Ventricular Septal Defect
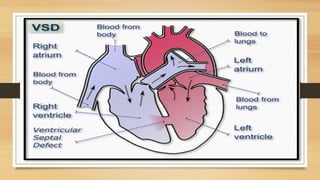
•Abnormalopening between the right and left ventricles.
May be classified according to location: membranous (accounting for 80%) or
muscular.
•May vary in size from a small pinhole to absence of the septum, resulting in a
common ventricle. Frequently associated with other defects, such as pulmonary
stenosis, transposition of the great vessels, patent ductus arteriosus, atrial defects,
and Coarctation of the aorta.
3.
•Many VSDs (20%to 60%) are thought to close
spontaneously. Spontaneous closure is most likely to occur
during the first year of life in children having small or
moderate defects. A left-to-right shunt is caused by the flow
of blood from the higher pressure left ventricle to the lower
pressure right ventricle.
5.
Pathophysiology:
•Because of thehigher pressure within the left ventricle and because
the systemic arterial circulation offers more resistance than the
pulmonary circulation, blood flows through the defect into the
pulmonary artery.
•The increased blood volume is pumped into the lungs, which may
eventually result in increased pulmonary vascular resistance.
6.
Pathophysiology:
•Increased pressure inthe right ventricle as a result of left to right shunting and
pulmonary resistance Causes the muscle to hypertrophy.
•If the right ventricle is unable to accommodate the increased workload, the
right atrium may also enlarge as it attempts to overcome the resistance offered
by incomplete right ventricular emptying. In severe defects Eisenmenger
syndrome may develop.
7.
Clinical manifestations:
•CHF iscommon. There is a characteristic murmur. Patients are at
risk for bacterial endocarditis and pulmonary vascular obstructive
disease. In severe defects Eisenmenger syndrome may develop.
8.
Surgical treatment:
•Palliative: Pulmonaryartery banding (Placing a band around the main
pulmonary artery to decrease pulmonary blood flow) in infants in severe CHF
was common in the past. It is usual now because improvements in surgical
techniques and postoperative care make complete repair in infancy the
preferred approach.
9.
Complete repair (Procedureof choice):
•Small defects are repaired with a purse string approach.
•Large defects Usually require a knitted Dacron patch sewn over the opening.
Both procedures are performed via cardiopulmonary bypass.
•The repair is generally approached through the right atrium and the tricuspid
valve.
•Postoperative complications include residual VSD and conduction
disturbances.
10.
Non-surgical Treatment:
•Device closureduring cardiac catheterization is under clinical trials in some
centers for closure of muscular defects that carry a high operative risk.
•
11.
Prognosis:
•Risks depend onthe location of the defect, number of defects, and other
associated cardiac defects. Single membranous defects have a low mortality;
multiple muscular defects can have a risk of more than 20%.




















































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)















![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)