasty prostheses obscure underlying eburnation. Statistical Analyses. Log-binomial generalized linear models (GLMs) were used to estimate adjusted prevalence and prevalence ratios for knee OA, which are reported with 95% confidence intervals (95% CIs). Prevalence is a measure of effect size that varies as a function of the values of predictors. Here, we predict prevalence over a range of values of the predictor of interest while holding all other covariates constant at the sample mean. A prevalence ratio is a measure of effect size that is constant over the range of the predictor of interest while controlling for other covariates. Since prevalence ratios are multiplicative, they denote a rate of change (percentage change) of the response per unit increase in the predictor of interest. Model goodness of fit was assessed using the Hosmer–Lemeshow χ2 test, with significance of in- dividual estimates determined through two-sided Wald tests with an alpha level of 0.05 (Table S2). Three separate GLMs were performed with a binary response variable indicating presence or absence of knee OA for each individual but including different explanatory variables. The first analysis included the prehistoric, early industrial, and postindustrial samples and controlled only for sex effects,
- 17. since age and BMI were undocumented for prehistoric individuals. The second and third analyses included only the early industrial and postindustrial samples and additionally controlled for age, BMI, and ethnicity. The second analysis used all available individuals weighted equally, whereas the third analysis incorporated a subset of individuals who were differentially weighted based on optimal matching of covariate values between the early industrial and postindustrial samples. The analysis of matched data was performed as a sensitivity check to assess whether inferences were robust to sampling bias between the early industrial and postindustrial samples. This bias was evidenced by the large differences in average covariate values between these two samples in the unmatched data (Table 1). The purpose of matching is to approximate an experimental template, where the matching procedure mimics blocking before random group assignment to balance average covariate values between “target” and “comparator” groups. Separation of the estimation procedure into two steps simulates the re- search design of an experiment where no information on outcomes is known at the point of experimental design and randomization. The non- parametric matching procedure is therefore a data preprocessing step that
- 18. replicates a randomized experiment with respect to observed covariates (27). Preprocessing was achieved by matching individuals from the early industrial and postindustrial samples that had a similar propensity to be included in the postindustrial sample based on covariate values (SI Text). Pruning nonmatches increased similarity in average covariate values be- tween the early industrial and postindustrial samples (Table 1) and reduced model dependency and bias (28). Weights for each individual were con- structed to estimate the average effect of interest on the postindustrial sample, with the early industrial sample weighted to look like the post- industrial sample. Analyses were conducted using R, version 3.3.2 (29). Results Long-Term Change in Knee OA Prevalence. Across all individuals analyzed (n = 2,576), the prevalence of knee OA was markedly higher among individuals from the postindustrial era compared with individuals from early industrial and prehistoric times, with females more affected than males (Fig. 1 A and C). After con- trolling for sex, knee OA prevalence in the postindustrial sample (16%; 95% CI, 14–19%) was 2.6 times higher (95% CI, 2.1–3.4; P < 0.001) than in the early industrial sample (6%; 95% CI, 5– 7%) and 2 times higher (95% CI, 1.3–3.3; P = 0.003) than in the prehistoric sample (8%; 95% CI, 5–13%). Among postindustrial individuals with knee OA, 42% (64/151) had the disease in both
- 19. knees, a 2.5-fold higher proportion (Fisher’s exact test: P = 0.042) Wallace et al. PNAS | August 29, 2017 | vol. 114 | no. 35 | 9333 A N TH R O P O LO G Y http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/- /DCSupplemental/pnas.201703856SI.pdf?targetid=nameddest=S T1 http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/- /DCSupplemental/pnas.201703856SI.pdf?targetid=nameddest=S TXT http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/- /DCSupplemental/pnas.201703856SI.pdf?targetid=nameddest=S TXT http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/- /DCSupplemental/pnas.201703856SI.pdf?targetid=nameddest=S TXT http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/-
- 20. /DCSupplemental/pnas.201703856SI.pdf?targetid=nameddest=S T1 http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/- /DCSupplemental/pnas.201703856SI.pdf?targetid=nameddest=S TXT http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/- /DCSupplemental/pnas.201703856SI.pdf?targetid=nameddest=S T2 http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/- /DCSupplemental/pnas.201703856SI.pdf?targetid=nameddest=S TXT Jennifer Highlight Jennifer Sticky Note (highlighted in green) The next major section of a research report is the 'Methods' (sometimes 'Methods and materials', 'procedure', etc.). Depending on the publication, the methods section may come right after the introduction (as it does in this example), or it may be placed later in the report (e.g. towards the end). The methods section provides sufficient detail about the sampling procedure, study design, and statistical analysis/data manipulation that a reader could redo the study with a new set of data. For the purpose of our assignment, try not to get too bogged down in descriptions of statistical analysis and very discipline- specific methodology. Keep your focus on the level of detail/understanding we have worked with in our course. The report might not use the exact vocabulary you've seen in the course (they might, though!), but the descriptions they use
- 21. should be recognizable. Jennifer Highlight Jennifer Sticky Note (highlighted in red) The third major section is the 'Results' section. As the heading suggests, it is a description of the results. This section tends to be pretty painful to read, especially if the researchers used complex statistical analyses. But, it does present the results of all comparisons, hypothesis tests, descriptive summaries, etc. that they include in their report. You'll likely recognize means and standard deviations, you might also see reference to confidence intervals (e.g. 95% CI, 14-19) and hypothesis tests (e.g. P=0.003). You'll also see tables and figures summarizing key results to address research questions. For the purpose of our assignment, it's best to read through the Results section, looking for text that describes comparisons useful to our assignment, and to explore the data provided/summarized in tables and figures. Remember not to get hung up on the details of the statistical analyses reported. of bilateral cases of knee OA than among the diseased individuals in the prehistoric sample (17%; 3/18) and 1.4-fold higher (Fisher’s exact test: P = 0.058) compared with the early industrial sample (30%; 28/94). Temporal Change in Knee OA Prevalence Controlling for Age and BMI. To test whether the higher levels of knee OA in the post- industrial era are attributable to greater longevity and higher
- 22. BMIs, we analyzed the subset of individuals in our samples for Table 1. Sample composition and covariate balance before and after matching Variable Unmatched analysis Matched analysis Improvement, %Early industrial Postindustrial Early industrial Postindustrial Female/male ratio 0.17 0.41 0.46 0.39 71.3 Age, y 62.3 ± 9.7* 68.5 ± 10.4* 68.5 ± 9.8* 68.6 ± 10.4* 99.3 BMI, kg/m2 18.7 ± 4.2* 26.4 ± 8.0* 25.3 ± 6.8* 25.3 ± 6.3* 99.7 Ethnicity ratio† 0.32 0.023 0.039 0.024 95.0 Distance‡ 0.15 0.61 0.59 0.59 100 n 1334 525 857§ 500 100 *Mean ± SD. †African American/European American ratio. ‡Distance measure is the propensity score of being in the postindustrial sample, calculated using all observed covariates. §The 857 early industrial observations were down-weighted in log-binomial models to equal the 500 observations from the postindustrial sample, thus giving an effective sample size of 1,000 observations for the analysis of matched data. Female / male Early industrial / prehistoric Postindustrial / prehistoric
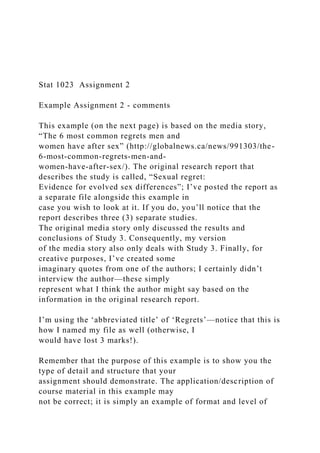
- 23. Postindustrial / early industrial Knee OA prevalence ratio (%) BMI Age Female / male Postindustrial / early industrial 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 Knee OA prevalence ratio C D 0 5 10 15 20 Pre his tor ic
- 25. ( % ) Ea rly in du str ial Po stin du str ial A B Fig. 1. Knee OA prevalence during different time periods. (A and B) Knee OA prevalence from regression models controlling for sex (A) as well as age, BMI, sex, and ethnicity (B). Dark and light gray bars are from unmatched and matched analyses, respectively (B). (C and D) Knee OA prevalence ratios from re- gression models including sex (C) as well as age, BMI, sex, and ethnicity (D) as predictor variables. Black and light gray dots are from unmatched and matched analyses, respectively (D). Age and BMI were entered into models as continuous variables, but effects are reported for 10-y and 5-U intervals, respectively (D).
- 26. Whiskers represent 95% CIs. Ethnicity effects are reported in Table S3. 9334 | www.pnas.org/cgi/doi/10.1073/pnas.1703856114 Wallace et al. http://www.pnas.org/lookup/suppl/doi:10.1073/pnas.170385611 4/- /DCSupplemental/pnas.201703856SI.pdf?targetid=nameddest=S T3 www.pnas.org/cgi/doi/10.1073/pnas.1703856114 whom age and BMI were documented (n = 1,859). Individuals from the postindustrial group were, on average, 6 y older and had 41% higher BMIs than their early industrial counterparts (Welch’s t test: P < 0.001 for both the age and BMI comparisons) (Table 1). Only 1% (13/1,334) of early industrial individuals were obese (BMI ≥ 30) and 6% (74/1,334) were overweight (25 ≤ BMI < 30) compared with 25% (132/525) and 24% (126/525) of postindustrial individuals who were obese and overweight, re- spectively (Fisher’s exact test: P < 0.001 for both the obese and overweight comparisons). Nevertheless, in a model controlling for age, BMI, and other variables, knee OA prevalence in the post- industrial sample (11%; 95% CI, 8–14%) remained 2.1 times higher (95% CI, 1.5–3.1; P < 0.001) than in the early industrial sample (5%; 95% CI, 4–7%) (Fig. 1 B and D). Age and BMI were posi- tively associated with knee OA prevalence (P < 0.001 for both variables) (Fig. 1D), but at all ages, knee OA prevalence was at least twice as high in the postindustrial sample than in the early industrial
- 27. sample, even after controlling for BMI (Fig. 2). Temporal Change in Knee OA Prevalence Assessed Using Matched Samples. Matching individuals from the early industrial and postindustrial samples by propensity score increased covariate balance by 99% for age, 100% for BMI, 71% for sex, and 95% for ethnicity (Table 1). In a model using these matched samples and additionally controlling for age, BMI, and other variables, knee OA prevalence in the postindustrial sample (15%; 95% CI, 12–19%) remained approximately twice as high (prevalence ra- tio: 1.9; 95% CI, 1.1–3.5; P < 0.029) compared with the early industrial sample (8%; 95% CI, 5–13%) (Fig. 1 B and D). Discussion To gain insight into the current high prevalence of OA in the United States and other developed nations, this study examined long-term trends in knee OA levels in the United States from prehistoric times through the early industrial era to the modern postindustrial era. These data show that knee OA long existed at low frequencies, but since the mid-20th century, knee OA has ap- proximately doubled in prevalence, even after accounting for the effects of age and BMI. Our analyses therefore indicate that, al- though knee OA prevalence has increased over time, today’s high levels of the disease are not, as commonly assumed, simply an in- evitable consequence of people living longer and more often hav- ing a high BMI. Instead, our analyses indicate the presence of additional independent risk factors that seem to be either unique to or amplified in the postindustrial era.
- 28. Retrospective studies cannot directly test causation, but the dramatic increase in knee OA prevalence in recent times raises the question of what these additional risk factors might be. Alleles of genes, such as GDF5, have been shown to influence knee OA susceptibility (30), but the approximate doubling of knee OA prevalence in just the last few generations proves that recent envi- ronmental changes have played a principal role. The results of this study are thus clinically significant because they indicate that knee OA may be more preventable than is currently supposed. Given evidence that nearly all knee OA is associated with loading- induced damage to joint tissues (4), either because the loads are abnormal or the tissues are structurally weak, one especially important source of environmental change that warrants greater attention is whether and how joint loading has altered. Trauma has presumably always predisposed some individuals to knee OA (8), as suggested by the predominance of unilateral knee OA since prehistoric times (31), and while joint overloading from high BMI has become common only recently, our results indicate that the majority of knee OA today is not caused by high BMI per se. Although altered loads generated by walking more frequently on hard pavements (32) or with certain forms of footwear (33) might be factors, another pos- sibility that merits more study is physical inactivity, which has
- 29. be- come epidemic during the postindustrial era. Less physically active individuals who load their joints less develop thinner cartilage with lower proteoglycan content (34, 35) as well as weaker muscles re- sponsible for protecting joints by stabilizing them and limiting joint reaction forces (36). Chronic low-grade inflammation, which is ex- acerbated by physical inactivity (37), modern diets rich in highly refined carbohydrates (38), and excessive adiposity (10), can further magnify and accelerate loading-induced damage to joint tissues and may also directly affect knee OA pathogenesis (5). Evaluating which of these or additional features of modern environments are re- sponsible for today’s high knee OA levels is necessary. This study has important limitations that need to be considered. First, the samples analyzed, although large for their kind, were constrained by the availability of well-curated skeletal collections in the United States, and it is plausible that these collections exhibit levels of knee OA that differ from the actual US population prev- alence. Second, BMI recorded at death is likely to underestimate average lifetime BMI, especially for individuals whose cause of death was associated with somatic wasting. While discrepancy be- tween lifetime and postmortem BMI introduces error into the re-
- 30. lationship between BMI and knee OA, such error is likely to have been systematic rather than specific to a particular time period. Third, although it is reasonable to infer that the postindustrial in- dividuals studied here were, on average, less physically active and consumed more proinflammatory diets than those from earlier periods (39), direct data on these and other potential risk factors are not available for the individuals studied. Fourth, although socio- economic status was undocumented for individuals in this study, the early industrial group likely included more relatively low- income individuals than the postindustrial group. This differ- ence, however, partly reflects important sociodemographic shifts that occurred across the epidemiological transition be- tween time periods (40). Fifth, BMI was unknown for pre- historic individuals, and although sex is reliably determined, age estimates beyond 50 y old are imprecise. Thus, the prehistoric samples could not be included in regression models that used age and BMI as predictor variables, and although the modal age of adult death in living hunter-gatherers is 68–78 y old (41), we cannot reject the hypothesis that knee OA levels are lower among prehistoric individuals than among postindustrial individuals, partly because prehistoric individuals were, on average, younger or had lower BMIs. Although the causes of OA in general and knee OA in partic- ular are still not fully understood, the most important conclusion
- 31. Earl y ind ustr ial Po sti nd us tria l 0 5 10 15 20 25 50 55 60 65 70 75 80 Age (Years) K n e e
- 32. O A p re va le n ce ( % ) Fig. 2. Age-related change in knee OA prevalence controlling for BMI, sex, and ethnicity. Shading represents 95% CIs. Wallace et al. PNAS | August 29, 2017 | vol. 114 | no. 35 | 9335 A N TH R O P O LO G Y
- 33. Jennifer Highlight Jennifer Sticky Note (highlighted in light blue) The last major section is the 'Discussion'; this is typically the most interesting section when reading a research report because it discusses the results presented. That is, it places the results in the context of the research questions, discusses their similarities/differences to previous research results, and attempts to explain why the results occurred. Discussion sections also tend to allocate some time to discussing limitations of their research study, and/or next steps/further analyses that could be explored for greater understanding. For the purpose of our assignment, reading the discussion might be helpful in attempting to understand the results/comparisons made, as well as any concerns/limitations the researchers identified with their data. of this study is that the recent increase in knee OA levels cannot simply be considered an inevitable consequence of people living longer, but instead is the result of modifiable risk factors, in- cluding but not limited to high BMI, that have become more common since the mid-20th century. From an evolutionary perspective, knee OA thus fits the criteria of a “mismatch dis- ease” that is more prevalent or severe because our bodies are inadequately or imperfectly adapted to modern environments (39). Intriguingly, other well-studied mismatch diseases, such as hypertension, atherosclerotic heart disease, and type 2 diabetes (39), that also have become epidemic during the last few
- 34. decades are strongly associated with knee OA (42), suggesting com- mon causes and risk factors. Susceptibility to knee OA and other mismatch diseases is undoubtedly influenced by intrinsic factors, including age, sex, and genes, but the historical and evolutionary perspective afforded by our data underscores that many modern cases of knee OA may be preventable. Prevention, however, will require a reappraisal of potential risk factors that have emerged or intensified only very recently. As with other mismatch dis- eases, it is likely that any effective prevention strategy will in- volve adjusting physical activity patterns and diets to approximate more closely the lifestyle conditions under which our species evolved. ACKNOWLEDGMENTS. We thank the curatorial staffs of institutions housing the skeletal collections analyzed, including the American Museum of Natural History, the Cleveland Museum of Natural History, the Department of Anthropology at San Jose State University, the Forensic Anthropology Center at the University of Tennessee, the Maxwell Museum of Anthropol- ogy at the University of New Mexico, the National Museum of Natural History, the Peabody Museum at Harvard University, and the W. S. Webb Museum of Anthropology at the University of Kentucky. We also thank Michèle Morgan for providing age estimates for the prehistoric
- 35. skeletons from New Mexico, and Ashley Brennaman for providing data used to assess interobserver agreement for eburnation identification. This work was sup- ported by the Hintze Family Charitable Foundation and the American School of Prehistoric Research (Harvard University). 1. Murray CJ, et al. (2013) The state of US health, 1990-2010: Burden of diseases, injuries, and risk factors. JAMA 310:591–608. 2. Vos T, et al. (2012) Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2163–2196. 3. Lawrence RC, et al. (2008) Estimates of the prevalence of arthritis and other rheumatic con- ditions in the United States. Part II. Arthritis Rheum 58:26–35. 4. Felson DT (2013) Osteoarthritis as a disease of mechanics. Osteoarthritis Cartilage 21:10–15. 5. Robinson WH, et al. (2016) Low-grade inflammation as a key mediator of the path- ogenesis of osteoarthritis. Nat Rev Rheumatol 12:580–592. 6. Bijlsma JWJ, Berenbaum F, Lafeber FPJG (2011) Osteoarthritis: An update with rele- vance for clinical practice. Lancet 377:2115–2126. 7. Nguyen US, et al. (2011) Increasing prevalence of knee pain and symptomatic knee
- 36. osteoarthritis: Survey and cohort data. Ann Intern Med 155:725–732. 8. Felson DT, et al. (2000) Osteoarthritis: New insights. Part 1: The disease and its risk factors. Ann Intern Med 133:635–646. 9. Loeser RF, Collins JA, Diekman BO (2016) Ageing and the pathogenesis of osteoar- thritis. Nat Rev Rheumatol 12:412–420. 10. Wluka AE, Lombard CB, Cicuttini FM (2013) Tackling obesity in knee osteoarthritis. Nat Rev Rheumatol 9:225–235. 11. Cross M, et al. (2014) The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis 73:1323–1330. 12. Rogers J, Dieppe P (2003) Paleopathology of osteoarthritis. Osteoarthritis, eds Brandt KD, Doherty M, Lohmander LS (Oxford Univ Press, Oxford), 2nd Ed, pp 57–65. 13. Larsen CS (1982) The anthropology of St. Catherines Island. 3. Prehistoric human bi- ological adaptation. Anthropol Pap Am Mus Nat Hist 57:162– 270. 14. Waldron HA (1991) Prevalence and distribution of osteoarthritis in a population from Georgian and early Victorian London. Ann Rheum Dis 50:301– 307. 15. Rogers J, Dieppe P (1994) Is tibiofemoral osteoarthritis in the knee joint a new dis-
- 37. ease? Ann Rheum Dis 53:612–613. 16. Webb S (1995) Palaeopathology of Aboriginal Australians: Health and Disease Across a Hunter-Gatherer Continent (Cambridge Univ Press, Cambridge, UK). 17. Inoue K, et al. (2001) Prevalence of large-joint osteoarthritis in Asian and Caucasian skeletal populations. Rheumatology (Oxford) 40:70–73. 18. Phenice TW (1969) A newly developed visual method of sexing the os pubis. Am J Phys Anthropol 30:297–301. 19. Lovejoy CO, Meindl RS, Pryzbeck TR, Mensforth RP (1985) Chronological meta- morphosis of the auricular surface of the ilium: A new method for the determination of adult skeletal age at death. Am J Phys Anthropol 68:15–28. 20. Murray KA, Murray T (1991) A test of the auricular surface aging technique. J Forensic Sci 36:1162–1169. 21. Pritzker KP, et al. (2006) Osteoarthritis cartilage histopathology: Grading and staging. Osteoarthritis Cartilage 14:13–29. 22. Cockburn A, Duncan H, Riddle JM (1979) Arthritis, ancient and modern: Guidelines for field workers. Henry Ford Hosp Med J 27:74–79. 23. Jurmain R (1999) Stories from the Skeleton: Behavioral Reconstruction in Human
- 38. Osteology (Gordon and Breach, Amsterdam). 24. Waldron T (2009) Paleopathology (Cambridge Univ Press, Cambridge, UK). 25. Kellgren JH, Lawrence JS (1957) Radiological assessment of osteo-arthrosis. Ann Rheum Dis 16:494–502. 26. Waldron T, Rogers J (1991) Inter-observer variation in coding osteoarthritis in human skeletal remains. Int J Osteoarchaeol 1:49–56. 27. Morgan SL, Winship C (2015) Counterfactuals and Causal Inference (Cambridge Univ Press, Cambridge, UK), 2nd Ed. 28. Ho DE, Imai K, King G, Stuart EA (2007) Matching as nonparametric preprocessing for reducing model dependence in parametric causal inference. Polit Anal 15:199–236. 29. R Core Team (2016) R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, Vienna). 30. Valdes AM, et al. (2011) The GDF5 rs143383 polymorphism is associated with osteoarthritis of the knee with genome-wide statistical significance. Ann Rheum Dis 70:873–875. 31. Davis MA, Ettinger WH, Neuhaus JM, Cho SA, Hauck WW (1989) The association of knee injury and obesity with unilateral and bilateral osteoarthritis of the knee. Am J Epidemiol 130:278–288.
- 39. 32. Radin EL, Orr RB, Kelman JL, Paul IL, Rose RM (1982) Effect of prolonged walking on concrete on the knees of sheep. J Biomech 15:487–492. 33. Kerrigan DC, Todd MK, Riley PO (1998) Knee osteoarthritis and high-heeled shoes. Lancet 351:1399–1401. 34. Kiviranta I, Tammi M, Jurvelin J, Säämänen A-M, Helminen HJ (1988) Moderate running exercise augments glycosaminoglycans and thickness of articular cartilage in the knee joint of young beagle dogs. J Orthop Res 6:188–195. 35. Urquhart DM, et al. (2011) What is the effect of physical activity on the knee joint? A systematic review. Med Sci Sports Exerc 43:432–442. 36. Roos EM, Herzog W, Block JA, Bennell KL (2011) Muscle weakness, afferent sensory dysfunction and exercise in knee osteoarthritis. Nat Rev Rheumatol 7:57–63. 37. Handschin C, Spiegelman BM (2008) The role of exercise and PGC1α in inflammation and chronic disease. Nature 454:463–469. 38. Giugliano D, Ceriello A, Esposito K (2006) The effects of diet on inflammation: Em- phasis on the metabolic syndrome. J Am Coll Cardiol 48:677– 685. 39. Lieberman DE (2013) The Story of the Human Body: Evolution, Health, and Disease (Pantheon, New York).
- 40. 40. Floud R, Fogel RW, Harris B, Hong SC (2011) The Changing Body: Health, Nutrition, and Human Development in the Western World Since 1700 (Cambridge Univ Press, Cambridge, UK). 41. Gurven M, Kaplan H (2007) Longevity among hunter- gatherers: A cross-cultural ex- amination. Popul Dev Rev 33:321–365. 42. Zhuo Q, Yang W, Chen J, Wang Y (2012) Metabolic syndrome meets osteoarthritis. Nat Rev Rheumatol 8:729–737. 43. Church TS, et al. (2011) Trends over 5 decades in U.S. occupation-related physical activity and their associations with obesity. PLoS One 6:e19657. 44. Tudor-Locke C, Ainsworth BE, Washington TL, Troiano R (2011) Assigning metabolic equiva- lent values to the 2002 census occupational classification system. J Phys Act Health 8:581–586. 45. Omran AR (1971) The epidemiologic transition. A theory of the epidemiology of population change. Milbank Mem Fund Q 49:509–538. 46. Gaziano JM (2010) Fifth phase of the epidemiologic transition: The age of obesity and inactivity. JAMA 303:275–276. 47. National Center for Health Statistics (2000) Leading Causes of Death, 1900-1998. Available at https://www.cdc.gov/nchs/data/dvs/lead1900_98.pdf. Accessed
- 41. June 15, 2017. 48. Jones DS, Podolsky SH, Greene JA (2012) The burden of disease and the changing task of medicine. N Engl J Med 366:2333–2338. 49. Brennaman AL (2014) Examination of Osteoarthritis for Age-at-Death Estimation in a Modern Population. MS thesis (Boston Univ School of Medicine, Boston). 50. Cohen J (1960) A coefficient of agreement for nominal scales. Educ Psychol Meas 20:37–46. 51. Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174. 52. Gelman A, Hill J (2007) Data Analysis Using Regression and Multilevel/Hierarchical Models (Cambridge Univ Press, Cambridge, UK). 53. Austin PC, Stuart EA (September 1, 2015) Estimating the effect of treatment on binary outcomes using full matching on the propensity score. Stat Methods Med Res. 54. Stuart EA (2010) Matching methods for causal inference: A review and a look for- ward. Stat Sci 25:1–21. 55. Ho DE, Imai K, King G, Stuart EA (2011) MatchIt: Nonparametric preprocessing for parametric causal inference. J Stat Softw 42:1–28.
- 42. 9336 | www.pnas.org/cgi/doi/10.1073/pnas.1703856114 Wallace et al. https://www.cdc.gov/nchs/data/dvs/lead1900_98.pdf www.pnas.org/cgi/doi/10.1073/pnas.1703856114 Jennifer Highlight Jennifer Sticky Note (highlighted in gray) At the end of the report, you'll find the literature cited (References) section; this typically follows an Acknowledgments section and possibly some other minor sections. You would have noticed that the researchers reference ideas, data, methodology, and arguments from other researchers throughout the research report. The Literature Cited section provides the content on those citations, in a format required by the publication. For our purposes, you need not review the information in the Literature Cited unless you read something in the research report that interests you and you want to look up more content on it for your own purposes! Stat 1023/2037A – FW19 Assignment 2 Assignment 2: Clarifying Statistical Research Introduction
- 43. Throughout this course, we discuss ways in which data and statistical analysis could be manipulated or reported in manners which may be deceptive, or in the least, ambiguous. We focus on learning foundational concepts in statistics to equip you with the background necessary to ask the ‘right questions’ before making decisions based on the results of research encountered in your schooling, life, and/or careers. One way to demonstrate your understanding of statistical concepts is to interpret and explain research characteristics in layperson’s language. This assignment, therefore, is set up to evaluate your ability to apply these skills. Learning Objectives • Demonstrate an understanding of statistical vocabulary and concepts when presented in an original research report; • Experience the process of searching for, and reading the original research report upon which a media story is based; • Accurately explain statistical concepts and background using non-statistical language within a novel context. Assignment Media presents the results of statistical research in short articles that are read by the general public; we refer to these articles as ‘media stories’ in our course. However, these stories often summarize only key results (with little content on context and/or sampling and study design) to present a more sensational
- 44. story. As a consequence, relevant information and details— necessary to make rational decisions based on the research—are typically lacking. Your assignment is to take one of the following media stories, find the original published source, and rewrite the media story (using language suitable for a layperson) to make it more informative. Steps to complete the assignment 1. Choose one of the following media stories; it’s a good idea to read through all three options before settling on which one you will work with. A keyword for each media story has been provided to help when you are uploading your Assignment to Gradescope: Option 1: altruism “We’d rather harm ourselves than others, electric shock study finds.” https://www.tvnz.co.nz/one-news/world/wed-rather-harm- ourselves-than-others-electric- shock-study-finds Option 2: pregnant “Pregnant women with morning sickness are more likely to use marijuana: Study” https://www.huffingtonpost.ca/2018/08/22/marijuana- pregnancy- study_a_23507102/?utm_hp_ref=ca-living
- 45. https://www.tvnz.co.nz/one-news/world/wed-rather-harm- ourselves-than-others-electric-shock-study-finds https://www.tvnz.co.nz/one-news/world/wed-rather-harm- ourselves-than-others-electric-shock-study-finds https://www.huffingtonpost.ca/2018/08/22/marijuana- pregnancy-study_a_23507102/?utm_hp_ref=ca-living https://www.huffingtonpost.ca/2018/08/22/marijuana- pregnancy-study_a_23507102/?utm_hp_ref=ca-living admin 高亮 Stat 1023/2037A – FW19 Assignment 2 Option 3: sex “Those good vibes you feel after sex can last for 48 hours, study finds” https://www.huffingtonpost.ca/entry/those-good-vibes-you- feel-after-sex-can-last-for-48- hours-study-finds_n_58d3f3b2e4b0b22b0d1aa255 2. Read the media story very carefully so you understand all the information that it contains. As you read, note any information about the source of the research (e.g. researcher names/affiliations, original publication source, keywords for the research objective/variables, etc.). 3. Think carefully about the information provided in the media story and what is missing or ambiguous, or what you still have questions about regarding the study. That is, using what you’ve learned in this course, try to identify what information
- 46. or details someone reading the media story would need to know about the sampling/study design and results to make informed decisions based on the research. 4. Find the original research report describing the study (i.e. the primary source or research article); use the information about the source of the research that you noted in step 2 to help in this search. If you’re not sure you’ve found the original research report, take a look at the ‘example of an original research report’ that was posted alongside this instruction file. The example also provides some descriptions of what’s included in a research report and how to approach reading one. Be careful: Sometimes, a researcher has published several research reports about a particular topic. When you are looking for the original research report for this assignment, be sure to see if the report you find actually matches the information described in the media story. If you aren’t certain, ask! It’s better to double check before trying to write your assignment based on the wrong report! 5. Read the original research report with the purpose of finding the information/clarification you identified as lacking in step 3. Make notes on this information in your own words.
- 47. Note: research reports often use a lot of discipline-specific jargon and complex statistical analysis. Do NOT get bogged down or discouraged by the language of the research article. Stay focused on understanding the information necessary to explain what the researchers did and what were the results. Again, if you need help, ask! 6. Once you’ve done this background work, you can write your assignment according to the description/format detailed below. Assignment Description Write your own version of the media story, providing enough detail/information about the study design/results so that readers of your version would have the necessary content to make informed decisions about the study’s conclusions. In essence, you should create a ‘fair’, unambiguous version of the media story. However, you must write the details/information in non-statistical jargon (i.e. layperson’s terms) such that an individual with no background in statistics would understand (you can assume that the person has typical high school math knowledge, if necessary). As well, keep in mind that you are writing a media story (i.e. which tends to be more conversational and sensational in tone), and not simply summarizing the research. Consequently, you should be creative (e.g. changing the title, making up answers from interviews with the researchers, using humour, etc.) provided your resulting
- 48. admin 高亮 admin 高亮 admin 高亮 admin 高亮 admin 高亮 admin 高亮 Stat 1023/2037A – FW19 Assignment 2 media story is accurate (i.e. correctly discusses the research and findings…refer back to the learning objectives for this assignment). At the end of your assignment, include a citation to the original research article on which the media story is based. You may use any reference formatting format you are familiar with, provided it gives full information about the article. For example, the following would be a suitable format: Galperin, A., Haselton, M.G., Frederick, D.A., Poore, J., von Hippel, W., Buss, D.M., and G.C. Gonzaga.
- 49. 2012. Sexual regret: Evidence for evolved sex differences. Archives of Sexual Behavior 42(7): 1145-1161. Doi: 10.1007/s10508-012-0019-3 Your assignment must follow these formatting criteria (see the Example assignment): -and-a-half single-sided, 8.5” x 11” pages. Any additional content may not be graded. etc.). Black font only, please. (i.e. top, bottom, left, right) complete sentences, using proper English punctuation, spelling, and grammar. Have someone who is not in our course edit it for you. this, ask for help! Marking Scheme Your assignment will be graded based on the following criteria: ✓ Adherence to ‘Format’ criteria described above (4 marks); ✓ Evidence of understanding and accuracy of description of the original research study design and results (4 marks); ✓ Appropriate ‘voice’ for a media story (i.e. use of non- statistical vocabulary that a non-statistics
- 50. student would understand; maintaining the tone of a media story as opposed to a research article or summary of research) (3 marks); ✓ Inclusion of original article citation at the end of your assignment (2 marks); Questions you should ask yourself before submitting: study design, and results needed to make the media story better/more informative? Have I missed any relevant ideas/information that would be necessary to make an informed opinion on the research described in the media story? demonstrating I understand the study design and results? media story written in language that someone who has not taken statistics would understand? a summary of research? (remember, you are just writing a new version of the media story that is more informative—it still is meant to attract attention and/or be entertaining) spelling, and had someone else not in statistics edit it?
- 51. ave I included the citation for the original article at the end of my assignment? admin 高亮 admin 高亮 admin 高亮 admin 高亮 admin 高亮 admin 高亮 admin 高亮 Stat 1023/2037A – FW19 Assignment 2 Note Carefully: As you are working on your assignment, email it to yourself occasionally, or save a copy on a USB key or to a ‘Cloud’ (e.g. Dropbox). Don’t put yourself in a situation where your computer crashes and you lose your work right before the
- 52. deadline. Writing in your own words One of the major challenges of this assignment—or any situation in which you must describe something someone else has already done—is writing in your own words. You will be working with two pieces of writing from other individuals, (i) the original media story, and (ii) the original research report, in order to make your own piece of writing. In this type of situation, it can be very easy to (accidentally or otherwise) use the pieces of the other writing in your own, especially if you take notes on the story/report by copying sentences into your own file. To avoid getting into this situation, I suggest the following strategies: • Writing something in your own words based on information from other people’s words takes some work and time—especially when you have to understand the content of an original research report written for discipline experts; • Read the original media story several times so that you know what it talks about without looking at the actual page; this means you won’t really have to look back at the media story again for reference when reading the original research report, or when writing your own version of the media story (which will limit the opportunity to use the media story’s phrasing); • Make notes on the original research report in your own words. It is SO tempting to just copy relevant phrases into your notes as you read, with the purpose
- 53. of collecting the relevant information for rewording later. But, as time passes you might find yourself in two situations: (i) you might forget what is your words versus copied from the report, and (ii) you might be pressed for time and struggle to rephrase your notes. If your notes are always in your own words, you’ve already done the hard work! In the end, it’s always easier to write something in your own words if you’ve worked hard to understand the research you’ve been reading. If you understand it, you can write freely from your memory, without referring to any notes (whether those notes are your words, or from the original sources). Comment on Referencing For the purpose of this assignment, you should not need to make any references/citations within your writing except the inclusion of the citation for the original research article. The content of your assignment will be based on the media story you chose (and associated original research report) and the textbook/lecture material presented in this course. You can assume I know that the material you are presenting is from these sources. You do have the freedom to ‘make up’ quotations from the researchers; use standard quotation format (e.g. refer back to how quotes from researchers are typically formatted in the media story). You can assume I know that any quotes you include are made up for the purpose of making your media story more interesting/creative. There should be no reason to quote directly from the original research report OR the media story;
- 54. consequently, you should not be using any true quotes (beyond what you have ‘made up’ to maintain a media story tone) in your assignment. Stat 1023/2037A – FW19 Assignment 2 How to submit this assignment: Your assignment is submitted digitally (i.e. not on paper) in TWO (2) places. You need to submit to BOTH of these portals: 1. On OWL, through the “Assignment (OWL submissions)” tool. 2. On Gradescope. You were emailed an account set up email to your UWO email address on September 29. Follow that email to set up your Gradescope account, and to submit your assignment. Academic Integrity and Plagiarism You must complete this assignment on your own and in your own words; no collaboration with peers is permitted at any stage of the assignment. Your assignment will be automatically submitted to Turnitin (as per the course syllabus) for an originality report when you submit your assignment through our OWL website as described above (you do not have to and must not separately submit your assignment to Turnitin). What does Turnitin do?
- 55. Turnitin compares the content of the assignment you submit against websites, online databases and repositories of past assignments submitted to Western as well as other universities. It checks for ‘textual similarity’ between your assignment and these databases/repositories by matching similar phrases and sentences. It then generates an ‘originality report’ for your assignment, which indicates the percentage of your assignment which has textual similarity to other sources. An originality report of 100% indicates your entire assignment was copied from other sources. Why use Turnitin for Stat 1023/2037? Turnitin is being used to ensure that students complete and write their assignments in their own words. This is relevant to Stat 1023/2037 as this assignment is part of your course mark; the work you submit should reflect YOUR understanding and ability. How does my Turnitin ‘originality report’ affect my mark for Stat 1023/2037? If you have written your assignment in your own words, your submission to Turnitin shouldn’t affect your mark on the assignment at all! In the event that the analysis provided by Turnitin indicates a high degree of textual similarity, the situation will be dealt with as described in the University’s procedure for handling scholastic offences (see the Western Academic Calendar). Now I’m worried that I don’t know what plagiarism is or whether I’m paraphrasing correctly. Help! If you are concerned about whether you are paraphrasing information correctly or adequately, or are uncertain what writing practices constitute plagiarism, ask for
- 56. help! Just be sure to ask for this help with plenty of time before the submission deadline! Need help on the assignment? • If you don’t fully understand what you need to do for this assignment: o post a question to the Forum under ‘Assignment 2’ (be sure to use an informative title!); o come to our course drop-in hours to ask for clarification and/or help. • If you aren’t sure what constitutes plagiarism, find out! There are plenty of resources available: o come to our course drop-in hours; Stat 1023/2037A – FW19 Assignment 2 o speak with a librarian at the Research Help desk and/or review the information on plagiarism from the Western libraries (http://www.lib.uwo.ca/tutorials/plagiarism); o check out this website: http://www.plagiarism.org/plagiarism- 101/what-is-plagiarism/ • If you need help with spelling, grammar, punctuation, editing a draft, clarity, style, or writing in general, visit the Writing Support Centre (http://www.sdc.uwo.ca/writing/). The people and services available are a great resource for writers of all skill levels. They have individual
- 57. appointments as well as drop-in hours (see the website for information). • If you don’t know how to set the preferences on your computer software (e.g. Microsoft Word, etc) so that the margins, line spacing, etc are correct, ask for help during our course drop-in hours or on the Forum; • If you need help finding the original research report or obtaining access to the report, Western’s library team can help! Their research help site www.lib.uwo.ca/services/research_help.html is a good place to start; it even has videos on how to get full text versions of original articles. You might also have success walking in to one of the libraries and asking for help at the research desk. Alternatively, if you are struggling with finding information about the original research report in the first place, stop by our course drop-in hours for help. • If you need help writing a citation for the original research report (i.e. identifying what the components of a citation are), just ask! Post to the Forums, or come to drop-in hours. • If you have any other questions, just ask! Come to drop-in hours, or use the Forums. http://www.lib.uwo.ca/tutorials/plagiarism http://www.plagiarism.org/plagiarism-101/what-is-plagiarism/