Downloaded 48 times



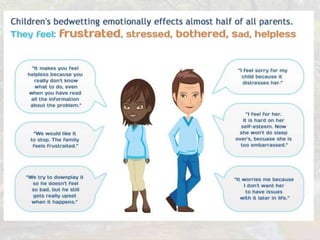





This document presents a case of a 10-year-old girl with monosymptomatic nocturnal enuresis, or nighttime bedwetting without other urinary symptoms. Her examination and tests were normal. The document discusses the diagnosis, causes, and management options for childhood nocturnal enuresis, which commonly includes motivational therapy and enuresis alarms. Medical treatments like desmopressin may also be used but have higher relapse rates after stopping. Referral is recommended if enuresis does not improve after 8-12 weeks of treatment or if other issues are suspected.

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

