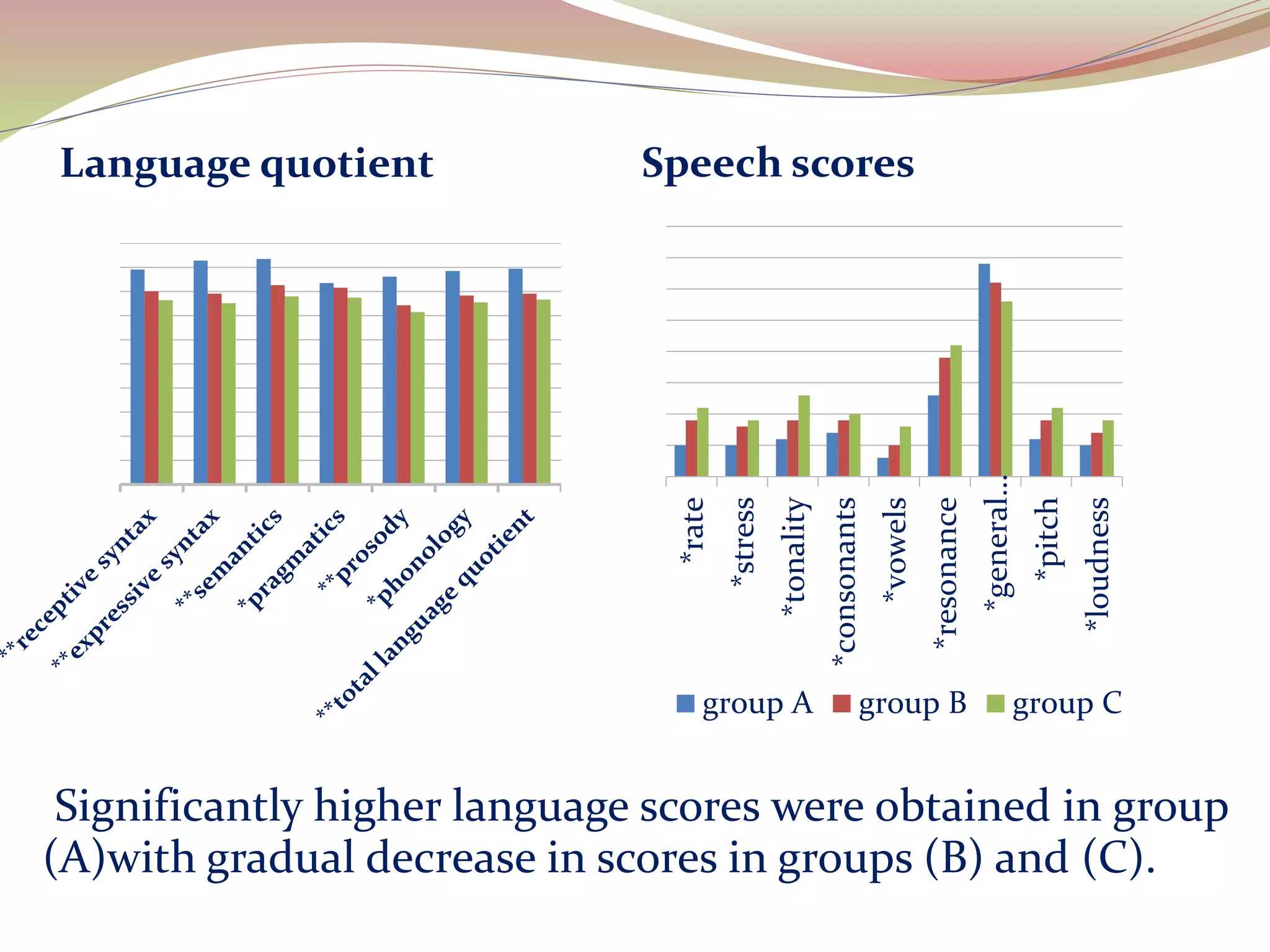
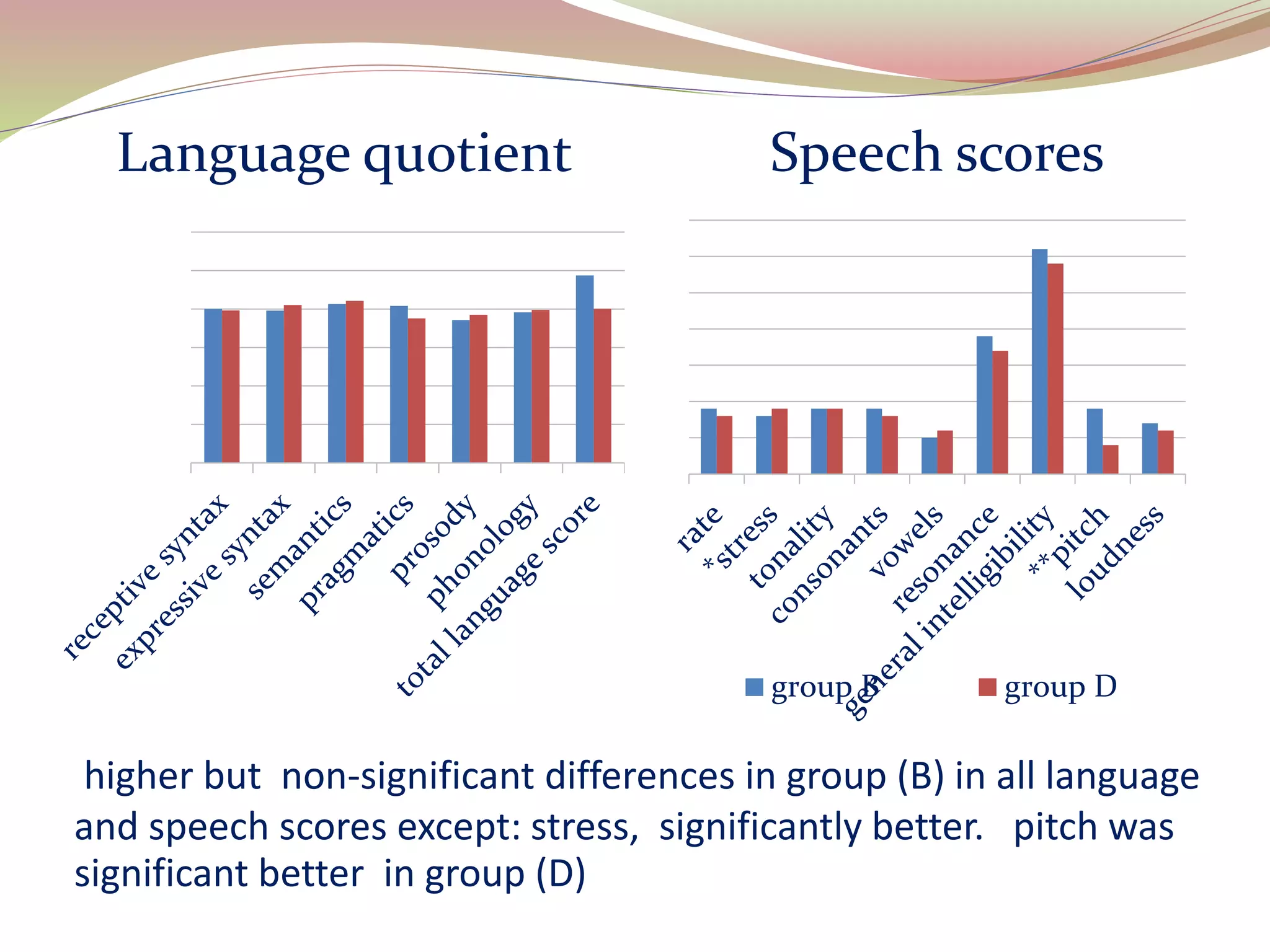
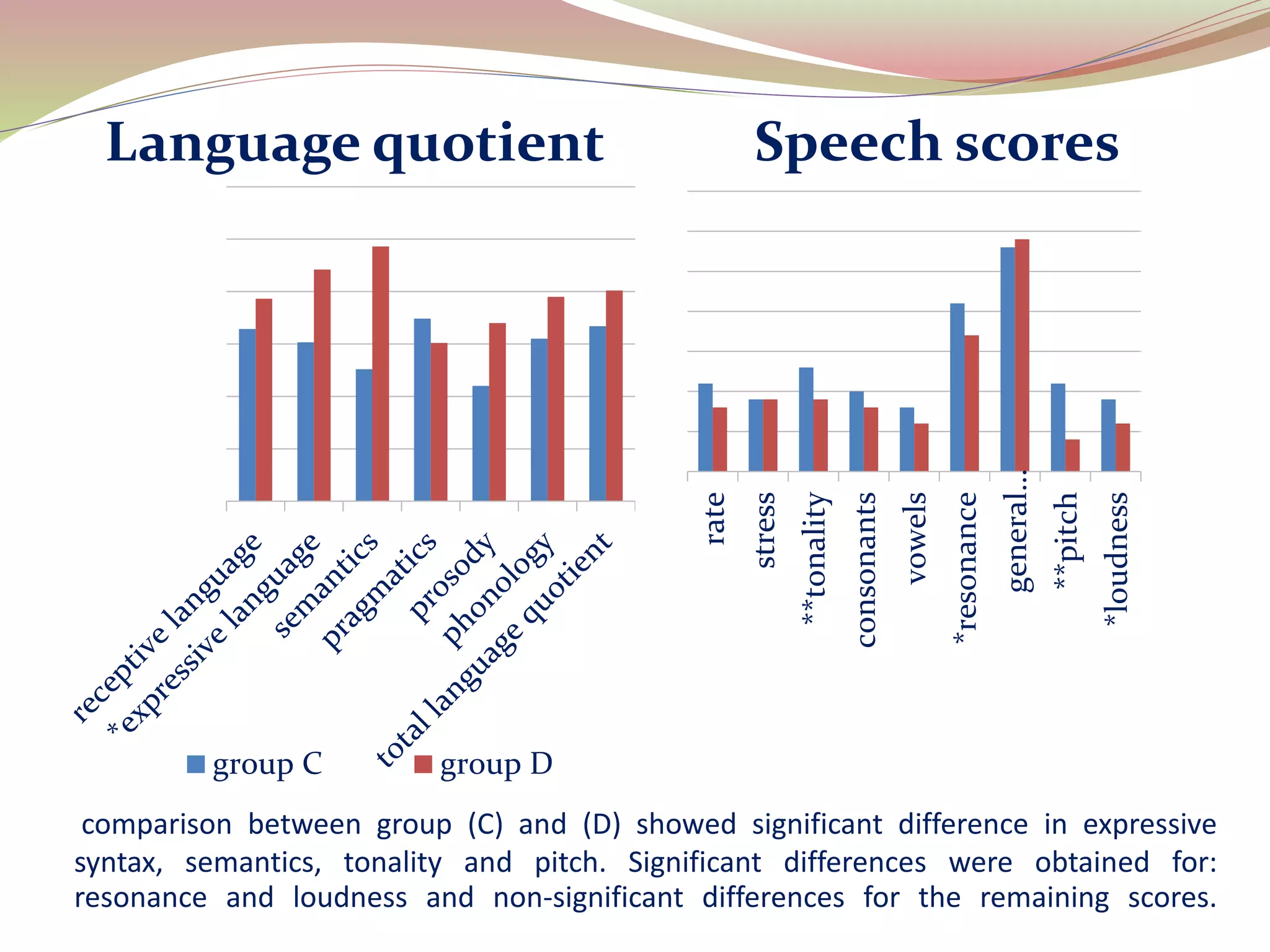
The document discusses the critical period for language acquisition in deaf children and the effects of early intervention. It summarizes a study that assessed language and speech outcomes in 58 deaf children who received hearing aids or cochlear implants at different ages. The study found that children who were amplified before 6 months of age achieved significantly higher language scores than those amplified between 6-12 months or 12-24 months. Children who received cochlear implants after 12-24 months showed better outcomes than those receiving hearing aids only, indicating electrical stimulation can still support language acquisition past the critical period. The document concludes early detection before 6 months is best for language outcomes, and cochlear implants may provide benefits even after 24 months.