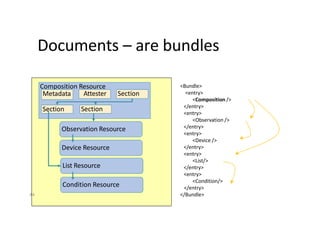
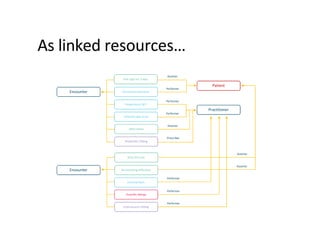
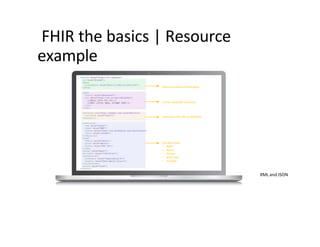
This document provides an introduction and overview of FHIR (Fast Healthcare Interoperability Resources), an interoperability standard developed by HL7. It discusses the benefits of FHIR for implementers, clinicians, consumers, and healthcare organizations. It also covers the basics of FHIR including resources, references between resources, structured and coded data, terminology, and profiling to adapt FHIR to specific needs.


![Coded datatypes
• Code: "status" : "confirmed"
• Coding: {
"system": "http://www.nlm.nih.gov/research/umls/rxnorm",
"code": "C3214954",
"display": "cashew nut allergenic extract Injectable"
}
• CodeableConcept: {
"coding": [{
"system": "http://snomed.info/sct",
"code": "39579001",
"display": "Anaphylactic reaction“
}],
"text" : "Anaphylaxis"
}](https://image.slidesharecdn.com/introtofhir-231009152927-cbda2b04/85/Intro_To_FHIR-pptx-31-320.jpg)