
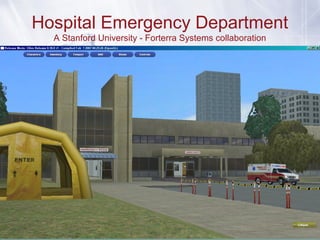

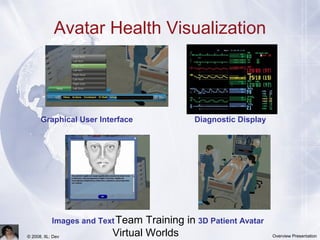
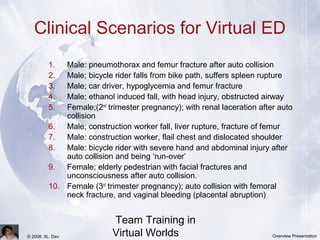
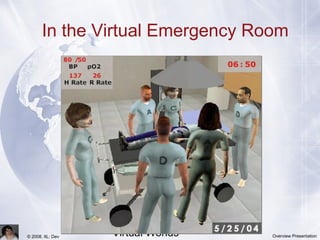

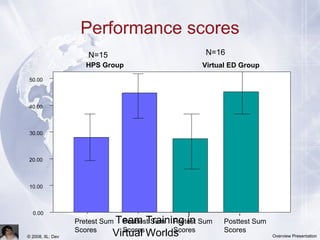


This document discusses the use of virtual worlds for team training, highlighting how immersive 3D environments facilitate interaction and learning through avatars. It outlines clinical scenarios in a virtual emergency room setting and emphasizes the effectiveness of multiplayer environments for teaching crisis resource management in trauma situations. The study suggests further exploration of various medical scenarios and the unique knowledge and skills that can be taught in virtual settings.































































