Downloaded 174 times

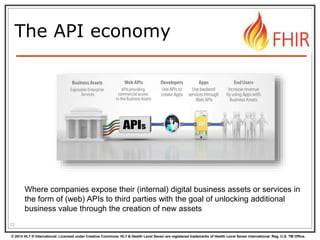
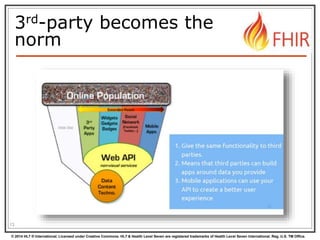



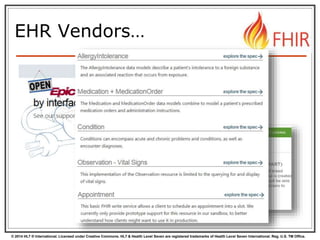


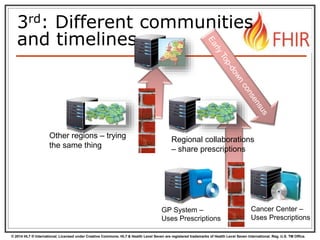



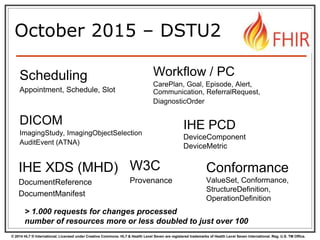


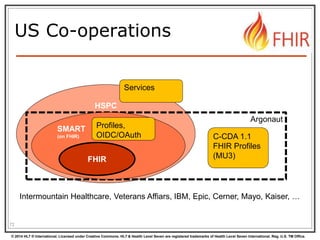




The document introduces HL7's Fast Healthcare Interoperability Resources (FHIR), emphasizing its role as a set of flexible, standardized models for healthcare APIs that allow third-party developers to seamlessly connect to healthcare systems. It discusses the importance of building blocks for integration, promoting interoperability, and addressing the need for context-specific adaptations through profiling and extensions. The document also outlines various concepts related to the API economy and the challenges in achieving universal standardization in healthcare data exchange.