This document provides an overview of nocturnal enuresis (bedwetting), including:
- Historical treatments included using animal organs or inducing blisters, with limited effectiveness. Psychic treatment in the 1920s showed an 87% success rate.
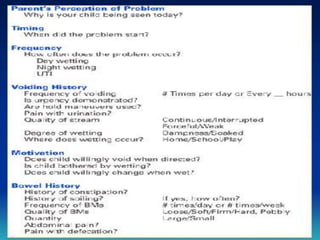
- Enuresis is usually due to a maturational delay and resolves naturally by age 15. Evaluation looks for underlying causes but most cases are primary nocturnal enuresis without other issues.
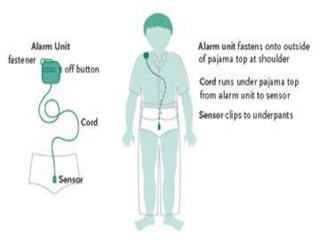
- Treatment focuses on education, behavioral modification using star charts and alarms, and pharmacotherapy like imipramine or desmopressin acetate. The goal is improving self-esteem until natural maturation occurs. A multimodal approach tailored to the












![Paediatric Urology [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/paeduroedmond-140716213023-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

































































