2. Patient Identification
36-year-old male
• Chief complaint:
– Unconscious 2 hr PTA
• Present illness:
– Found unconscious on the
footpath, then was
transferred to hospital
– Could not recall the situation
– Deformity Lt. elbow
2
3. Primary Survey
• Vital signs:
– BP 203/111, PR 120, RR 18, SpO2 100 %
• A: Could not talk, on ETT no 7.5, on philadelphia collar
• B: clear and equal breath sound both lungs, SpO2 100%
• C: no active external bleeding, HR 120, BP 203/111
• D: E1VtM4, pupil – Lt. 3 mm RTL, Rt. Could not evaluate
• E: Good sphincter tone, yellow feces, no stepping spine
3
4. Adjunct to Primary survey
• NG: could not insert due to bleeding
• OG: blood clot
• Foley’s catheter: clear and yellow urine
• Extended-FAST: negative
4
5. Secondary Survey
• HEENT:
• - bleeding both nostrils, Rt. ear and oral cavity
• - generalized facial swelling with Rt. periorbital ecchymosis
• - laceration wound 2x2 cm at forehead
5
6. Physical Examination
• Swelling c deformity Lt. elbow
• No open wound
• Could perform full passive ROM Lt.
elbow
• Could not perform active ROM due
to poor level of consciousness
• Radial and ulnar artery 2+, CRT < 2 s
Affected part: Lt. elbow
6
7. Physical Examination
• Marked swelling c deformity Rt. elbow
• No open wound
• Limited passive ROM Rt. Elbow due to
mechanical block
• Loss of Heuter’s line and triangle
• Could not perform active ROM due to
poor level of consciousness
• Radial and ulnar artery 2+, CRT < 2 s
Affected part: Rt. elbow
7
8. Adjunct to Secondary survey
• CT brain NC emergency:
– Hemorrhagic contusion at Lt. occipital lobe
– Rt. Intraventricular hemorrhage
– Subdural hemorrhage Lt. temporal lobe 6 mm thickness
– Panfacial fracture with base of skull fracture (sphenoid and
mastoid)
8
9. Adjunct to Secondary survey
• CT chest:
– No ATAI
– No pneumohemothorax
– No rib fracture, no thoracolumbar spine fracture
9
10. Adjunct to Secondary survey
• CT abdomen:
– No pneumo-hemoperitoneum
– No solid organ injury
10
13. Diagnosis
• Polytraumatized patient
• Closed posterior dislocation Rt. Elbow
• Closed radial head subluxation Lt. elbow with coronoid
fracture (PLRI)
• Severe head injury
– IVH, SDH Lt. temporal lobe
– Panfacial bone fracture c base of skull fracture
14
14. The Terrible Triad
- Elbow dislocations
- Radial head fractures
- Coronoid fractures
Poor outcomes for this injury pattern
- No specific classification
- separate classification for the terrible triad
22
15. Regan and Morrey Fracture Classification
Type I coronoid process tip fracture
Type II fracture of 50% or less of height
Type III fracture of more than 50% of height
23
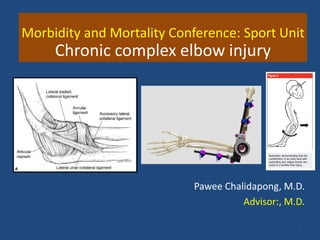
17. Valgus posterolateral Rotatory Injury
▶ Mechanism
▶ Axial load with valgus and supination
▶ Force
▶ Lateral => medial
▶ 1. avulsion LUCL
▶ 2. Radial head fracture
▶ 3. posterior-inferior subluxation with shearing
force => coronoid fracture (usually tip of coronoid
O’Driscoll)
▶ 4. Disrupt of MCL
18. Evaluation
▶ Radiograph
▶ Plain film (AP,lateral elbow)
▶ CT (more accurate for evaluate)
▶ Initial reduction
▶ Apply traction and extension
▶ Flex elbow
▶ Test stability
▶ Pronate forearm with extension If elbow dislocation at
elbow flexion 30 degree => unstable
19. Management
• NeuroSx alert operating theatre immediately
to perform Rt. Frontal ventriculostomy
• Orthopaedics surgeon
– Closed reduction Rt. Elbow at emergency room then
applied long arm slab (90 degrees elbow flexion)
– Closed reduction + applied long arm slab Lt. elbow
27
21. Pitfall
• 1) Late repeat radiographic examinations
– Due to unstable patients
– How to improve?
– 2) Lack of repeated physical examination at ward
– Resulted in chronic subluxation of elbow within slab
– How to improve?
30
25. ▶ Non operative
▶ Full arc of motion with stable elbow joint
(if pronation of forearm then the elbow dislocation at 0-30
degree flexion => operative treatment should be considered)
▶ 7-10 days Splint in 90 degree flexion with pronation with
Isometric exercise
26. Surgical treatment terrible triad
▶ Indication
▶ Residual instability
▶ Contraindication
▶ Medical comorbidities
▶ Non functional upper limb
▶ Address
▶ Radial head fracture
▶ LUCL
▶ Coronoid fragment
▶ ± AMCL
▶ ± External fixation (hinge or static)
28. LUCL
▶ Repaired
▶ Heavy non-absorbable
▶ Suture No.2 through
drill hole => isometric
suture
▶ By anchor suture
29. Coronoid
▶ No concensus for approach
for coronoid fixation
▶ Options
▶ Suture Lasso technique
▶ Small fragment screw
▶ Mini fragment plate
▶ If coronoid < 10% may left
unrepaired if secure
repaired concomitant injury
30. ▶ Is AMCL need to be addressed ?
▶ Elbow is test by
▶ Forearm in neutral position
▶ Gravity extension => if joint remain congruence at 45
degree flexion
=> No need for repaired MCL
▶ IF repaired AMCL =>elbow remain unstable
▶ Hinge or static external fixator should be applied
Green Ed. 6th
31. Treatment
- Most terrible triad injuries require surgery
44
Indications for nonsurgical treatment
- CT documentation of a minimally displaced radial
head fracture without mechanical block
- A coronoid fracture that involves only the tip
- Concentric reduction after relocation
32. Surgical Planning:
• Open reduction
• Adhesion and callus removal
• LUCL and AMCL repair with anchor suture [Smith]
• Applied long arm slab Lt.
• +/- hinge external fixation Lt. elbow
45
34. Advantages
• Concentric reduction of the ulnohumeral joint
• Allow early range of motion
• Aids collateral ligament healing
- maintaining appropriate tension
- limiting capsular retraction
35. Indications
• Persistent instability after attempted
bony and ligamentous repair in the acute
setting
• Chronic elbow instability in delayed
treatment or failed previous treatment
47. Post-operative Care
• Rehabilitation program depend on integrity of
osseous and ligament repaired test at
intra-operative (RW. 8th ed )
• Active ROM in 1-2 days after surgery
• Avoid shoulder in abduction
• Strengthening begin at 6-8 weeks (evidence of
bone healing)
• (Green 6th ed)
69