This document provides guidance on writing informal reports, including their typical parts and format. It discusses the three main parts of any report: introduction, discussion sections, and conclusion. The introduction includes a statement of the problem or situation, the task assigned, and the report's purpose and scope. Discussion sections may include headings, lists, and visuals to break up the text. The conclusion should remind readers of any needed actions and provide contact information. The document also provides an example client report assignment, asking students to document a subjective assessment, objective findings, and actual or potential risk factors for the client.
![Writing Informal Reports
Format
Memo header
To: (name and title of target audience)
From: (name and title of writer: remember to sign or initial if it
isn’t an electronic submission)
Date:
RE:
CC: (distribution list when necessary)
Introduction [No heading necessary]
Discussion sections [Use headings provided in the outline
attachment of the syllabus]
Conclusion [Reflection is the content]
---------------------------------------------------------------------------
-------------------------------------
Parts of an informal report
Reports are written for many different reasons and use two
basic formats. One is the long or formal
report and the short or informal report. But EVERY report, like
every letter, essay, or article has 3
main parts: Introduction, Discussion sections, Conclusion.
These reports follow the same format as the
memo but are longer and more comprehensive. Because they are
longer than one or two pages, reports
also include such formatting elements as headings, bulleted or](https://image.slidesharecdn.com/writinginformalreportsformatmemoheaderto-221118063151-89cfcab2/85/Writing-Informal-Reports-Format-Memo-header-To-docx-1-320.jpg)
![Writing Informal Reports
Format
Memo header
To: (name and title of target audience)
From: (name and title of writer: remember to sign or initial if it
isn’t an electronic submission)
Date:
RE:
CC: (distribution list when necessary)
Introduction [No heading necessary]
Discussion sections [Use headings provided in the outline
attachment of the syllabus]
Conclusion [Reflection is the content]
---------------------------------------------------------------------------
-------------------------------------
Parts of an informal report
Reports are written for many different reasons and use two
basic formats. One is the long or formal
report and the short or informal report. But EVERY report, like
every letter, essay, or article has 3
main parts: Introduction, Discussion sections, Conclusion.
These reports follow the same format as the
memo but are longer and more comprehensive. Because they are
longer than one or two pages, reports
also include such formatting elements as headings, bulleted or](https://image.slidesharecdn.com/writinginformalreportsformatmemoheaderto-221118063151-89cfcab2/75/Writing-Informal-Reports-Format-Memo-header-To-docx-1-2048.jpg)
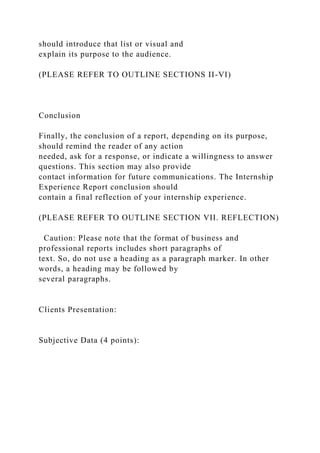


![Format:
· Standard American English (correct grammar, punctuation,
etc.)
http://extmedia.kaplan.edu/nursing/preBSN/Global/APA_Progre
ssionLadder_prelicensureBSN.pdf
Resources:
Chapter 5: SOAP Notes: The subjective and objective portion
only
Sullivan, D. D. (2012).
Guide to clinical documentation. [E-Book]. Retrieved
from
http://ezproxy.rasmussen.edu/login?url=http://search.ebscohost.
com/login.aspx?direct=true&db=nlebk&AN=495456&site=eds-
live&ebv=EB&ppid=pp_91
Smith, L. S. (2001, September). Documentation do’s and don’ts.
Nursing, 31(9), 30. Retrieved from
http://ezproxy.rasmussen.edu/login?url=http://search.ebscohost.
com/login.aspx?direct=true&db=rzh&AN=107055742&site=eds-
live
Documentation Grading Rubric- 10 possible points
Levels of Achievement
Criteria
Emerging
Competence
Proficiency
Mastery
Subjective
(4 Pts)
Missing components such as biographic data, medications, or
allergies. Symptoms analysis is incomplete. May contain
objective data.](https://image.slidesharecdn.com/writinginformalreportsformatmemoheaderto-221118063151-89cfcab2/85/Writing-Informal-Reports-Format-Memo-header-To-docx-6-320.jpg)