Viral infection in the central nervous system (CNS) is a common cause of seizures and epilepsy. Acute symptomatic seizures can occur in the context of almost all types of acute CNS viral infection. Secondary generalized seizures begin in one part of the brain, but then spread to both sides of the brain. In other words, the person first has a focal seizure, followed by a generalized seizure.
This file is designed by Mohammad saleh Moallem
Clinical ScenarioREASON FOR CONSULTATION Desaturation to 64.docxbartholomeocoombs
Clinical Scenario:
REASON FOR CONSULTATION:
Desaturation to 64% on room air 1 hours ago with associated shortness of breath.
HISTORY OF PRESENT ILLNESS:
Mrs. X is 73-year-old Caucasian female who was admitted to the general surgery service 3 days ago for a leaking j-tube which was surgically replaced 2 days ago and is now working properly. This morning at 07:30, the RN reported that the patient was sleeping and doing fine, then the CNA made rounds at 0900 and Mrs. X was found be mildly dyspneic. Vital signs were checked at that time and were; temperature 38.6, pulse 120, respirations 22, blood pressure 138/38. O2 sat was 64% on room air. The general surgeon was notified by the nursing staff of the hypoxia, an order for a chest x-ray and oxygen therapy were given to the RN. The O2 sat is maintaining at 91% on 4L NC. The patient was seen and examined at 10:10 a.m. She reports that she has been having mild dyspnea for 2 days that has progressively gotten worse. She does not use oxygen at home. Her respiratory rate at the time of visit was 22 and she feels short of breath. She has felt this way in the past when she had pneumonia. She is currently undergoing radiation treatment for laryngeal cancer and her last treatment was 1 to 2 weeks ago. She reports that she has 2 to 3 treatments left. She denies any chest pain at this time and denies any previous history of CHF. Review of her vital signs show that she has been having intermittent fevers since yesterday morning. Of note, she was admitted to the hospital 3 weeks ago for an atrial fibrillation with RVR for which she was cardioverted and has not had any further problems. The cardiologist at that time said that she did not need any anticoagulation unless she reverted back into A-fib.
REVIEW OF SYSTEMS:
Constitutional:
Negative for diaphoresis and chills.
Positive for fever and fatigue.
HEENT:
Negative for hearing loss, ear pain, nose bleeds, tinnitus.
Positive for throat pain secondary to her laryngeal cancer.
Eyes:
Negative for blurred vision, double vision, photophobia, discharge or redness.
Respiratory:
Positive for cough and shortness of breath
. Negative for hemoptysis and wheezing.
Cardiovascular:
Negative for chest pain, palpitations, orthopnea, leg swelling or PND.
Gastrointestinal:
Negative for heartburn, nausea, vomiting, abdominal pain, diarrhea, constipation, blood in stool or melena.
Genitourinary:
Negative for dysuria, urgency, frequency, hematuria and flank pain.
Musculoskeletal:
Negative for myalgias, back pain and falls.
Skin:
Negative for itching and rash.
Neurological:
Negative for dizziness, tingling, tremors, sensory changes, speech changes.
Endocrine/hematologic/allergies:
Negative for environmental allergies or polydipsia. Does not bruise or bleed easily.
Psychiatric:
Negative for depression, hallucinations and memory loss.
PAST MEDICAL HISTORY:
Diabetes mellitus that was diagnosed 12 years ago with neuropathy. This resolved after gastric.
Case Presentation of a patient presented with polyradiculoneuropathy and bilateral bulbar palsy. Detailed evaluation finally pinpoints to Guillian barre syndrome.
Chapter 19 Nursing Management of Pregnancy at Risk PregnancyMorganLudwig40
Chapter 19: Nursing Management of Pregnancy at Risk: Pregnancy-Related Complications
Case 1
Teresa is a 36-year-old primigravida who is expecting twins. She is 26 weeks pregnant. She stays after your “What to Expect with Twins” class to talk to you. Although Teresa is a nurse, she has many questions and concerns. Her twins are a result of years of trying to get pregnant and in vitro fertilization. She is nervous about whether she will have a vaginal delivery or a cesarean section. She is worried about having the babies prematurely. She wants you to tell her everything that could go wrong so she can be prepared
1. Why is Teresa’s pregnancy considered a high-risk pregnancy
Incorrect answer.
Teresa’s pregnancy is considered high risk pregnancy because most of IVF pregnancies require induced labor or caesarean section.
Also, most babies conceived through IVF are born prematurely or with a low birth weight. Incorrect.. there is a higher incidence of preterm birth due to multiple gestation, IVF itself does not increase the risk factor
IVF increases the risk of Down syndrome as well. Incorrect as IVF allows for early genetic testing.
2. Discuss potential pregnancy-related complications for Teresa.
What else?
Some of the potential pregnancy –related complications for Teresa are late miscarriage, She is 26 weeks pregnant.. this is no longer a complication.
ovarian hyper stimulation syndrome, She is 26 weeks pregnant.. this is no longer a complication.
This is for IVF not the pregnancy
high blood pressure, pre-eclampsia, premature delivery, low birth weight,
birth defects, Fetal not maternal
and stress.
3. Discuss the potential risks to the babies.
You only discuss problems of prematurity.. what else?
The babies are at a higher risk of being born with breathing problems because mostly twins who are conceived through in vitro fertilization are born prematurely and therefore it means that their respiratory system and organs like lungs are not fully developed. They are also at risk of jaundice or sepsis.
Case 2
Sarah is 19-year-old G1P0 at 36 weeks' gestation. Sarah has been followed weekly in the clinic for mild–moderate preeclampsia. At her clinic appointment today, Sarah’s blood pressure reading was 188/104. She is admitted to the antepartum unit for management of her worsening preeclampsia. You perform her admission assessment and note that her reflexes are brisk, her heart rate is 94, she complains of having an intense headache, and is seeing spots before her eyes. You perform an abdominal assessment and note that she has significant epigastric tenderness. (Learning Objective 5)
1. Develop a plan of care for the woman experiencing preeclampsia, eclampsia, and HELLP syndrome.
this is a definition not a care plan
The best way to treat Sarah for preeclampsia is to deliver the baby because at 36 weeks’ gestation, the baby is full grown and it will be safer to deliver the baby and avoid further complications. In some cases, this c ...
Drs. Olson’s and Jackson’s CMC Pediatric X-Ray Mastery: May CasesSean M. Fox
Drs. Olson and Jackson are interested in education and Pediatric Emergency Medicine. Follow along with the EMGuideWire.com team and Drs. Nikki Richardson, Mary Grady, and Michael Gibbs as they post these educational, self-guided radiology slides on Pediatric Emergency Medicine Radiology. This month’s topics include:
Subcutaneous air
Osteopenia
Bronchiolitis
Constipation
Asthma exacerbation
Alveolar Rhabdomyosarcoma
Aspirated Foreign Bodies
Small Bowel Obstruction
Kyphoscoliosis
Pneumatocele
Cecal Volvulus
Insulinoma refers to a tumor of the beta cells of the islets of Langerhans; although usually benign, it is one of the chief causes of hypoglycemia. An abnormal mass that grows in the beta cells of the pancreas that make insulin. They secrete insulin and are the most common cause of low blood sugar caused by having too much insulin in the body.
This file is designed by Mohammad saleh Moallem
Here in this presentation we basically review the anatomy of Basal ganglia and its functions and also the relation of pathologic pathway of Parkinson's disease to the affected basal ganglia.
I have answered the following questions in this presentation:
1. What is the role of basal ganglia?
2. What neurotransmitter is changing in Parkinson's disease?
3. Which brain structures would change in Parkinson's disease?
So this is the summary of the presented file:
Basal ganglia are a group of subcortical nuclear agglomerations involved in movement, and are located deep to the cerebral hemispheres.
Basal ganglia include the striatum (caudate nucleus and putamen), globus pallidus, substantia nigra, and subthalamic nucleus. The components intricately synapse onto each other to promote or antagonize movement.
FUNCTIONS of basal ganglia:
Significant role in controlling posture and voluntary movement through connections to the:
Thalamus
Cerebral cortex
Basal nuclei
Has connections to limbic system pathways, which govern the expression of various behaviors and motivational states. Plays a major role in making decisions. Plays a role in controlling eye movements.
Parkinson's disease is characterized by a deficiency of dopamine in the nigrostriatal system.
Dopamine is a type of neurotransmitter and hormone. It plays a role in many important body functions, including movement, memory and pleasurable reward and motivation.
Presented by: Mohammadsaleh Moallem
More Related Content
Similar to Viral meningitis and Secondary epilepsy
Clinical ScenarioREASON FOR CONSULTATION Desaturation to 64.docxbartholomeocoombs
Clinical Scenario:
REASON FOR CONSULTATION:
Desaturation to 64% on room air 1 hours ago with associated shortness of breath.
HISTORY OF PRESENT ILLNESS:
Mrs. X is 73-year-old Caucasian female who was admitted to the general surgery service 3 days ago for a leaking j-tube which was surgically replaced 2 days ago and is now working properly. This morning at 07:30, the RN reported that the patient was sleeping and doing fine, then the CNA made rounds at 0900 and Mrs. X was found be mildly dyspneic. Vital signs were checked at that time and were; temperature 38.6, pulse 120, respirations 22, blood pressure 138/38. O2 sat was 64% on room air. The general surgeon was notified by the nursing staff of the hypoxia, an order for a chest x-ray and oxygen therapy were given to the RN. The O2 sat is maintaining at 91% on 4L NC. The patient was seen and examined at 10:10 a.m. She reports that she has been having mild dyspnea for 2 days that has progressively gotten worse. She does not use oxygen at home. Her respiratory rate at the time of visit was 22 and she feels short of breath. She has felt this way in the past when she had pneumonia. She is currently undergoing radiation treatment for laryngeal cancer and her last treatment was 1 to 2 weeks ago. She reports that she has 2 to 3 treatments left. She denies any chest pain at this time and denies any previous history of CHF. Review of her vital signs show that she has been having intermittent fevers since yesterday morning. Of note, she was admitted to the hospital 3 weeks ago for an atrial fibrillation with RVR for which she was cardioverted and has not had any further problems. The cardiologist at that time said that she did not need any anticoagulation unless she reverted back into A-fib.
REVIEW OF SYSTEMS:
Constitutional:
Negative for diaphoresis and chills.
Positive for fever and fatigue.
HEENT:
Negative for hearing loss, ear pain, nose bleeds, tinnitus.
Positive for throat pain secondary to her laryngeal cancer.
Eyes:
Negative for blurred vision, double vision, photophobia, discharge or redness.
Respiratory:
Positive for cough and shortness of breath
. Negative for hemoptysis and wheezing.
Cardiovascular:
Negative for chest pain, palpitations, orthopnea, leg swelling or PND.
Gastrointestinal:
Negative for heartburn, nausea, vomiting, abdominal pain, diarrhea, constipation, blood in stool or melena.
Genitourinary:
Negative for dysuria, urgency, frequency, hematuria and flank pain.
Musculoskeletal:
Negative for myalgias, back pain and falls.
Skin:
Negative for itching and rash.
Neurological:
Negative for dizziness, tingling, tremors, sensory changes, speech changes.
Endocrine/hematologic/allergies:
Negative for environmental allergies or polydipsia. Does not bruise or bleed easily.
Psychiatric:
Negative for depression, hallucinations and memory loss.
PAST MEDICAL HISTORY:
Diabetes mellitus that was diagnosed 12 years ago with neuropathy. This resolved after gastric.
Case Presentation of a patient presented with polyradiculoneuropathy and bilateral bulbar palsy. Detailed evaluation finally pinpoints to Guillian barre syndrome.
Chapter 19 Nursing Management of Pregnancy at Risk PregnancyMorganLudwig40
Chapter 19: Nursing Management of Pregnancy at Risk: Pregnancy-Related Complications
Case 1
Teresa is a 36-year-old primigravida who is expecting twins. She is 26 weeks pregnant. She stays after your “What to Expect with Twins” class to talk to you. Although Teresa is a nurse, she has many questions and concerns. Her twins are a result of years of trying to get pregnant and in vitro fertilization. She is nervous about whether she will have a vaginal delivery or a cesarean section. She is worried about having the babies prematurely. She wants you to tell her everything that could go wrong so she can be prepared
1. Why is Teresa’s pregnancy considered a high-risk pregnancy
Incorrect answer.
Teresa’s pregnancy is considered high risk pregnancy because most of IVF pregnancies require induced labor or caesarean section.
Also, most babies conceived through IVF are born prematurely or with a low birth weight. Incorrect.. there is a higher incidence of preterm birth due to multiple gestation, IVF itself does not increase the risk factor
IVF increases the risk of Down syndrome as well. Incorrect as IVF allows for early genetic testing.
2. Discuss potential pregnancy-related complications for Teresa.
What else?
Some of the potential pregnancy –related complications for Teresa are late miscarriage, She is 26 weeks pregnant.. this is no longer a complication.
ovarian hyper stimulation syndrome, She is 26 weeks pregnant.. this is no longer a complication.
This is for IVF not the pregnancy
high blood pressure, pre-eclampsia, premature delivery, low birth weight,
birth defects, Fetal not maternal
and stress.
3. Discuss the potential risks to the babies.
You only discuss problems of prematurity.. what else?
The babies are at a higher risk of being born with breathing problems because mostly twins who are conceived through in vitro fertilization are born prematurely and therefore it means that their respiratory system and organs like lungs are not fully developed. They are also at risk of jaundice or sepsis.
Case 2
Sarah is 19-year-old G1P0 at 36 weeks' gestation. Sarah has been followed weekly in the clinic for mild–moderate preeclampsia. At her clinic appointment today, Sarah’s blood pressure reading was 188/104. She is admitted to the antepartum unit for management of her worsening preeclampsia. You perform her admission assessment and note that her reflexes are brisk, her heart rate is 94, she complains of having an intense headache, and is seeing spots before her eyes. You perform an abdominal assessment and note that she has significant epigastric tenderness. (Learning Objective 5)
1. Develop a plan of care for the woman experiencing preeclampsia, eclampsia, and HELLP syndrome.
this is a definition not a care plan
The best way to treat Sarah for preeclampsia is to deliver the baby because at 36 weeks’ gestation, the baby is full grown and it will be safer to deliver the baby and avoid further complications. In some cases, this c ...
Drs. Olson’s and Jackson’s CMC Pediatric X-Ray Mastery: May CasesSean M. Fox
Drs. Olson and Jackson are interested in education and Pediatric Emergency Medicine. Follow along with the EMGuideWire.com team and Drs. Nikki Richardson, Mary Grady, and Michael Gibbs as they post these educational, self-guided radiology slides on Pediatric Emergency Medicine Radiology. This month’s topics include:
Subcutaneous air
Osteopenia
Bronchiolitis
Constipation
Asthma exacerbation
Alveolar Rhabdomyosarcoma
Aspirated Foreign Bodies
Small Bowel Obstruction
Kyphoscoliosis
Pneumatocele
Cecal Volvulus
Insulinoma refers to a tumor of the beta cells of the islets of Langerhans; although usually benign, it is one of the chief causes of hypoglycemia. An abnormal mass that grows in the beta cells of the pancreas that make insulin. They secrete insulin and are the most common cause of low blood sugar caused by having too much insulin in the body.
This file is designed by Mohammad saleh Moallem
Here in this presentation we basically review the anatomy of Basal ganglia and its functions and also the relation of pathologic pathway of Parkinson's disease to the affected basal ganglia.
I have answered the following questions in this presentation:
1. What is the role of basal ganglia?
2. What neurotransmitter is changing in Parkinson's disease?
3. Which brain structures would change in Parkinson's disease?
So this is the summary of the presented file:
Basal ganglia are a group of subcortical nuclear agglomerations involved in movement, and are located deep to the cerebral hemispheres.
Basal ganglia include the striatum (caudate nucleus and putamen), globus pallidus, substantia nigra, and subthalamic nucleus. The components intricately synapse onto each other to promote or antagonize movement.
FUNCTIONS of basal ganglia:
Significant role in controlling posture and voluntary movement through connections to the:
Thalamus
Cerebral cortex
Basal nuclei
Has connections to limbic system pathways, which govern the expression of various behaviors and motivational states. Plays a major role in making decisions. Plays a role in controlling eye movements.
Parkinson's disease is characterized by a deficiency of dopamine in the nigrostriatal system.
Dopamine is a type of neurotransmitter and hormone. It plays a role in many important body functions, including movement, memory and pleasurable reward and motivation.
Presented by: Mohammadsaleh Moallem
The following file is about the most important procedures of neurological examination and has been taught in PBL class by MohammadSaleh Moallem.
A neurological examination is the assessment of sensory neuron and motor responses, especially reflexes, to determine whether the nervous system is impaired. This typically includes a physical examination and a review of the patient's medical history. In general, a neurological examination is focused on finding out whether there are lesions in the central and peripheral nervous systems or there is another diffuse process that is troubling the patient.
The results of the examination are taken together to anatomically identify the lesion. Finally, it is the role of the physician to find the cause for why such a problem has occurred.
Presented by: Mohammadsaleh Moallem
Difference between benign and malignant tumors:
Benign tumors:
Benign tumors are those that stay in their primary location without invading other sites of the body.
Benign tumors tend to grow slowly and have distinct borders. A growth that is not cancer.
Malignant tumors:
Are cells that grow uncontrollably and spread locally and/or to distant sites, they are cancerous.
They spread to distant sites via the bloodstream or the
lymphatic system. This spread is called metastasis.
Neostigmine:
Neostigmine is a cholinesterase inhibitor used in the treatment of myasthenia gravis.
Neostigmine does not cross the blood-brain barrier. Neostigmine is used as an antidote for anticholinergic intoxication.
Mechanism of action:
Inhibits the hydrolysis of acetylcholine by competing with acetylcholine for attachment to acetylcholinesterase at sites of cholinergic transmission. It enhances cholinergic action by facilitating the transmission of impulses across neuromuscular junctions.
Presented by: Mohammadsaleh Moallem
Laparoscopic surgery is a surgical technique in which short, narrow
tubes (trochars) are inserted into the abdomen through small (less
than one centimeter) incisions. Through these trochars, long, narrow instruments are inserted. The surgeon uses these instruments to manipulate, cut, and sew tissue.
The advantages include reduced pain due to smaller incisions, reduced hemorrhaging, and shorter recovery time.
The key element is the use of a laparoscope, a long fiber optic cable system that allows viewing of the affected area by snaking the cable from a more distant, but more easily accessible location.
Right Adrenalectomy:
Since its first description in 1992, laparoscopic adrenalectomy has become the gold standard for the surgical treatment of most adrenal conditions. The benefits of a minimally invasive approach to adrenal resection such as decreased hospital stay, shorter recovery time and improved patient satisfaction are widely accepted. However, as this procedure becomes more widespread, critical steps of the operation must be maintained to ensure expected outcomes and success. This presentation reviews the surgical techniques for the laparoscopic adrenalectomy.
Presented by: Mohammadsaleh Moallem
Nephrotic syndrome is a disorder of the glomerular filtration barrier, and central to the filtration mechanism of the glomerular filtration barrier is the podocyte.
So it’s a kidney disorder that causes your body to pass too much protein in your urine. It’s usually caused by damage to the clusters of small blood vessels in your kidneys that filter waste and excess water from your blood.
Nephrotic syndrome:
Characterized by heavy proteinuria, hypoalbuminemia, edema, hyperlipidemia, it's 90% idiopathic and Relapses are common.
The treatment of nephrotic syndrome can be symptomatic or can directly address the injuries caused to the kidney.
1. Symptomatic treatment
2. Kidney damage treatment
Symptomatic treatment is a therapy that eases the symptoms without addressing the basic cause of the disease, while kidney damage treatment can directly address the injuries caused to the kidney.
Presented by: Mohammadsaleh Moallem
This lecture is about what is the neostigmine and what are its medical uses, mechanism of action and side effects.
Neostigmine is a cholinesterase inhibitor used in the symptomatic treatment of myasthenia gravis by improving muscle tone.
Neostigmine is in the cholinergic family of medications. It works by blocking the action of acetylcholinesterase and therefore increases the levels of acetylcholine.
Neostigmine: Cholinesterase inhibitor = ↑ ACh
Neostigmine is an anticholinesterase inhibitor and inhibits the hydrolysis of acetylcholine by competing with acetylcholine for binding to acetylcholinesterase at the site of cholinergic transmission. By reducing the hydrolysis of acetylcholine, the transmission of nerve impulses is facilitated.
At the end of surgery, neostigmine has been given for the reversal of neuromuscular blocking agents with several adverse effects such as bradycardia and profuse secretion.
Atropine has been used to prevent those side effects of neostigmine.
Side effects titles as review:
.
Nausea, headache, insomnia, dry mouth, dizziness, vomiting, allergic reactions, skin rash, hot flashes, joint pain, stroke, weakness, muscle cramps, frequent urination
Neostigmine is rapidly absorbed after intramuscular injection (IM). Neostigmine binding to human serum albumin is approximately 15 to 25%.
Neostigmine is metabolized in the liver by microsomal enzymes. The apparent excretory half-life of neostigmine is between 24 and 113 minutes.
Presented by: Mohammadsaleh Moallem
Farmer’s lung disease:
Farmer's lung disease (FLD) is a form of hypersensitivity pneumonitis (HP) caused by inhaling microorganisms from hay or grain stored in conditions of high humidity in the agricultural workplace.
Hypersensitivity pneumonitis, also known as extrinsic allergic alveolitis, is an immunologically mediated inflammatory disease of the lung involving the terminal airways.
It's also called extrinsic allergic alveolitis, hypersensitivity alveolitis, or hypersensitivity pneumonitis.
The "-itis" at the end of these names means it causes inflammation. With farmer's lung, the inflammation, or swelling, is in the lungs.
Two conditions cause COPD: chronic bronchitis and emphysema. Both affect your lungs in different ways.
Asthma is not typically considered a type of COPD, but it is a chronic respiratory condition. You can have asthma along with COPD.
Presented by: Mohammadsaleh Moallem
Here in this lecture we will discuss two main points:
1. Analyzing the MRI images and their relationship to Encephalitis.
2. Explaining that how neurosurgical operation can assist in treatment of intractable epilepsy.
Pathology of Encephalitis:
In acute encephalitis, inflammation and edema occur in infected areas throughout the cerebral hemispheres, brain stem, cerebellum, and, occasionally, spinal cord.
Petechial hemorrhages may be present in severe infections. Direct
viral invasion of the brain usually damages neurons, sometimes
producing microscopically visible inclusion bodies.
MRI analysis: The right occipital leaf-shaped slightly longer T2 signal shadow, consider infarction. Right occipital lobe-shaped FS like high signal, consider infarction or brain contusion.
Intractable epilepsy:
Intractable epilepsy is when seizures can't be controlled by medicines. Intractable epilepsy is diagnosed when someone has had years of uncontrolled seizures.
Many people whose seizures do not respond to medication will
respond to surgical treatment, relieving seizures completely or almost completely in one-half to two-thirds of patients who qualify for surgery.
Epilepsy surgery is usually performed during general anesthesia, and you'll be unconscious during the procedure. In rare circumstances, your surgeon may awaken you during part of the operation to help the team determine which parts of your brain control language and movement. In such cases, you would receive medication to control pain.
The surgeon creates a relatively small window in the skull, depending on the type of surgeryAfter surgery the window of bone is replaced and fastened to the remaining skull for healing.
Presented by: Mohammadsaleh Moallem
Mushroom poisoning is poisoning resulting from the ingestion of mushrooms that contain toxic substances. Its symptoms can vary from slight gastrointestinal discomfort to death in about 10 days. Mushroom toxins are secondary metabolites produced by the fungus.
Amanita virulent fungus; Fungal pathogens possess virulence factors that allow them to cause disease in humans and animals.
All toxic mushrooms cause vomiting and abdominal pain; other manifestations vary significantly by mushroom type. Generally, mushrooms that cause symptoms early (within 2 hours) are less dangerous than those that cause symptoms later (usually after 6 hours).
The treatment of patients poisoned with amanita muscaria poisoning should be conducted in hospital.
Gastric lavage and symptomatic treatment should be carried out as soon as possible. If necessary, restraint or sedation should be employed for agitated and/or delirious patients.
Patients hospitalized and given aggressive support therapy almost immediately after ingestion of amanitin-containing mushrooms have a mortality rate of only 10%, whereas those admitted 60 or more hours after ingestion have a 50–90% mortality rate.
Presented by: Mohammadsaleh Moallem
This is a schema chart about a patient named Mr. Zhang, a middle-aged farmer with Systemic atherosclerosis, whose diagnosis and treatment in a hospital by a specialist doctor are fully illustrated in this schema-chart and diagram. The main treatment for this patient was implantation of a stent in his right coronary artery.
The initial diagnosis was hypertensive crisis, but after tests, the doctor realized that the more accurate diagnosis was Systemic atherosclerosis.
This schema-chart is designed by Mohammadsaleh Moallem
The facial nerve is one of a group of nerves called the cranial nerves (CN), 12 pairs of nerves that, with the exception of the spinal accessory nerve (CN XI), originate in the brain and contribute to the peripheral nervous system (PNS).
facial nerve contains many different types of fibers, including general sensory (afferent) fibers, special sensory fibers, visceral/autonomic motor (efferent) fibers, and somatic motor fibers.
So these are also the functions of facial nerve:
Somatic sensory
Special sensory
Branchial motor
Parasympathetic motor
To remember the branches of the facial nerve, you can use the following mnemonic: "To Zambia By Motor Car", standing for:
Temporal
Zygomatic
Buccal
Marginal mandibular
Cervical branches.
Presented by: Mohammadsaleh Moallem
Hemodialysis is a treatment to filter wastes and water from your blood; In hemodialysis, the blood is cleaned outside the body using a dialysis machine and then sent back into the body.
Hemodialysis is a treatment to filter wastes and water from your blood, as your kidneys did when they were healthy. Hemodialysis helps control blood pressure and balance important minerals, such as potassium, sodium, and calcium, in your blood.
Hemodialysis is one way to treat advanced kidney failure and can help you carry on an active life despite failing kidneys.
Mechanism of Hemodialysis:
Hemodialysis is a procedure by which waste products and excess water are removed from a patient’s blood. This is done by directly removing blood from the patient’s circulation, passing it through the dialysis filter, and then returning it directly back into the circulation.
Apparatus needed:
Dialyzer or dialysis filter
Dialysate (dialysis solution)
Tubing for transport of blood and dialysate
Machine that powers and monitors the filtration
Hemodialysis has 5 main steps which are as follows:
1.Two sets of tubing are connected to the patient’s dialysis access:
Connected directly to central venous catheter
Two needles inserted into AVF/AVG and taped down
2. Azotemic blood pumped from patient into dialysis filter
3. Dialysis filter removes toxins primarily through diffusion:
Dialysis filter is a plastic cylinder filled with thousands of tiny individual tubes composed of the filtering material.
Blood flows through the inside of the tiny tubes in one direction.
Dialysis fluid (dialysate) flows on the outside of the tiny tubes (but still within the single plastic cylinder that contains them) in the opposite direction.
The opposing directions of blood and dialysate result in maximal concentration gradients that drive the diffusion of toxins:
Known as “countercurrent” mechanism
Also results in correction of electrolyte/acid–base abnormalities via diffusion.
4. Dialysis filter removes excess water from the blood through ultrafiltration.
Suction force is applied by the dialysis machine across the dialysis filter.
Water is pulled from the blood side into the dialysate side.
5. Clean blood and waste-filled dialysate exit the dialysis filter.
Clean blood is pumped back into the patient’s Circulation.
Waste-filled dialysate is disposed of (including the excess water from the patient’s body that was removed during ultrafiltration).
Chronic dialysis
3–4 hours each session
3 times a week (Monday/Wednesday/Friday or Tuesday/Thursday/Saturday)
Acute dialysis:
Treatment duration and daily schedule are
Variable.
Priscriptions: The nephrologist may control many variables within the dialysis procedure:
Duration of treatment
Ultrafiltration goal
Anticoagulation
Electrolyte composition of the dialysate
Speed of blood flow and dialysate flow
Presented by: Mohammadsaleh Moallem
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Acute scrotum is a general term referring to an emergency condition affecting the contents or the wall of the scrotum.
There are a number of conditions that present acutely, predominantly with pain and/or swelling
A careful and detailed history and examination, and in some cases, investigations allow differentiation between these diagnoses. A prompt diagnosis is essential as the patient may require urgent surgical intervention
Testicular torsion refers to twisting of the spermatic cord, causing ischaemia of the testicle.
Testicular torsion results from inadequate fixation of the testis to the tunica vaginalis producing ischemia from reduced arterial inflow and venous outflow obstruction.
The prevalence of testicular torsion in adult patients hospitalized with acute scrotal pain is approximately 25 to 50 percent
Knee anatomy and clinical tests 2024.pdfvimalpl1234
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...
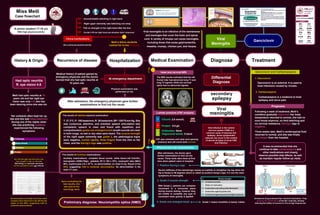
Viral meningitis and Secondary epilepsy
1. Clinical manifestations
Miss Meili
A senior student 17-18 y/o
Case flowchart
With high physical activity
History & Origin Recurrence of disease Hospitalization Medical Examination Diagnose Treatment
Had optic neuritis
R. eye vision 4.6
Meili had optic neuritis at 15
years old and her right eye
vision was only 4.6. she has
been dancing since she was six.
Chilliness
Sore throat
Malaise
Myalgia
Her schedule often kept her up
late and she was sleep-deprived.
During one of the nights when
she was practicing suddenly
experienced the following
symptoms:
She continued physical activity
Uncontrollable twitching in right hand
Right upper extremity was twitching non-stop
Couldn’t lift her right hand and situation didn’t improved
Felt no strength in her right hand after the tics
At emergency department
The results of detailed physical examination:
T: 37.3°C, P: 100 beats/min,R: 26 beats/min,BP: 120/75 mm Hg. She
was conscious, attentive, and oriented; speech articulation was
competent; speech is clear and fluent with repetition, and
comprehension;grade one enlarged tonsil;breath sounds are clear
in both lungs; no wet or dry rales were heard. The muscle strength
of the right upper extremity was grade 2, the pathological signs
were negative, nuchal rigidity, three fingers from the chin to the
chest, and the Kernig's sign was positive.
After admission, the emergency physician gave further
examinations to find out the cause.
Preliminary diagnose: Neuromyelitis optica (NMO)
Head and cervical MRI
Chlorid: 2.6 mmol/L
Protein: 0.6 g/L
CSF was colorless and clear and opening
pressure and cell count were normal.
Physical and Lab. Examinations
After admission, the doctor gave
further examination to find out the
cause. These tests were done at first
time when patient came to hospital.
Differential
Diagnose
secondary
Viral
Meningitis
Ganciclovir
Viral meningitis is an infection of the membranes
and meninges that cover the brain and spinal
cord. A variety of viruses can cause meningitis,
including those that cause gastroenteritis,
measles, mumps, chicken pox, and herpes.
Ganciclovir and Carbamazepine
1. Ganciclovir
Following a week of treatment, Meili’s
condition gradually improved. Her body
temperature returned to normal, she had no
sore throat anymore, no limb twitching and
no cervical resistance. Kernig’s sign is
negative.
PBL2-2
Flowchart
4
June, 2022
Teacher
Prof. Cui Shuang 崔爽老师
Students
默汉 哈沙
莎格 索菲雅
阿朵 娜迪
约书亚 露华
艾里克
Saleh Harsha
Razy
Shaghayegh Saffiyah
Aliakbar
Nadia
Niloufar
JJ
李明
Abubakar
Medical history of patient gained by
emergency physician and the doctor
learned that she had optic neuritis at
15 years old.
Physical examination was
performed on her
HI
G
Lo
w
Viral infection in the central
nervous system (CNS) is a
common cause of seizures and
epilepsy. Acute symptomatic
seizures can occur in the context
of almost all types of acute CNS
viral infection.
It was recommended that she
continue to take carbamazepine and
other medications and closely
observe possible side effects, as well
as maintain regular follow-up visits.
Antiseizure drug-enhanced Na+ channel inactivation. They
prolong the inactivation of the Na+ channels, thereby
reducing the ability of neurons to fire at high frequencies.
Meili’s fellow students
rushed her to the hospital.
Her first thought was that she must
have caught a cold, so she took
BaiFuNing and antiviral oral liquid
but the symptoms were not relieved.
Auxiliary examinations: complete blood counts: white blood cell 9.0x10/L,
hemoglobin (HGB)130g/L, platelets (PLT) 180 x 109
/L, neutrophil ratio (NEU)
60%, erythrocytes 4.6 x 1012
/L, no abnormalities on chest X-ray. Result of the
EEG, suggesting mild to moderate abnormalities. No abnormalities in the
head CT scan.
The results of Auxiliary examinations:
Upon evaluating her
test results, she
was sent to the
neurology ward.
Several spikes and spike and slow-wave
complex were observed in the left frontal
region of the EEG, suggesting mild to
moderate abnormalities.
The MRI results indicated that the left
frontal lobe had abnormal long T1 and
long T2 signals, while the cervical
spine had no abnormal signals.
Lumbar puncture (CSF analysis)
Nor
Antibodies: None
Oligoclonal bands: 0 band
1. Positive Kernig’s sign
Severe stiffness of the hamstrings causes an inability to straighten the leg when the
hip is flexed to 90 degrees which is called as positive kenig’s sign; it’s one the main
symptoms of meningitis.
2. Grade 2 muscle strength
With Grade 2, patients can complete
movement in a horizontal plane
during muscle testing, however they
are unable to complete any type of
movement when gravity is applied.
3. Grade one enlarged tonsil Grade 1 means tonsillitis is barely visible.
epilepsy
Viral
meningitis
2. Carbamazepine
Ganciclovir is an antiviral. It is used to
treat infections caused by viruses.
Carbamazepine is a medicine to treat
epilepsy and nerve pain.
Prognosis
Three weeks later, Meili’s cerebrospinal fluid
returned to normal, and she was finally
discharged from the hospital.
1
st
day
2
nd
day