Vibration disease (VD)
Vibrationdisease (pneumatic hammer disease) is an
occupational disease characterized by a chronic course with a
lesion of the peripheral nervous, vascular and the
musculoskeletal system when the employee exposed to
occupational vibration above the maximum permissible level
(MPL; exposure limit).
The disease is characterized by a long benign course with a
gradual increase in clinical syndromes with continued contact
with vibration.
Early signs of vibration exposure (ESVE) are the presence of
deviations in the health of a worker based on the results of an
instrumental examination in the absence of clinical signs of
illness with prolonged exposure to industrial vibration above
the MPL.
•This nosological form is one of the leading ones in
professional pathology. In the structure of occupational
diseases it ranks second.
4.
Vibration- these aremechanical vibrations of solid
bodies.
Classification of vibration:
• Very low frequency vibration - below 2 Hz;
• Low frequency vibration - between 2 and 20 Hz;
• Medium frequency vibration - between 20 and 300 Hz;
• High frequency vibration - between 300 and 1000 Hz,
sometimes even up to 5000 Hz and Shaking.
The most significant damaging effect on the human body is
vibration in the frequency range of 35 – 250 Hz.
5.
Who gets vibrationdisease?
•Heavy engineering workers,
•Workers in the metallurgical
industry,
6.
Who gets vibrationdisease?
•Workers in the
construction, aviation and
shipbuilding industries
7.
Who gets vibrationdisease?
•Workers in the coal and
mining industry,
•Transport and agricultural
workers.
8.
Who gets vibrationdisease?
•Those whose activities are directly
related to mechanized tools,
equipment and machines that serve
as sources of vibration.
9.
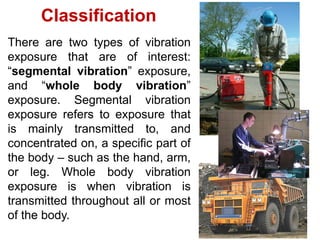
There are twotypes of vibration
exposure that are of interest:
“segmental vibration” exposure,
and “whole body vibration”
exposure. Segmental vibration
exposure refers to exposure that
is mainly transmitted to, and
concentrated on, a specific part of
the body – such as the hand, arm,
or leg. Whole body vibration
exposure is when vibration is
transmitted throughout all or most
of the body.
Classification
10.
Etiology
Whole-body vibration
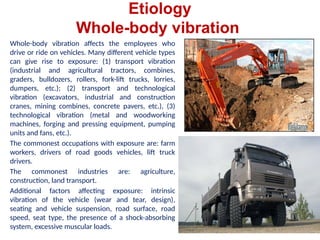
Whole-body vibrationaffects the employees who
drive or ride on vehicles. Many different vehicle types
can give rise to exposure: (1) transport vibration
(industrial and agricultural tractors, combines,
graders, bulldozers, rollers, fork-lift trucks, lorries,
dumpers, etc.); (2) transport and technological
vibration (excavators, industrial and construction
cranes, mining combines, concrete pavers, etc.), (3)
technological vibration (metal and woodworking
machines, forging and pressing equipment, pumping
units and fans, etc.).
The commonest occupations with exposure are: farm
workers, drivers of road goods vehicles, lift truck
drivers.
The commonest industries are: agriculture,
construction, land transport.
Additional factors affecting exposure: intrinsic
vibration of the vehicle (wear and tear, design),
seating and vehicle suspension, road surface, road
speed, seat type, the presence of a shock-absorbing
system, excessive muscular loads.
11.
Etiology
Whole-body vibration
Prevention andcontrol
Drivers should:
• Adjust their seating
• Avoid rough, poor or uneven surfaces
• Adjust the vehicle speed to suit road
conditions.
It also advises on several other measures,
including:
• Maintenance of vehicle suspension
• Maintenance of site roadways
• Better choice of seating
• Rest breaks
• Safer systems of work
• Simple health monitoring.
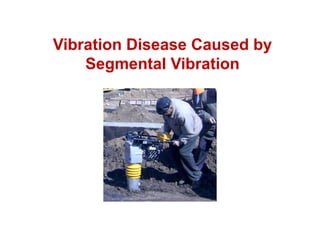
12.
Etiology
Segmental vibration
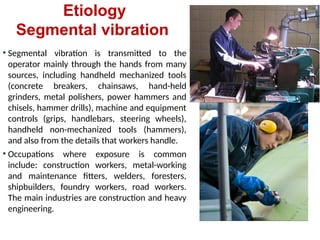
• Segmentalvibration is transmitted to the
operator mainly through the hands from many
sources, including handheld mechanized tools
(concrete breakers, chainsaws, hand-held
grinders, metal polishers, power hammers and
chisels, hammer drills), machine and equipment
controls (grips, handlebars, steering wheels),
handheld non-mechanized tools (hammers),
and also from the details that workers handle.
• Occupations where exposure is common
include: construction workers, metal-working
and maintenance fitters, welders, foresters,
shipbuilders, foundry workers, road workers.
The main industries are construction and heavy
engineering.
13.
Main factors affectingexposure
• Tools: intrinsic properties of the tool (e.g. size, weight, characteristics (acceleration,
duration, direction, frequency, level, type of vibration), balance between reciprocating
forces), age of tools, and their maintenance.
• Material being worked
• Type of action at the work interface (e.g. cutting, drilling, grinding)
• Operator technique (e.g. type and force of grip, orientation of the hand-arm, working
posture).
• Other associated occupational hazards (cooling microclimate, airflow and wetting of
the operator’s hands, noise and harmful chemicals)
• Nonoccupational exposure to vibration and cold on employees
Etiology
Segmental vibration
14.
Prevention and control
Anumber of steps can mitigate the risk in exposed populations. These may be
broadly summarized as:
• Avoidance (e.g. doing the job another way)
• Substitution (of tool or material worked)
• Interruption of the pathway (by isolation or vibration-damping)
• Safer systems of work. Some options include:
• Routine replacement of worn out tool parts
• Proper selection of tools for the task
• The redesign of tools to avoid the need to grip high vibration parts, or to
reduce grip force
• Rest breaks to limit exposure times.
Another common approach involves screening for early health effects and limiting
further exposure in those with hand-arm vibration syndrome.
Etiology
Segmental vibration
The human bodyis subject to general vibration at an oscillation frequency
higher than 2 Hz. The degree of oscillation propagation throughout the body depends
on their frequency, amplitude, the area of body sections in contact with the vibration
object, application location, and direction of the vibration, damping properties of
tissues, resonance phenomena, etc. For a person standing on a vibrating floor, there
are two resonant peaks at 5-12Hz and 17-25Hz, for a sitting one - at frequencies 4-
6Hz, for a lying one - at 3-3.5Hz. The physiological effects of human exposure to
vibration are determined by the deformation or displacement of organs and tissues,
which disrupts their normal functioning and leads to irritation of mechanoreceptors
that perceive vibration. Moreover, low-frequency vibration can cause the effect of
motion sickness due to irritation of the otolith apparatus and the nerve endings of the
semicircular ducts. But the main effects of vibration on the musculoskeletal system
due to fatigue of the muscles and micro traumatization of intervertebral discs and
bone tissue. The general fatigue also takes place at the person working with the
general vibration. Due to the difficulty of venous outflow and neuro-reflex disorders,
the development of peripheral angiodystonic syndrome is possible.
Pathogenesis
17.
Clinical picture
At present,the leading syndromes in the clinical picture of
VD caused be whole-body vibration are non-specific low-back
pain (LBP), sciatica (radiculopathy), lumbar disc degeneration,
peripheral neuropathy of the extremities, central and peripheral
angiodystonic syndrome.
Among the syndromes of the stage I of the disease,
polyneuropathy syndrome occurs most frequently. It is
characterized by gnawing pain in the extremities, which often
localized in the joints, numbness and paresthesias, mainly in
the hands. Over time, the pain syndrome increases, disturbing
the sleep of patients. Hypalgesia of a polyneuritis type, a
decrease in vibration sensitivity, takes place. Along with
sensory impairments, such signs as marbling, hyperhidrosis,
and, less frequently, hypothermia of the feet and hands may
develop.
18.
Clinical picture
As theVD caused by whole-body vibration progresses (stage II),
musculoskeletal disorders begins to predominate. Now the low-back
pain which limited motions, the tension in the paravertebral muscles,
and their soreness on palpation add to the pain in the lower extremities.
In the future, sciatica may join, which has the following symptoms:
signs of compression of the root of a spinal nerve which increases pain,
numbness, and paresthesias; weakening (loss) of tendon reflexes in the
affected area; positive symptoms like straight leg raise, Neri's sign;
distal hypalgesia is supplemented with a radicular type of hypalgesia;
motor impairment is possible up to paresis.
The impact of general vibration causes cerebral vascular disorders,
complementing the clinical picture of the disease with unstable
headaches without clear localization, bouts of non-systemic vertigo,
increased fatigue, cachexia.
Motion sickness includes four forms: nervous, gastrointestinal,
cardiovascular, and mixed.
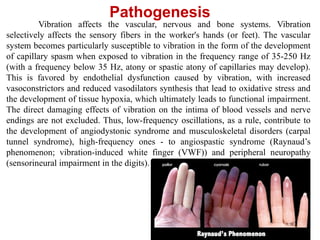
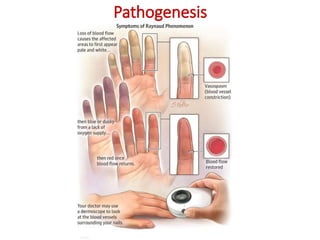
Vibration affects thevascular, nervous and bone systems. Vibration
selectively affects the sensory fibers in the worker's hands (or feet). The vascular
system becomes particularly susceptible to vibration in the form of the development
of capillary spasm when exposed to vibration in the frequency range of 35-250 Hz
(with a frequency below 35 Hz, atony or spastic atony of capillaries may develop).
This is favored by endothelial dysfunction caused by vibration, with increased
vasoconstrictors and reduced vasodilators synthesis that lead to oxidative stress and
the development of tissue hypoxia, which ultimately leads to functional impairment.
The direct damaging effects of vibration on the intima of blood vessels and nerve
endings are not excluded. Thus, low-frequency oscillations, as a rule, contribute to
the development of angiodystonic syndrome and musculoskeletal disorders (carpal
tunnel syndrome), high-frequency ones - to angiospastic syndrome (Raynaud’s
phenomenon; vibration-induced white finger (VWF)) and peripheral neuropathy
(sensorineural impairment in the digits).
Pathogenesis
Clinical picture
Hand–arm vibrationsyndrome
The term ‘hand–arm vibration syndrome’ has been used to
collectively define the disorders thought to be associated with exposure
to hand-transmitted vibration.
Clinical features of HAVS involve two main disorders: (1)
vibration-induced sensorineural disease (peripheral neuropathy and
carpal tunnel syndrome) and (2) peripheral angiodystonic/angiospastic
syndrome (vibration white finger).
Peripheral angiodystonic syndrome of the upper extremities is
characterized by numbness and mild pain in the hands at rest and
increased sensitivity to cold of the fingers. There are no sensation
disorders. On examination, moderate hypothermia of the fingers (26–
25 ºС) and thermal asymmetry (more than 1 ºС), marbling of the
hands, and hyperhidrosis of the palms are noted. The cold challenge
test reveals a slowdown in time (up to 30 minutes) to restore the
temperature of the skin of the fingers to the original values (20-25
minutes).
23.
Clinical picture
Hand–arm vibrationsyndrome
Peripheral angiospastic syndrome of the upper extremities (or
VWF) is characterized by episodic attacks of painless finger blanching
(mainly the “working” hand) and is exacerbated by exposure to
vibration and cold (often in winter), spontaneously resolving after a
few minutes. It is associated (during the attack) with
numbness/coldness and (in recovery) with paresthesias and a reactive
hyperemia. The number of attacks correlates with the severity and
duration of the disease.
The syndrome of distal autonomic-sensory polyneuropathy of the
upper extremities, being the main manifestation of the disease at the
initial (I) stage, is characterized by recurrent hand pain, numbness in
the hands appearing in a state of rest, pain and vibration sensitivity
disorders in the form of “short gloves” combined with vegetative-
vascular disorders (marbling, fall in temperature, hyperhidrosis of the
palms), and a decrease in muscle endurance to static effort.
24.
Clinical picture
Hand–arm vibrationsyndrome
The syndrome of distal autonomic-sensory
polyneuropathy of the upper extremities, being the
main manifestation of the disease at the initial (I)
stage, is characterized by recurrent hand pain,
numbness in the hands appearing in a state of rest,
pain and vibration sensitivity disorders in the form of
“short gloves” combined with vegetative-vascular
disorders (marbling, fall in temperature, hyperhidrosis
of the palms), and a decrease in muscle endurance to
static effort.
25.
Clinical picture
Hand–arm vibrationsyndrome
If the effect of vibration continues for several more years, the
vibration disease passes into stage II – moderately-marked
disorders, characterized by an increase in the intensity of
manifestations of the initial stage, that limits the ability of patients
to work. Workers also may have a decrease in touch sensitivity, fine
finger dexterity, and grip strength. They may complain that "the
hand does not hold the tool," "everything falls out of the hands."
Objectively: cyanosis and marbling of the hands and lower third of
the forearm, hypothermia of the hands (up to 22-24 ºС),
hyperhidrosis of the palms, swelling of the fingers, and, as a result,
stiffness in the joints of the hands. The frequency and duration of
attacks, which can occur without a provoking factor (cold factor),
can last up to 30-45 minutes and drastically limit the work activity.
Pain syndrome becomes persistent and permanent. Sensory
impairment reaches the level of the elbow joint.
26.
Clinical picture
Hand–arm vibrationsyndrome
At this stage, especially for workers with great work
experience and additional hazards like physical exertion on the
hands and upper limb girdle, disorders of the musculoskeletal
system of the upper limbs in the form of myelofibrosis can
develop. Myelofibrosis is characterized by pain in muscles of
the hands and forearms, increased fatigue of the hands during
work, tonic convulsions in the small muscles of the hands.
Palpation reveals indurations and soreness of the muscles of
the forearm. Dynamometry diagnoses a decrease in absolute
muscle strength.
Osteoarthritis of the wrist or elbow, specific
musculoskeletal disorders of the upper limb and Dupuytren’s
contracture may also be commoner in workers exposed to
hand-transmitted vibration.
27.
Clinical picture
Hand–arm vibrationsyndrome
The most severe cases that involve skin trophic
changes and gangrene (III stage) are rarely seen.
Their presence requires more extensive investigation
for a major comorbidity, such as a collagen vascular
disease or obstructive arterial disease.
28.
Clinical assessment anddiagnosis
of HAVS
The examination should include:
1) Occupational (exposure) history assessment (at least 10-15 years
of work in contact with vibration).
2) The sanitary and hygienic characteristic of the working conditions
(character, levels, exposure time, a spectrum of the vibration, presence
of other hazards) with exposure levels exceeding their maximum
permissible levels.
3) Data of the pre-placement and surveillance examinations, the
patient card (health status before starting the work; the dynamics of the
disease). The emergence of health problems after a few years of work
with vibration, slow progression of the disease, the lack of a history of
diseases of the nervous, cardiovascular, musculoskeletal system, and
other illnesses that can manifest this symptoms, the absence of
harmful habits (drug addiction, substance abuse, alcoholism) will testify
in favor of VD. One more "pros" can be called resolution of the
symptoms of the disease after a change of profession.
29.
Clinical assessment anddiagnosis
of HAVS
4) Special tests
Assessment of the state of peripheral circulation:
- skin thermometry (lowering the temperature of the hands/feet below
27 ºС);
- thermal camera (decrease in skin temperature with asymmetry on
the fingers below 27 ºС, up to the symptom of “finger amputation” during
an attack, dorsum of the hand and forearms below 29.6 ºС);
- cold provocation test (CPT) (attack of whitening of the
fingers/slowing down of the temperature recovery of the skin on the hands
for more than 25 minutes or increase in systolic blood pressure of
fingers);
- arteriography (narrowing of arterioles, arteries);
- rheovasography (decrease in the intensity of pulse blood filling in
combination with an increase in the tone of the arterioles and arteries of
the upper extremities);
- Doppler ultrasound of peripheral vessels (decrease in the diameter
of arterioles and arteries, decrease in the systolic and volumetric blood
30.
Clinical assessment anddiagnosis
of HAVS
Assessment of the sensorimotor system
- algesimetry (increase in pain thresholds);
- pallestesiometry, as nerve conduction study (an
increase of vibration sensitivity thresholds);
- Electroneuromyography (slowing down the nerve
conduction velocity through the sensory fibers of the
somatic nerves of the upper limb (below 50 m/s; with
normal rates of excitation through the motor fibers of these
nerves; reducing bioelectric activity (less than 400 mV) and
reducing biopotentials (less than 50 Hz) at maximum
arbitrary contractions of the forearm muscles).
31.
Clinical assessment anddiagnosis
of HAVS
Assessment of the state of the locomotory apparatus
- X-ray (osteoarthritis of the wrist (less often - elbow)
joints);
- ultrasound of the joints (joint effusion, narrowing of the
joint space);
- densitometry (osteoporosis of the distal phalanges of
the fingers while maintaining the mineral density of other
parts of the skeleton).
32.
Clinical assessment anddiagnosis
of HAVS
!!! Vascular and sensory effects are normally graded
separately, according to two three-point scales proposed in
1986 by an expert Stockholm Workshop (see Tables 01
and 02). Some assessors now combine these clinical
features with the output from objective tests.
33.
Clinical assessment anddiagnosis
of HAVS
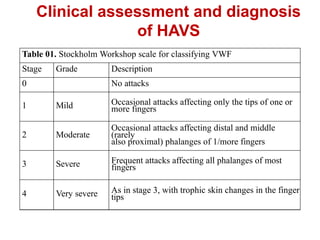
Table 01. Stockholm Workshop scale for classifying VWF
Stage Grade Description
0 No attacks
1 Mild Occasional attacks affecting only the tips of one or
more fingers
2 Moderate
Occasional attacks affecting distal and middle
(rarely
also proximal) phalanges of 1/more fingers
3 Severe Frequent attacks affecting all phalanges of most
fingers
4 Very severe As in stage 3, with trophic skin changes in the finger
tips
34.
Clinical assessment anddiagnosis
of HAVS
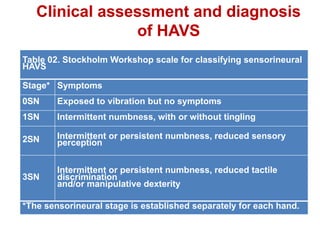
Table 02. Stockholm Workshop scale for classifying sensorineural
HAVS
Stage* Symptoms
0SN Exposed to vibration but no symptoms
1SN Intermittent numbness, with or without tingling
2SN Intermittent or persistent numbness, reduced sensory
perception
3SN
Intermittent or persistent numbness, reduced tactile
discrimination
and/or manipulative dexterity
*The sensorineural stage is established separately for each hand.
35.
Clinical assessment anddiagnosis
of HAVS
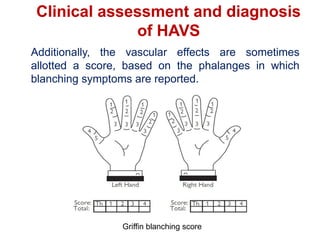
Additionally, the vascular effects are sometimes
allotted a score, based on the phalanges in which
blanching symptoms are reported.
Griffin blanching score
36.
Differential diagnosis ofHAVS
Differential diagnosis of HAVS is based on exclusion
of primary Raynaud's disease and other causes of
this phenomenon, including trauma of the fingers
and hands, carpal tunnel syndrome, thoracic outlet
syndrome, connective-tissue disease, congenital
inferiority of the sympathetic nervous system,
obstructive vascular diseases, polyneuropathies,
syringomyelia, drug intoxication, etc.
37.
Medical management
Removal fromexposure to vibration (absolute
indication - Stage II (III) of VD) tends to reduce the
symptoms of the disease. In case of continuation of
contact with vibration (stage I of VD), a course
treatment is indicated (1-2 times a year depending
on the severity of the symptoms).
There is no well-established and really satisfactory
treatment. Most efforts are directed against
blanching attacks.
• Conservative measures are often advocated
(e.g. the wearing of thermal gloves and warm
clothing, avoidance of draughts and exposure to
cold, wet, windy conditions), but such advice
cannot always be followed in the work situation.
38.
Medical management
• Evidenceon efficacy of other forms of treatment is relatively weak; benefits have
been claimed from:
physical therapy (exercises, compresses, hot packs, paraffin baths, massage,
traction, infrared treatment)
adrenergic receptor blockers (thymoxamine hydrochloride)
stanozolol or prostaglandin E
antiplatelet and antithrombotic agents (pentoxifylline)
calcium-channel blockers —oral nifedipine and diltiazem may offer some
promise
metabolic therapy: vitamins of group B, ethylmethylhydroxypyridine succinate.
• For the relief of acute pain syndrome, NSAIDs are used - meloxicam, diclofenac,
celecoxib, sometimes in combination with antidepressants - Duloxetine,
Amitriptyline, anticonvulsants - Pregabalin, Gabapentin, Carbamazepine, opiates -
Tramadol; and also local therapy - Capsaicin, Lidocaine.
• Surgical sympathectomy may be considered for irreversible cases. For medical or
surgical therapy, the patient should be referred to the appropriate vascular specialist
or hand surgeon.
39.
Fitness for work
-at stage I the ability to work is preserved, however, patients
require dynamic medical observation;
- at stage II(III) ability to work is limited; the patients are
contraindicated to work in contact with vibration, significant
dynamic and static physical force, exposure to adverse
microclimate. Young people need retraining.
Prognosis
For life and health - favorable. As a rule, after 3-7 years after the
cessation of contact with vibration, there is a regression of the
clinical symptoms of the disease, which reclassifies the disease into
"residual effects of vibration disease."











![CS_Project-_HAVS[1]-1 (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/csproject-havs1-11-221122184114-79ddb73c-thumbnail.jpg?width=640&height=640&fit=bounds)




































