
Recommended
More Related Content
Similar to 2. Atrial Septal Defect - M.Rafi HAMIDI.ppt
Similar to 2. Atrial Septal Defect - M.Rafi HAMIDI.ppt (20)
Recently uploaded
Recently uploaded (20)
2. Atrial Septal Defect - M.Rafi HAMIDI.ppt
- 1. Presentation by M.Rafi HAMIDI Supervised by Prof. NAJMI, Head of Thoracic Surgery
- 3. Common congenital malformation Acyanotic: a. Atrial septal defect b. Ventricular septal defect c. PDA d. Coarctation of Aorta Cyanotic: a. TOF b. Transposition of great vessels c. Tricuspid atresia
- 4. Atrial Septal defect • ASD is the abnormal opening between the atrium, and it is a left to right shunt
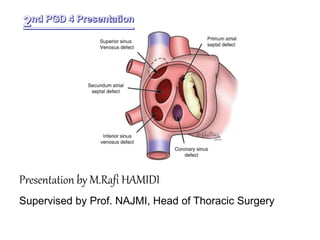
- 5. Types • 3 types: Secundum Primum Sinus venosus
- 6. Types • Primum – affects the lower part of the septum • Secundum – common, affects the upper part of the septum • Sinus venosus – affects the upper part and may be associated with abnormalities of superior vena cava
- 7. Classification by size ASDs can be • Small (3 to <6 mm) • Medium (6 to <12 mm) • Large (>12 mm)
- 8. Incidence • Sex - female : male = 3:1 • 1/1500 live births • Ostium secundum counts for 7% of CHD’s • 100% ASD’s 3mm in diameter • Most of the secundum are associated with Holt- Oram’s syndrome. • Holt–Oram syndrome is a disorder that affects bones in the arms and hands (the upper limbs) and may also cause heart problems
- 10. Pathophysiology Increased left atrial pressure(02 nated blood) Left to right shunt ( no cyanosis) Burden on right side of the heart Increased pulmonary blood flow Pulmonary stenosis / pulmonary HTN Right ventricular hypertrophy Right atrial pressure Right to left shunt cyanosis
- 11. Clinical Features In majority remains asymptomatic Systolic murmer best heard over 2nd & 3rd ICS Dysrrythmias Increased fatigability In older children recurrent chest infection, breathlessness, & bulging of the chest due to enlargement of right ventricle Growth failure in some children
- 13. A hyperdynamic impulse of the right ventricle may be palpated at the lower left sternal border Split S2 Cyanosis in later stages Cardiomegaly Pulmonary vascular emboli Echo shows right ventricular volume overload Cardiac catheterization shows increased 02 content in blood
- 14. Diagnostic measures • Chest X-Ray • ECG • MRI heart • Cardiac catheterization • Intracardiac imaging: with special catheters that are typically placed in the venous system and advanced to the level of the heart. Involves only mild sedation.
- 15. Management • Medical Furosemide 1mg/kg BD Digoxin 5 g/kg BD Potassium chloride 1mq/kg BD Antibiotics
- 16. Surgical closure 1. Cardiopulmonary bypass 2. Purse-string closure 3. Knitted Dacron patch
- 17. Nursing management 1. Identify symptoms 2. Carry out investigations 3. Monitor potassium levels 4. Intake output chart 5. Vital signs 6. Timely administrations of medications 7. Provide rest to decrease O2 demand 8. Psychological support 9. Prevention of infection
- 19. Complications • Pulmonary hypertension & over circulation • Heart failure • Atrial dysrrhythmias • Stroke
- 20. Prognosis • With a small to moderate atrial septal defect, a person may live a normal life span without symptoms. • Larger defects may cause disability by middle age because of increased blood flow and shunting of blood back into the pulmonary circulation.
- 21. Ventricular Septal defect • Abnormal opening between the ventricles • It can be single pin hole opening to absence of membrane • Results in left to right shunt, ultimately right to left shunt.
- 22. Types • Membranous • Muscular- swiss cheese • (Perimembranous- lie in the LV outflow tract just below the aortic valve. • Infundibular- These defects lie beneath the pulmonic valve )
- 23. Incidence • VSD accounts for 25% of CHD’s • Seen in 2-6 / 1000 live births Etiology • unknown
- 24. Pathophysiology Blood from left ventricle right ventricle pulmonary artery Increased pulmonary resistance Increased pressure in right ventricle Right ventricular hypertrophy Enlargement of right ventricle Enlargement of right atrium Eisenmengers syndrome Cyanosis
- 26. Clinical features • Pan systolic Murmur • In large VSD’s Dyspnoea Tachypnea Feeding difficulties Poor growth Profuse perspiration Recurrent pulmonary infections
- 27. Cardiac failure and its symptoms Cyanosis seen on exertion specially while crying Prominence of left precordium Digital clubbing Poor exercise tolerance S2 is split
- 29. Diagnostic evaluation • Hematology for polycythemia • Electrocardiography • Echocardiography/ doppler • Radiographic findings • Cardiac catheterization for 02 saturation
- 30. Management • Small defects no surgical correction but to prevent bacterial endocarditis precautions to be taken • Moderate to large defects surgical closure is needed < 6 months: high risk for surgery usually open heart surgery is done
- 31. • 6 to 24 months: in case of pulmonary hypertension surgery is indicated to prevent development of hypertensive vascular disease • >24 months: depends on pulmonary vascular resistance • Surgical interventions done for small defects are Purse String closure n for large defects Knitted Dacron patch • Clamshell type catheter occlusion devices are tested For closing of apical VSD
- 33. Complication • Residual VSD • Conduction defects • Infection
- 34. Prognosis • Risk depends on Location of defect Number of defects Other associated cardiac defects Single membrane defect have low mortality <5% Multiple defects have a risk of >20%