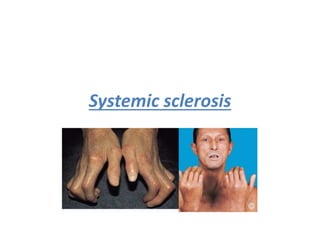
2. Definition; It is a chronic autoimmune disease condition of unknown
etiology characterized by increased
• fibroblast activity and fibrosis in a number of different organ
systems in the form of hardened,
• sclerotic skin and other connective tissues.
• It is 4 times more common in females.
There are three patterns of disease:
• 1) Limited cutaneous systemic sclerosis:
• Raynaud's may be first sign
• Scleroderma affects face and distal limbs predominately
• Associated with anti-centromere antibodies
• CREST syndrome is an older term for the limited cutaneous form.
• CREST syndrome is a subtype of limited cutaneous systemic
sclerosis: Calcinosis, Raynaud's
• phenomenon, Esophageal dysmotility, Sclerodactyly, Telangiectasia
3. Complications of CREST syndrome:
Malabsorption can develop in these patients secondary
to bacterial overgrowth of the sclerosed
• small intestine (dysmotility secondary to infiltration of
the intestinal wall with fibrous tissue).
• Also, unfortunately pulmonary hypertension is one of
the more common late complications seen
• in such patients.
• It is often difficult to distinguish between interstitial
lung disease and pulmonary hypertension as the
• cause of breathlessness in systemic sclerosis
4. • NB: Lung involvement is a frequent complication of systemic
sclerosis, and can be split into 2 main
• syndromes:
• 1- pulmonary vascular disorder evolving over time into relatively
isolated pulmonary
• hypertension
• 2- interstitial lung disease.
• 2) Diffuse cutaneous systemic sclerosis
• Scleroderma affects trunk and proximal limbs predominately
• Associated with scl-70 antibodies
• Hypertension, lung fibrosis and renal involvement seen
• Poor prognosis
• Whilst diffuse systemic sclerosis is associated with more severe and
rapid internal organ
• involvement it is also seen in the limited form.
5. • 3) Morphea (Localized Scleroderma) (without internal
organ involvement)
• tightening and fibrosis of skin
• May be manifest as plaques (morphoea) or linear.
• This is a well-defined oval to round plaque. (Like a painless
lesion to his left subcostal region,
• dry, indurated and slightly coarse to palpation).
• The pathogenesis is poorly defined.
• An autoimmune component is suggested by enhanced T
helper 2 (Th2) dependent interleukin 4
• (IL-4) activity, which in turn up regulates transforming
growth factor beta (TGF -beta). TGF-beta
• stimulates fibroblast production of collagen and other
extracellular matrix proteins.
6. Presentation:
• Typical patient is a young female (35-65); Male: female ratio of about 1:4; Prevalence about 10-20
per 100000
• in the population
• Onset: Initial symptoms are typically non-specific and include Raynaud’s phenomenon, fatigue, and
• musculoskeletal complaints.
• The first specific clue is skin thickening that begins as swelling or puffiness of the fingers and hands.
• The patient feels a progressive tightening of the skin and decreased flexibility.
• In diffuse SSC various degrees of hypo or hyper pigmentation may occur giving the skin a tanned or
• “salt and pepper” appearance.
• Limited SSc (L-SSc): Usually have RP for 1-10 years prior to onset; skin involvement is distal to the
• elbows and knees but may involve the face.
• Diffuse SSc (d-SSc): Short interval between onset of RP and skin involvement which includes the
trunk
• & extremities
7. Progression:
• As SSc progresses the skin becomes progressively tighter and
thicker. This stage may persist for one to
• three years, after which the skin tends to soften and either thins
(becomes atrophic and thinned, with
• tethering to underlying structures) or returns toward normal
texture. After this initial improvement
• the disease may be progressive.
• Constitutional Features: Fatigue may be prominent, weight loss due
to activity of the disease and GI
• involvement with anorexia.
• Functional Status: Reduced functional status with difficulties with
ADLs; Difficulty at work; Loss of
• libido - Erectile dysfunction in men is common; Depression in up to
50%
8. Review of systems:
• Vascular: Raynaud’s Phenomenon (RP): Present in 95% of patients with SSc vs 4%
of general
• population; In SSC, RP is associated with tissue fibrosis of the fingers, loss of the
digital pads, digital
• ulceration, and on occasion digital ischemia with amputation
• Musculoskeletal: Arthralgias and myalgias are one of the earliest symptoms; A
rheumatoid-like
• erosive polyarthritis is occasionally seen (<20%); Inflammation and fibrosis of the
tendon sheaths also
• lead to pain and restriction of movement with accompanying tendon friction rubs;
Muscle weakness
• and atrophy is a dominant problem in late SSc secondary to fibrosis, disuse,
contractures of fibrotic
• skin, along with malnutrition
• Mucocutaneous: Xerostomia and xerophthalmia
• Neurologic: Trigeminal neuralgia; Other entrapment neuropathies such as carpal
tunnel
• Cardiac: Pericardial effusions; Myocardial fibrosis with diastolic dysfunction;
Premature coronary
• artery disease
9. • Respiratory: Leading cause of mortality in SSc;
• (a) Interstitial Fibrosis: Occurs with diffuse disease (30-60%), anti-topoisomerase-1
antibodies (Scl-70),
• and FVC<75 early in the course of disease;
• (b) Pulmonary hypertension without fibrosis occurs in 20-25% of limited SSc
patients and less often in
• diffuse disease: Risk factors include long standing RP and limited SSc; Poor survival
- 90% were dead at
• 5 years; Pulmonary arterial pressures (PAP) >45 with right sided heart changes
correlate with
• catheterization in 90% of cases. Right heart catheterization should be done in all
cases to confirm the
• diagnosis.
• Gastrointestinal: Small oral aperture; Dental disease and oral sicca features;
Esophageal dysmotility
• with resulting GERD; Gastric ectasia (watermelon stomach); Pseudo obstruction
secondary to small
10. .
• Respiratory: Leading cause of mortality in SSc;
• (a) Interstitial Fibrosis: Occurs with diffuse disease (30-60%), anti-
topoisomerase-1 antibodies (Scl-70),
• and FVC<75 early in the course of disease;
• (b) Pulmonary hypertension without fibrosis occurs in 20-25% of limited
SSc patients and less often in
• diffuse disease: Risk factors include long standing RP and limited SSc; Poor
survival - 90% were dead at
• 5 years; Pulmonary arterial pressures (PAP) >45 with right sided heart
changes correlate with
• catheterization in 90% of cases. Right heart catheterization should be
done in all cases to confirm the
• diagnosis.
• Gastrointestinal: Small oral aperture; Dental disease and oral sicca
features; Esophageal dysmotility
• with resulting GERD; Gastric ectasia (watermelon stomach); Pseudo
obstruction secondary to small
• Renal : one of the main causes of death is hypertensive renal crisis ,
characterized by rapidly developing accelerated phase hypertension and
renal failure , much more likely to occur in DCSSCL
11. INVESTIGATIONS:
CBC: Thrombocytopenia and microangiopathic hemolysis (schistocytes) with
renal crisis.
• Urinalysis: Proteinuria with renal crisis
• Creatinine: May be elevated with renal crisis
• Elevated AST/ALT/ALP: Think PBC associated with L-SSc
• ANA: In majority of cases
• Anti-Topoisomerase-1 (Scl-70): Diffuse SSc associated with interstitial
pulmonary fibrosis
• Anti-centromere antibodies: Limited SSc
• Anti-Polymerase-III: Diffuse SSc associated with cardiac or renal disease
• Radiology: Soft-tissue calcification; Usually a non-erosive arthritis with
deformities secondary to
contraction of the overlying skin; Reported cases of erosive arthritis
Screening (yearly): Chest radiographs; ECG & echocardiogram; Pulmonary
function test
13. management:
• Disease Modifying Interventions: Methotrexate -
Possible favorable outcome in skin; D-Penicillamine,
chlorambucil, and interferon-alpha have not been
fruitful
• Treatment of Skin Disease: Topical moisturizers; Treat
ulcers with anti-septic, antibiotic ointments,
and analgesics; Calcinosis - Can try colchicine
• Raynaud’s Phenomenon: Avoid cold and keep warm
(socks, hat, scarf, gloves); Stop smoking; Avoid
estrogen containing compounds; Calcium channel
blockers; Topical nitroglycerin paste; IV iloprost
14. .
• Gastrointestinal: Reduce caffeine and alcohol, stop
smoking, elevate head of the bed, avoid foods
which precipitate GERD, eat frequent small meals; Oral
antacids, H2 blockers, and proton pump
inhibitors; Metoclopromide, erythromycin, or
domperidone for dysmotility; Broad spectrum
antibiotics; Supplemental vitamins
• Cardiopulmonary: cyclophosphamide is effective in
slowing progression of interstitial lung disease and
similar result observed with MMF. More recently the
tyrosine kinase inhibitor nintedanib ( 150mg twice
daily has shown efficacy in slowing decline of lung
function in DCSSCL
15. Scleroderma Renal Crisis management:
• Control blood pressure: Discontinue any medications which may
worsen blood pressure; ACEInhibitors - Have improved survival
from 10% in 1 year to 90% in 5 years. Captopril is most commonly
used aiming to reduce blood pressure slowly. Dose 25 mg PO BID-
TID increasing to max 150 mg TID; Angiotensin receptor blockers -
Less effective than ACE (? Lack of bradykinin effect; Calcium channel
blockers; Dialysis and renal care; Consult nephrology; Continue ACE
during dialysis as persistent hyperreninemia may occur; Supportive
• Treatment: Consult cardiology if CHF is an issue; Oxygen; Careful
use of diuretics; Nitrates; Statins; Neurology involvement if
associated encephalopathy or seizures; Correct electrolyte
abnormalities
• Musculoskeletal: Physiotherapy - Early and aggressive to prevent
joint contractures; Acetaminophen; NSAIDs and COXIBs;
Methotrexate and corticosteroids for inflammatory myopathies
16. Poor Prognosis:
• Older age
• Diffuse skin disease
• Proteinurea
• High ESR
• Low gas transfer factor for carbon monoxide
• Pulmonary hypertension