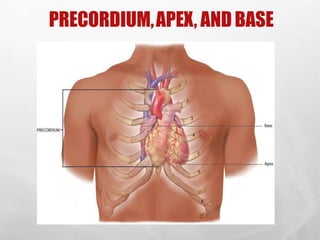
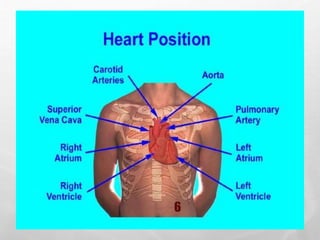
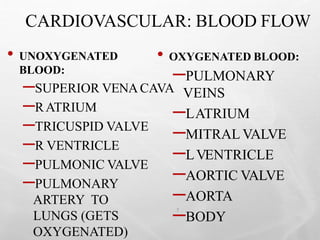
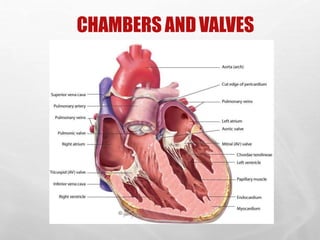
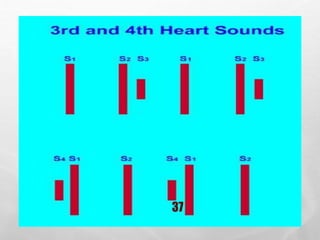
This document provides an overview of cardiovascular system assessment. It describes assessing the heart through inspection, palpation, percussion, and auscultation of the precordium. Key steps include identifying landmarks like the PMI, assessing heart sounds and rhythms, and characterizing any murmurs. The document also reviews the anatomy and physiology of blood flow through the heart, as well as factors like preload and afterload that influence cardiac function.






































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)







