Download as DOCX, PPTX
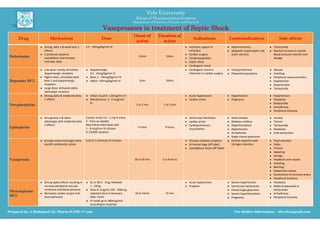
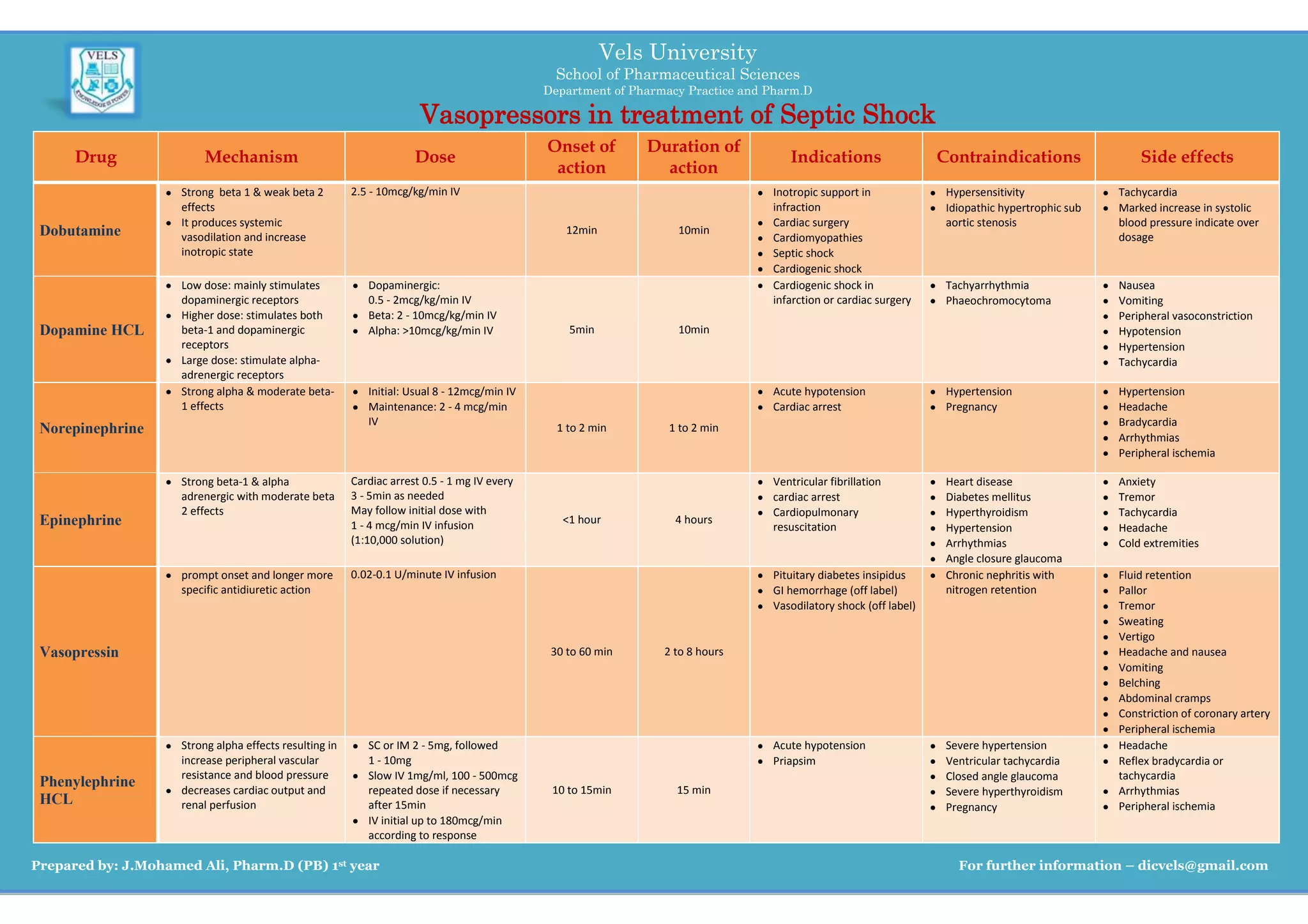

The document summarizes several vasopressors including dobutamine, dopamine HCL, norepinephrine, epinephrine, vasopressin, and phenylephrine HCL that are used in the treatment of septic shock. It provides information on the mechanism of action, typical dosing, indications for use, contraindications, and common side effects of each vasopressor. The vasopressors are compared in terms of their onset of action, duration of action, and adrenergic receptor effects to guide clinicians in selecting the appropriate vasopressor for different clinical situations.



























