Factors that ImpactVerbal Communication
Pace and intonation
Simplicity
Clarity and brevity
Timing and relevance
Adaptability
Credibility
Humor
7.
Terms Clients MayNot Understand
MedicalTerm
Analgesic
Anti-inflammatory
Benign
Carcinoma
Cardiac problem
Cellulitis
Contraception
Enlarge
Plain language
Pain killer
Lessens swelling and
irritation
Not cancer
Cancer
Heart problem
Skin infection
Birth control
Get bigger
8.
Terms Clients MayNot Understand
MedicalTerm
Heart failure
Hypertension
Infertility
Lateral
Lipids
Menopause
Menses
Monitor
Oral
Osteoporosis
Referral
Terminal
Toxic
Plain language
Heart isn’t pumping enough
High BP
Can’t get pregnant
Outside
Fats in the blood
Change of life
Period
Keep track of
By mouth
Soft, brittle bones
Send to another MD
Going to die
Poisonous
Factors Influencing theCommunication Process
Development
Gender
Values and Perceptions
Personal space
Territoriality
Ability to communicate
(speak, hear, etc.)
Boundaries
Roles and Relationships
Environment
Timing
Congruence
Interpersonal attitudes
Health status
Emotions
Knowledge level
13.
Factors Influencing theCommunication
Process
Boundaries
Professional.Are you and I face book friends??? Why? Should I
ask you to babysit my kids?
Personal
14.
Impairments to Communication
Language deficits
Sensory deficits- such as? Bingo story
Cognitive impairments. Grocery bagger story
Structural deficits
Paralysis
15.
Types of Communication
Social
Unplanned, small talk, develops rapport
Structured
Defined, planned content
Teaching an injection
Therapeutic
Oh boy here we go……
The difference between nice and kind is what?
16.
Therapeutic Communication
See StudyGuide # 1
Therapeutic communication
Promotes understanding and can help establish a
constructive relationship between the nurse and the
client
Client and goal-directed
Helping relationship. Helping is kind
More than a social interaction. Social is nice
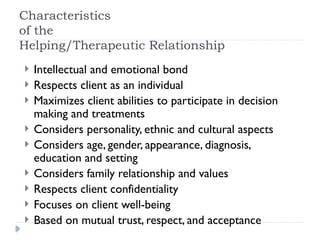
Characteristics
of the
Helping/Therapeutic Relationship
Intellectual and emotional bond
Respects client as an individual
Maximizes client abilities to participate in decision
making and treatments
Considers personality, ethnic and cultural aspects
Considers age, gender, appearance, diagnosis,
education and setting
Considers family relationship and values
Respects client confidentiality
Focuses on client well-being
Based on mutual trust, respect, and acceptance
20.
Youtube therapeutic communications
properpatient care communication
techniques
ATI video therapeutic communications
Use textbook pg 420,421 and 422
(blockers) and scenarios to buddy up and
role-play and present your best
communication
21.
Phases of aHelping Relationship
Pre-interaction phase
Nurse collects data on a client before face-to-face meeting
22.
Phases of aHelping Relationship
Introductory phase
Introductions are made
Develop a degree of trust
Establish confidentiality
Understand the roles of the nurse and the client
Clarify the problem
Structure and formalize contract
23.
Phases of aHelping Relationship
Working phase
Exploring and understanding thoughts and feelings
Facilitating taking action
Includes plans for activities to achieve goals
24.
Phases of aHelping Relationship
Termination phase
Saying goodbye
Review how far the client has come
Can cause a sense of loss or sadness for the client. Assist the
client to accept the end of the relationship without feelings of
anxiety or dependence
25.
Developing Helping Relationships
Listen actively
Help client to identify feelings
Use empathy
Be honest, genuine and credible
Use your ingenuity
Maintain confidentiality
Know your role and limitations
Be culturally aware
How does culture impact communication?
26.
Techniques that EnhanceCommunication
Using silence
Providing general leads
Being specific
Open-ended questions
Using touch
Restating or paraphrasing
Seeking clarification
Seeking validation
Offering self
Giving information
Acknowledging
Clarifying time or sequence
Presenting reality
Focusing
Reflecting
Summarizing and planning
27.
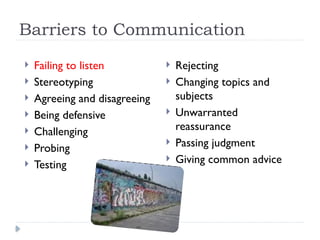
Barriers to Communication
Failing to listen
Stereotyping
Agreeing and disagreeing
Being defensive
Challenging
Probing
Testing
Rejecting
Changing topics and
subjects
Unwarranted
reassurance
Passing judgment
Giving common advice
28.
Process Recording
Aword-for-word account of a conversation
Purpose:To increase awareness and insight regarding
personal communication strengths and weaknesses
29.
Forms of Communication
Non-assertive (Passive or Submissive)
Discounts personal rights
Diminished sense of self-worth
Believes their feelings are unimportant
Avoids problems
Problem doesn’t get resolved
Lingering hurt feelings
Person hopes that the problem will just go away, which rarely
happens
30.
Forms of Communication
Aggressive
Overreacts, blames others, attacks person instead of the
problem
Demanding, hostile, egotistical
Can become violent
Causes distancing, fear
31.
Forms of Communication
Assertive
Faces problem realistically, direct, honest, fair, collaborative
Open expression of ideas
Respects personal rights and ideas of others
Problem is resolved in an appropriate manner
Win/win situation
Everyone feels better
32.
Characteristics of AssertiveBehavior
Own your own feelings
Stand up for personal rights
Do not blame others
Make feelings known by being direct
Possess self-confidence
Focus on the present problem
Don’t bring up the past
Address issue only
33.
Clinical Situation
Youare working as a Certified Nursing Assistant on a
nursing home unit and are asked to work another shift
because they are short-handed.You are frequently asked
because the supervisor knows you are a “good sport”
How would you respond to this situation using assertive
communication?
34.
Response to ClinicalSituation
Assertive approach
“I am in school now. I have a test in the morning. Is there
someway we could have someone else do it?”
35.
SBAR Communication Model
Situation
What is the situation you are reporting?
Background
Important client clinical information
Assessment
What is going on and severity of the problem?
Recommendation
Recommendation for resolving problem or what is needed by
provider
Features of EffectiveGroup Communication
Comfortable atmosphere
Goals/ tasks are clarified
Democratic leadership
Member participation
Open communication
Group decision-making
Cohesiveness
Appropriate conflict
resolution
Power is shared
High problem-solving
skills
Creativity encouraged
39.
Confidentiality
Professional responsibilityas a nurse
Nurses safeguard the trust of clients that information
learned in the context of a professional relationship is
shared outside the health care team only with the
client’s permission or as legally required
Nurses are legally required to report suspected abuse
Nurses also need to tell clients contemplating suicide
that this information cannot be kept confidential
40.
HIPAA requirements
AmericanHealth Insurance Portability and
Accountability Act (HIPAA)
Required as of April 2003
Requires that health information about clients be
secured in such a way that only those with the right
and need to acquire information are able to do so
41.
Confidentiality
Cannot usecomputer password to access any
information on a client, family member, or friend that
does not directly relate to the care of that client
All charts and medical records must be closely
monitored and kept away from visitors and others
seeking information
All papers with clients’ names or identification
numbers must be shredded or disposed of properly
Follow agency policy for documenting sensitive
material (e.g., HIV)
Correct errors per policy
42.
HIPAA Requirements
Computerscreens must be covered or turned away
so no one can read information about a client
Never leave a computer unattended once logged on
Cannot talk about clients in hallways, elevators, or
socially
Cannot leave any information about a client’s
condition on the telephone to a family member or on
an answering machine
Ask the person to call the health care facility for test results
Cannot remove PHI from property
43.
HIPAA Requirements
Cannotuse computer password to access any
information on a client, family member, or friend that
does not directly relate to the care of that client
All charts and medical records must be closely
monitored and kept away from visitors and others
seeking information
All papers with clients’ names or identification
numbers must be shredded or disposed of properly
Follow agency policy for documenting sensitive
material (e.g., HIV)
Correct errors per policy
Reports and Records
What is the difference?
Bedside report is oral
Record is an electronic or paper chart
46.
Purposes of ClientRecords
Communication
Planning client care
Auditing health agencies
Research
Education
47.
Purposes for Records
Reimbursement
Legal documentation
Health care analysis/statistics
48.
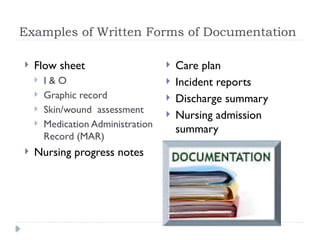
Examples of WrittenForms of Documentation
Flow sheet
I & O
Graphic record
Skin/wound assessment
Medication Administration
Record (MAR)
Nursing progress notes
Care plan
Incident reports
Discharge summary
Nursing admission
summary
52.
Incident Reports
Usedas
Reporting mechanism
Injury prevention tool
Not used as
Form of punishment
53.
Types of ClientRecords
Narrative charting
Written description of client’s condition, specific nursing
care given including teaching and client’s response
Includes client’s complaints and how client is coping
Charted in chronological order
Keep it concise and pertinent
You do not have to chart that client had a bath if he has a bath every
day unless you noted something abnormal such as skin breakdown
during the bath
55.
Types of ClientRecords
SOAP charting
Subjective data
Information obtained from what the client says
Usually quoted
Objective data
Information that is measured or observed with senses
Assessment
Interpretation or conclusions drawn about the subjective and
objective data
Plan
Plan of care designed to resolve the stated problem
56.
S-O-A-P-I-E-R
I =intervention
What was done
E = evaluation
Client responses to intervention
R = revision
Care plan modifications as suggested by evaluation
Charting by Exception(CBE)
Documentation system in which only abnormal or
significant findings or exceptions to norms are
charted
Includes flow sheets, standards of nursing care, and
bedside access to chart forms
Eliminates lengthy, repetitive notes and makes client
changes in condition more obvious
60.
Computerized Charting
Someinstitutions have computers at client’s bedside or handheld
Information can be quickly charted and retrieved
Easier to transmit information between departments
Timely access to information
More expensive and the system can go down halting access
Ethical, security and confidentiality issues
Which generation may be uncomfortable with computerized charting? Do they think
it is rude? Is this cultural?
61.
Guidelines for Charting
Date and time each entry
Entries should be concise, accurate, timely, complete, and
legible
Document in correct sequence
Chart in dark ink, in chronological order, made on consecutive
lines, and appropriately signed Lisa Bechard RN,MSN.
Do not leave any blank spaces on your flowsheets or in your
narrative notes.
62.
Guidelines for Charting
Charts are permanent legal documents and are
admissible as evidence in a court of law
Use only accepted terminology or abbreviations
Use correct spelling
Charting should be appropriate
Avoid personal judgments, opinions, or
interpretations
Errors should be crossed out with a line through it
and “mistaken entry” written above.
63.
Additional Documentation Tips
Use guideline sheets consistently (carry on clipboard)
Be client specific
Do not document for anyone else or another’s actions
Do not chart ahead of time.The client’s condition may
change. Charting care you did not give is fraudulent.
Can I initial meds given because I know the resident always
takes their meds? It’s quicker and I am so busy
64.
More Tips
Avoidimprecise descriptions such as “large amount”.
Don’t chart a symptom such as “client c/o pain” without
also charting what you did.
Don’t give excuses, such as “medication not given because
it was not available”.
Can I initial meds given because I know the resident
always takes their meds? It’s quicker and I am so busy
65.
More Tips
Usepunctuation appropriately
Entries should be in chronological order
Late entries should be recorded appropriately with
“late entry” notation
66.
Need to Know
Commonly used abbreviations
Abbreviations are less frequently used
24-hour clock
67.
Actual Notes onClient Records
The client refused autopsy.
Client was alert and unresponsive.
Client has chest pain if she lies on her side for over a
year.
On the second day her knee was better, and on the third
day it disappeared.
Healthy appearing decrepit 69 year old male. Mentally
alert but forgetful.
68.
Change of ShiftReports
Provides nurse-to-nurse communication from one
shift to the next
May be verbal, written, or audio-taped
Be concise
Avoid gossip, chatter, or judgments
Include significant changes in client’s condition and
action taken
Include contacts with physicians or members of the
health care team
Emotional needs
69.
Telephone Reports
Documentthe date and time, name of the person giving
the information, and subject of information received
Information should be repeated for accuracy
70.
Telephone Orders
Insome institutions, only registered nurses can take
telephone orders from a physician
When the MD gives the order, write it down and
repeat it back to the MD for accuracy
Transcribe the order to the physician order sheet
Document notifying physician in your nursing notes
and nursing actions taken
Use appropriate signature
T.O. Dr. Jones/A. Ruesch, R.N.
Editor's Notes
#1 Be sure to cover:
Therapeutic effects
Communication transmission
Verbal aspects
Nonverbal aspects
Techniques that enhance and barriers that hinder
Essential components of therapeutic relationship
Factors in documentation
Phone/verbal orders
Documentation forms and formats
Shift reports
Discharge planning
Documentation do’s and don’ts
Proxemics
Lifespan considerations
Assertive/passive/aggressive
HIPPA
#2 Communication is an essential and critical nursing skill. It is probably one of the most important tools that you will use as a nurse. Many times we judge a nurse is by their technical skills. But one of the things that sets us apart as nurses is our ability to communicate. In unit one we talked about one of the themes that is common in the definition of nursing is that nursing is an art. Just like other artists (such as painters or musicians) we continue to improve our skill. We learn from our successes and challenges as we interact with others. We communicate with our clients, families, our peers, other professionals and the general public.
Communication is used to gather data, teach and persuade and express caring and comfort. It is dynamic and is a 2 way activity. Documentation is one form of communication which we will address later.
If the nurse is an effective communicator the nurse will be better able to: collect assessment data, initiate interventions, evaluate outcomes, initiate health promoting change and prevent safety and legal problems.
From fall 2006 in-service:
Words are living things. With words we have the power to create or take away.
55% of communication is posture and nonverbal. 38% of communication is tone and 7% of communication is words.
#3 We may not need to spend much time on this as it should be a review from oral communication class.
What is the process of communication?
A sender conveys a message to another. Encoding is involved which is the selection of specific signs or symbols to transmit the message such as choosing which words, language, or tone to use to convey the message.
The message is the transmission itself. It is what is actually said or written and includes body language and how the message is transmitted. Is the message best sent face to face, written or even via TV or YouTube.
The receiver is the listener and he or she must listen, attend, and observe. The receiver's role is to perceive or interpret what the sender intended. The receiver decodes the message by sorting out the meaning of the message within the context of their experience and knowledge. The interpretation may be accurate or inaccurate.
Response is the feedback message the receiver sends to sender. It can be positive or negative and it can be verbal, nonverbal or both.
#4 Verbal communication is spoken or written because we use words. It is a conscious effort.
Nonverbal communication is the majority of our communication – 80-90%. It includes posture, clothing, gestures, touch and facial expression. It also includes factors such as appearance, adornment, gait, eye contact, sounds, personal space, & territoriality. Nonverbal communication can either reinforce or contradict what is said (from ATI (2008).
Another important point about communication is to try not to make assumptions or judgments or stereotypes. We are quick to make judgments. We see someone dressed in a certain way or certain behaviors are witnessed and we jump to conclusions. Culture is an important aspect to consider with nonverbal communication too. Nonverbal communication can vary widely and will require validation of the interpretation on the part of the nurse.
Communication works both ways – nurses draw conclusions from the client’s behavior and nonverbal communication yes, but clients draw conclusions from the nurse’s verbal and nonverbal too.
What impression does a clean lab coat make versus a dirty, wrinkled one?
#5 What does congruent communication mean? If communication is congruent the nonverbal is consistent with the verbal communication. Nonverbal communication can either reinforce or contradict the verbal communication. If someone has a crabby look on their face and yells “you did a good job”. The receiver might wonder if they did a good job or not. They can become confused as to what is the real message. What if you went to a client’s room and they were crying and you asked how they were doing and they said, “I am doing wonderful.” What would you do? How would you respond?
If you said you would want to examine the situation closer. You would be correct. The client’s communication is incongruent so your role as a nurse is to try to find out more. You could question or confront client. You might have to say, “you tell me things are wonderful yet I notice you are crying. Can you help me understand?” Perhaps the person was just being ironic or maybe the person got good news and they are tears of joy. Without clarification you would not know and might be giving inappropriate care and communication.
It is important to remember clients will read the nurse’s nonverbal communication just as we as nurses observe the client’s nonverbal communication. When communication is incongruent – the nonverbal behavior is usually the true meaning because it is unconscious. Whereas verbal communication is under conscious thought.
#6 There are many factors which impact verbal communication. These are important to know and would to apply to written communication as well.
Pace and intonation modify the feeling and impact of a message. Pace might indicate a lot of things such as interest, anxiety, fear, or boredom. Intonation can indicate excitement, sadness, or anger.
When considering simplicity use commonly understood words, be brief and complete. Do not use a 1000 words to say what you can say in 10. People have a limited attention span. You don’t want your point to be lost. Be cautious about using medical jargon (avoid words such as NPO, void etc.). The layperson usually will not understand technical terms. Use words that are appropriate for the age, knowledge, culture and education of the client. You can’t talk to an 80 year old with the same language you could use for a teen.
Clarity is saying precisely what is meant. Brevity is using the fewest words necessary. Enunciation helps with clarity. Speak slowly. Make sure your verbal language is congruent with nonverbal. Avoid ambiguity – where the person is unsure what you mean. Communicate so people know the how, why, (if necessary), what , when, who and where of an event. Being clear helps to avoid assumptions. People do not have to wonder what you mean. Brevity leads to simple and clear messages. Clients are less likely to be confused if we keep the message simple.
Timing and relevance. Timing needs to be appropriate so you can ensure the receiver heard message. Do not overwhelm the client with too many questions at once. Try to communicate when there are not a lot of distractions or their mind is not on something else such as what the physician just told them or pain they might be experiencing. Relevance is about dealing with fear first (such as if students are wondering about a test or the test results for example, I would try to address those needs first then I can start the discussion for the day). Be sensitive to client concerns and needs.
Adaptability involves being flexible depending on cues you get from the client. Tailor your language to meet the client’s needs and ability to understand. If clients look like they don’t understand, then adapt what you say to language they might understand. Or use pictures. Avoid routine speech, medical jargon and modify what you say for the situation.
Credibility is worthiness of belief, trustworthiness, & reliability. Are you reliable? Does the client see you that way? This is very important in establishing relationships. Credibility may be the most important criterion of communication. The nurse must be consistent, dependable, & honest. Convey confidence and certainty. Know the facts and information before responding. And acknowledge limitations. Saying “ I don’t know but I will find the answer” shows credibility.
Humor is good for reducing tension, promoting well-being and as an emotional and physical release. But use it with caution. Consider the timing and appropriateness of its use. Sometimes humor can backfire so assess your clients as to the appropriateness of humor.
Consider language barriers and cultural barriers.
Use appropriate terms – avoid idioms, or slang which can easily lead to misunderstandings.
Don’t speak louder. The person can still hear. Talking louder does not increase the person’s understanding.
Use standard grammar. Give the person time to translate and digest your message.
Be aware that when the client is saying “yes” it does not always mean agreement. It might mean I hear you or a sign of respect.
#7 These two slides are examples of medical terms and how we could say them in plain language. You do not need to know them for a test. I include them to illustrate a point.
#8 From Weis, B. (2003). Health literacy, a manual for clinicians. AMA foundation.
#9 The nurse should assess and be aware of his or her own nonverbal communication as well as that of the client.
Nonverbal communication often tells more about the person’s feelings because it is usually unconscious.
You can usually believe the non-verbal if there is incongruence in the communication.
Use caution in drawing conclusions as we talked about before.
Clarify your assessment with the client – you want to seek validation of what you are seeing. Tell the client what you see and hear and ask for feedback as to if you are correct. Be mindful of cultural differences in nonverbal communication.
Personal appearance involves adornment such as clothing, jewelry, tattoos and piercings. It is a matter of choice and people identify themselves or are making a statement about themselves. It may also be an indicator of feelings. Perhaps if the client is depressed they may take less care with their personal appearance. Personal appearance also tells you something about the client’s financial status, culture, status, religion and so forth. Ask about an adornment you don’t understand. Be sure to validate any nonverbal that you notice rather than making an assumption which may be incorrect.
Posture and gait can tell about self-concept, mood, health, or pain. What does the shuffling gait of a person tell you? Is the person walking really fast? The person curled in fetal position? Describe what you see and validate.
Facial expressions can give away feelings. They can be congruent or disguised. The nurse may have to learn to control and be aware of his or her own expressions at times such as if you are changing a dressing with a foul odor. Eye contact is also included in facial expressions. It may be linked to culture. Take your cue from the client or ask what is appropriate eye contact.
Gestures can enhance or replace communication. Such as giving a thumbs up does not need words. Most Americans know it means something good. Thumbs up means something different in Iran than in the US; “shoo” in US means come here in Asian cultures. Body movement and touch would be other examples. Sometimes gestures can replace words such as sign language or raising one finger for yes and two for no.
I spoke of interpreting client nonverbal communication but the nurse must be aware of these same factors so as not to give the wrong impression to the client.
#10 Email is most common form of electronic communication – now texting is very common as well. And then there are social networking forums. In health care settings it becomes a part of the client record. Be sure to know your agency policy on the use of email.
There are many advantages and disadvantages to electronic communication.
Advantages – it is quick and you can send the same message to a number of people so they all hear the same thing. it saves time. It documents the day and time of the message. It is legible. Be sure words are spelled correctly and the message is proof-read.
Disadvantages – you cannot see the nonverbal language so the message may be misinterpreted. It is impersonal. You can’t take it back and there is documentation of what was sent. This might be an advantage in some situations. Confidentiality is at risk of being compromised. All individuals might not have access to the software or hardware needed – or have the appropriate training.
When not to use electronic communication? In sensitive or highly confidential situations. Such as relaying test results. Or if the sender needs immediate feedback.
Imagine people used to ask these questions and have these thoughts about telephones!
#11 What are the factors that influence communication process? How do they impact positively or negatively communication?
These factors apply to peers & other professionals as well as clients. They are important to know.
Development
There are differences in communication across the life span. Infants communicate through their cries or movement for example. The nurse should know human developmental stages so the nurse is best able to communicate with all ages. Teens might be texting now rather than verbally interacting. Certain conditions may affect the person’s ability to communicate such as the hearing or visually impairments. Be sure to check your text for information about communication across the lifespan.
Men and women communicate differently. Women use language to establish intimacy, seek confirmation, & minimize differences. Men use it to negotiate status, & establish independence. Neither is better, we just need to aware of the differences.
Values are standards that influence behavior. Perceptions are the person’s personal view of an event. It is how a person sees things.
Everyone interprets messages differently. The nurse should give explanations so the patient understands. Clarify what you say and what you see.
Personal space is on the next slide.
Territoriality involves the concept of space and things belonging to a person. We all set our territory. We have our special spots and the dinner table or at church. Or a favorite chair. It makes us uncomfortable when someone else impinges on our space. The hospital room is the client’s space – it becomes their bed, their bedside table and so forth. Obtain permission to remove articles or rearrange or borrow objects from the client’s hospital room.
Roles and relationships – parents speak differently to their children than their spouse. Roles and relationships impact the words, tone, vocabulary etc. that is used. You might use a different tone of voice to say “good job” to a child than to a coworker.
Take into consideration the environment. It should be a comfortable setting with adequate lighting – particularly for the visually impaired. Consider ventilation and temperature. The noise level of the area should be evaluated for the hearing impaired or distractions to others. Privacy is important and in some situations may be more of a perception of privacy than reality. In the hospital there might only be a curtain separating clients so the ability to be totally private is limited. But the nurse should make the setting as private as is possible. The client should feel safe and nonisolated or confused.
Timing we discussed. Health status of the person may influence communication. If someone is really ill they might not feel like talking or may have reduced concentration but maybe if they are well they want to talk about staying healthy and the communication is constant.
Congruence we discussed earlier.
Interpersonal attitudes.
Elderspeak is belittling and doesn’t show respect. It is when we call elders dear or honey. It should not be used. In some clinical settings it is considered a violation of policy.
Caring and warmth will engender emotional closeness. Warmth conveys friendliness and consideration. caring shows deep and genuine concern. Attitudes convey beliefs, thoughts, and feelings about people and events.
Respect is an attitude that emphasizes the worth, & individuality of the person. Be open minded and an active listener. Respectful behavior tells people they are unique and yet the same.
Acceptance is when the nurse neither approves or disapproves – be nonjudgmental in your attitude. In this way the client can be honest and feels accepted. However you may need to restrict acceptance if the behavior is harmful to self or others. Coldness as you can imagine turns off communication.
Boundaries are limits in which a person may act or refrain from acting within a designated time and place. The nurse must try to maintain a professional distance with clients. The client should be the focus of the relationship not the nurse. It is inappropriate to share personal information with a client or to be on friendly terms. Accepting gifts from clients should be avoided.
~~~~~~~~
Knowledge level, emotions and ability to communicate might also influence communication. (are from ATI, 2008)
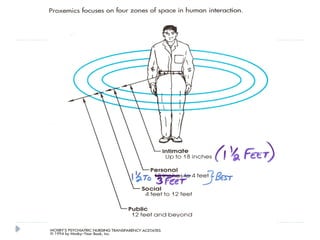
#12 Proxemics focuses on the space in human interactions. We all use all these spaces and they each have their appropriate use. It does have some personal and cultural variability. This is an important concept.
Intimate space is usually reserved for those people we are closest to. We allow these individuals to enter this space around ourselves. With intimate space the nurse should be aware not to violate the space. Ask permission to enter a person’s intimate space when changing a dressing, giving an injection, hugging, or taking a BP. This space is from skin contact to 1.5 feet. Examples are holding a baby, or giving patient care or offering touch.
Personal space is 1.5 – 4 feet (3-4 is best). This is most comfortable for western society. It would be when the nurse is sitting with a client, teaching, or giving meds.
Social space is 4-12 feet. It could be seen when the nurse is making rounds or when someone waves.
Public space is 12 + feet such as in group work or public speaking.
See your text for more detailed information.
#13 Boundaries is an important factor to consider. And is becoming increasingly more important. We spoke in unit one about nurses maintaining boundaries with clients. Boundaries are limits of individuals, objects or relationships. Nurses must maintain boundaries in order to maintain a therapeutic relationship with the client. Our focus should always be on the client and the sharing of personal information kept to a minimum. Sometimes clients wish to enter into a relationship outside of the clinical setting. The nurse should decline this invitation. Accepting gifts from clients should also be avoided. Or spending unnecessary time with the client.
With social media as a part of our daily lives, this too should be considered carefully by the nurse. “Friending” a client crosses professional boundaries. Guidelines for publishing to a social media site include P –which stands for pause and process. Recognize the potential for boundary crossing. C or Choices. Evaluate the situation and options before acting. And then A for action. Make sure you are conducting your self professionally as a nurse. Nurses must remember they must follow the code of ethics at all times. Even when they are not on duty.
#14 Many things can impact the ability to send, receive or comprehend a message. The nurse should determine the client’s primary language. Obtain an interpreter if needed. Any sensory impairment can impact the person’s ability to communicate. Determine if the client uses hearing aids or glasses and if they are working. Check for any medical alert bracelets or if the person uses sign language or is a lip reader. Clients might be unable to understand language due to a disease or condition. Examples are dementia or a stroke. Medications can impact the ability to express oneself or understand. The nurse can assess the client’s ability to communicate. Even unconscious clients are evaluated on the ability to understand. Structural deficits can influence the ability to speak clearly. Examples are a clef palate or tracheostomy. A paralyzed person may be unable to write or use nonverbal communication.
#15 The nurse may use all forms of communication in his/her encounters with clients. Social communication is unplanned and less focused on the client’s needs. It might consist of small talk and be more superficial. You might talk about the weather or sports or what happened on the weekend. Social communication has its purpose in a nurse-client relationship. It might help establish trust and build rapport with the client. Therapeutic communication is focused on the client and is used by the nurse to help the client meet their goals. It promotes understanding and a constructive nurse-client relationship.
Structured communication has a plan to it. For example the nurse might have a plan to teach the client how to give their own injection. There is an agenda the nurse adheres to for the client to meet certain goals. It is more formal in structure.
#16 Be sure you know the difference between social and therapeutic communication. Be sure to review study guide #1 in the syllabus.
Social communication is not focused on the client. There is no goal.
Therapeutic communication promotes an understanding by sender and receiver. The nurse and the client. In this way the nurse and client work together to reach goals. The nurse responds to the client’s verbal and nonverbal message. The nurse focuses on the client’s feelings as well.
Be genuine. Know yourself and be aware of your nonverbal expressions. Treat each person as an individual. Have a nonjudgmental attitude toward each person. Each client should believe he or she is the focus of your attention and care.
#17 Communication is perhaps the most important technique in nursing.
The nurse responds to both the verbal and nonverbal messages and feelings of the client.
Attentive listening is a highly developed skill. The nurse should be aware of what active listening involves and employ it in his or her nursing care. It takes energy, & concentration. If done correctly you will be mentally drained from an encounter. Pay attention to the total message of the client and if their message is congruent. Therapeutic communication conveys an attitude of caring and interest. It is an active process & uses many of the senses – hearing, vision, and touch. With vision the nurse takes in the nonverbal communication, with hearing the nurse not only hears the words but also the tone, inflection, pace and so forth. The focus is on the client and his/her message. The spotlight is on the client. Absorb the content and feelings of the client. Through attentive listening the nurse encourages the client to express him or herself.
Be nonjudgmental and unbiased and try not to react too quickly – let the client finish his or her thoughts. If we are finishing the client’s sentence or thinking of a response before they finish we are not actively listening. If we are thinking of other things we need to do, we are not actively listening because we are not 100% there for the person.
In active listening the nurse may ask questions to clarify and get additional info.
Let client close the conversation – not the nurse. Sincerity is important to establishing trust and rapport – don’t be phony. It will not do anything to build the relationship. Common responses that are used in active listening are:
Nodding or uttering “uh hun”.
Or, repeating the client’s words or saying things like “I see what you mean”.
Physical attending or as it is sometimes called visibly tuning is an important nonverbal behavior. It is evidenced in behaviors facing the client squarely. The nurse’s open posture is another sign and conveys a willingness to listen. Lean in towards the client shows involvement. Maintain appropriate eye contact, and touch and gestures. And finally, to be relaxed or natural. See your text for more actions of physical attending. If done correctly the client will know the nurse is present for the client. It is an expression of empathy toward the client. These behaviors may be adapted for each situation.
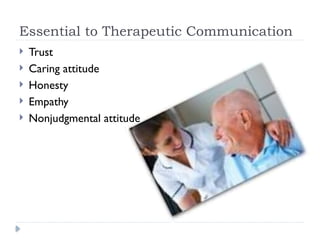
#18 These elements are essential if we are going to be therapeutic. Many of these we have talked about.
Trust is essential to building rapport.
The nurse should have a caring attitude.
Honesty – if you don’t know the answer – tell the client. If you say you will get back to them. Get back to them. Trust will follow.
Empathy –try to put yourself in the person’s shoes and try to understand what they are experiencing.
And have a nonjudgmental attitude.
From ATI (2008)
#19 A helping relationship is a dynamic, ever-changing relationship with another human being whose welfare is the focus of the interaction. This would certainly describe a relationship between the nurse and client. Both parties trust, respect and accept each other. The client is the focus. The relationship encourages independence. The client is part of the planning and implementation. And, the client is engaged in his or her care. Remember from unit one the definition of the client?
Clients learn to help themselves in a helping relationship. They begin to understand how to manage their problems more effectively and develop unused or underdeveloped opportunities more fully. Personnel are more fully utilized. The client believes his/her information is held in confidence.
What are the keys to a helping relationship? Trust and acceptance are keys. The client must believe the nurse cares about and wants to help him or her.
The relationship must go through the prescribed phases because they build on one another. This relationship can develop over weeks or minutes.
I would suggest being familiar with the aspects of the helping relationship and the phases we will be discussing in upcoming slides.
#21 Pre-interaction is the first phase of the helping relationship. The nurse begins to prepare for the encounter even before she or he meets the client. The nurse might get information from the chart or other professionals. Examples of information obtained in this phase are: the client’s name and other demographics, and the medical and social history. In this stage the nurse should identify his or her own feelings and needs – especially as a student. You might be nervous and wonder how the relationship will evolve. There might be some stereotypes or biases on the part of the nurse that have to be dealt with before meeting the client.
The goals of this stage are: planning the encounter, gathering information and identifying information to be disclosed.
#22 In the introductory phase the nurse and client observe each other. The nurse will introduce her or himself and explain the role and perhaps some of what is planned for the client’s care.
Both parties form judgments at this stage. It is the chance to make the best impression. The tone of the relationship is established at this phase.
The nurse opens the relationship and clarifies the problem. During this phase the client views the nurse as a competent professional, and is someone who is honest, open and concerned about the client. The client believes the nurse will try to understand and respect the client and his/her beliefs, values and culture. The client begins to feel comfortable talking with the nurse and expressing feelings and sensitive issues.
The nurse and client structure and formulate a contract – what care will be done and how. We let clients know what we will keep confidential. This phase includes introductions and a social exchange to put the client at ease. The client understands the purpose of the relationship and that he or she is active in his or her plan of care.
The client may be resistive at first- so what can the nurse do?
The nurse can display caring, competence, genuine interest and a nonjudgmental attitude.
Trust is important but this also involves some risk for the client. They may be unsure if they can share personal information with the nurse because it leaves them vulnerable. Once trust is established the client will share more.
#23 In the working phase the bulk of the relationship occurs. Caring develops. Both parties view each other as unique.
There should be a mutual plan that both parties are working towards. The goal of this stage is mutual goal setting and outcomes. Exploring and understanding occur as the nurse and client work together to accomplish the goals.
There are two stages to the working phase – exploring and understanding thoughts and feelings and facilitating and taking action. Exploring and understanding thoughts and feelings phase requires several skills.
Empathic listening and responding. Empathy is listening and understanding how the client feels. The nurse must be aware of both his or her own and the client’s verbal and nonverbal communication. Nonverbals such as a smile, laugh, forward leaning torso, gestures, or nodding the head relay comfort, caring, & a helping, healing relationship. In this relationship we, as nurses, enter into the client's world.
Therapeutic empathy is used – this is a learned, conscious way to convey understanding of another’s emotional state and point of view.
Emotional empathy is also used – this is where the nurse has a spontaneous response to client’s condition or needs.
The nursing skill of respect is used as is genuineness. Respect shows we take the client’s point of view seriously. Genuineness solidifies the rapport between the nurse and client. It shows the client the nurse is human. Spontaneity, nondefensiveness, consistency, and openness show the client the nurse is genuine. Self-discipline on the part of the nurse is important though – only share personal information when appropriate. Self-disclosure must be appropriate. The nurse should willingly but discreetly share personal information. Try to avoid the attention being focused on you, the nurse. We want the attention to be on the client.
Concreteness means the communication is not vague. Have the client talk in concrete and specific vs. general terms. You might have to ask for clarification and more data.
Confrontation occurs when the nurse clarifies client discrepancies in thoughts, feelings and actions. Do not judge but point out discrepancies that allow the client to explore and better understand him or herself.
Facilitating taking action is the second phase of the working relationship. In this phase the nurse will assist the client with taking action. It is up to client to act though. The nurse will collaborate with the client on ways to meet the goal as well as provide information and appropriate teaching. During this phase the nurse may provide support & offer options.
Other important skills the nurse might use are: assist with decision making, goal setting & reinforcement.
#24 This is the phase of saying good bye. It might be several hours after meeting the client or it may be days, weeks, months or even years. Allow time for the client to adjust to the idea of independence. Sometimes this is hard for the client. And it may be hard for the nurse too.
Hopefully the client will have a positive outlook and be able to handle problems by the time termination occurs.
Begin planning for the end of the relationship in advance. Give the client time to prepare. Give them a time of transition to get used to the idea. Make referrals as needed to home care or public health for example. Provide any follow-up that might be required.
Summarize or review the process – how far has the client come? What has been their progress?, Reminiscence over experiences, & make referrals if needed.
#25 Each nurse has the capacity to develop helping relationships. No special training is needed. The slide lists ways all nurses can develop a relationship with each client to help him or her meet his or her goals. See you text for more details.
#26 I will not go over all these techniques but I would suggest being familiar with them. They should be a review of the oral communication course. I would suggest that you study the chart in the text with this information and the one on barriers. Be sure you can identify when a particular technique or barrier is used. What is fascinating is to know these really work. They do elicit information from clients. Clients will share more information if we use these techniques. They do help to establish trust. They show the client you are listening and care about them.
I would suggest you try these in the clinical setting or in your job now. You can even use them in your personal relationships or in relationships the workplace.
We will be using these in the clinical assignment of process recording which we will discuss in a minute.
#27 The biggest inhibitor to communication is failing to listen. I would be familiar with these barriers too. They should be a review of your oral communication course. Be sure to consult your text for examples and definitions of these. They are important to understand. When you understand them you will aware of times when you use them and strive to avoid their use. These barriers can destroy attempts at establishing trust and rapport. It makes the client feel as though you are not listening to them or that they are not unique. Saying things like “why did you wait so long to come to the clinic?”, Or “don’t worry it will be alright.” Or “I have seen lots of people with this disease, you will be ok.” Or if you are uncomfortable with the topic and you change the subject. Are all forms of barriers to communication.
#28 You will use process recording in clinical. In a process recording assignment you will record verbatim what both you and the client said and then the important part will be when you analyze what you said and did. Did you use therapeutic communication or a barrier? And what was the result? Did you establish rapport or destroy it? I point this out now because when you get to clinical it will become a resource for you.
#29 There are three main communication styles. This is probably a review of oral communication class. The first of these is the submissive communicator. This person does not stand up for him or herself. They tend to agree to do things or make a decision because they want to avoid conflict. In this way they maintain their self-esteem. Even if they do not like the decision they will do it because they hope the problem will go away. When people communicate passively the problem really does not resolve. These communicators will typically hold on to the grudges and hurt feelings. And usually no one knows their feelings are hurt. One day they explode from all these pent up hurt feelings and bring up things from years ago. These might be the people who are always saying “yes” to things not because they want to but because they don’t want to hurt someone or are afraid to say “no”.
It ends up being a win/loose situation.
The passive communicator stuffs feelings and settles with the status quo. They don’t honor their own integrity. The passive person tends to go with the other guy so their own needs do not get met. They accept what is unacceptable and bear the burden. (from American Nurse Today 9/2007)
#30 The aggressive communicator is the opposite end of the spectrum. They are the bulldozers. They try to always get what they want no matter what. They are egotistical and they tend to think the world revolves around them and what they want. They use communication tactics such as humiliation, domination, control and embarrassment. They tend to insult, use sarcasm, belittling comments, or be rude. If they can lower the other person’s self-esteem their self-esteem is boosted. They tend to alienate people because no one wants to be around them because they can overreact, scream, blame others, or become violent.
This too is a win/loose situation.
#31 The most effective way to communicate is the assertive form of communication. I think sometimes people think of assertiveness as a negative trait. In reality assertive communicators strive for a win/win outcome. They own their feelings and use a lot of “I” statements. They are able to express how they feel and their views in a respectful way. They respect the thoughts and feelings of others and work to resolve the issue. They do not hold grudges or sandbag past conflicts and bring them up later. They do not bulldoze or try to push their own agenda.
The assertive person stands up for what is right. (Sounds like a client advocate) And they work to try to find solutions and common ground. Learning to be assertive can be hard to do at first. Some pointers are if you are asked to do something that you really do not want to do again—ask yourself what can I do to prevent this from happening again.
If you are asked to do extra again – say – “I have to get back to you”. This gives you time to consider what you really want to do. (from American Nurse Today 9/2007)
In terms of the nurse using assertive communication, using “I” statements encourages discussion. It gains the attention of the listener and gives the message of wanting to work cooperatively on behalf of the client. When the nurse communicates with the physician or other health care professional it is important to be clear, concise, organized, and fully informed about the client data. The nurse should provide information about the current situation, background information that relates specifically to the current situation, the assessment findings of the current situation and a recommendation that addresses the client’s need.
#32 Someone who communicates assertively clarifies what they see and hear to avoid ambiguity or misinterpreting the message. The assertive communicator doesn’t blame others or bring up past issues. They own their feelings, talk about the current issue and are self-confident about expressing their views, feelings and ideas. They focus on the situation at hand not the past. These communicators are seen as self-confident.
Joint Commission is issuing alerts at health care institutions in regard to communication. Rude language is not only unpleasant but may impact client safety and quality of care. Institutions are to have policies in place to deal with a code of conduct and process for managing unprofessional behavior. From American Nurse September/ October 2008
#33 Read this scenario and come up with a possible response.
#35 The SBAR model is used by nurses to communicate effectively with doctors. By using these guidelines the nurse can get right to the point in a professional manner. See the text for more details.
#36 These three behaviors are new to nursing. It is something that is more frequently occurring. Theses behaviors result in low productivity, absenteeism, emotional exhaustion or poor retention.
Incivility is rude, discourteous or disrespectful behavior, it shows little regard for others. It takes many forms such as insults, dirty looks teasing, or ignoring others.
Lateral violence is directed at coworkers at the same level – between staff nurses for example. It may be physical, emotional, or verbal abuse or aggression. Examples are backbiting or sabotaging.
Bullying is offensive, intimidating, insulting behavior or abuse of power. The person feels humiliated, stressed, threatened and so forth. This behavior is repetitive over at least 6 months and directed at someone who cannot defend themselves.
#37 The nurse must find solutions for disruptive behavior. It should not be tolerated. Protect colleagues and strive for collaboration. Build consensus and respect through skilled communication and goodwill. Promote education to learn more and support policies that support strong communication strategies.
#38 We will not discuss group work too much in first semester. You learn more on this in future semesters. But since you have a group project it might be good to talk about a few aspects of group communication.
A group is two or more people who have shared needs or goals, take each other into account in their actions, are held together & set apart from others by their interactions.
There are many advantages to working in groups. One advantage to group work is the shared workload. You have the value of expertise from others in the group. You can learn a great deal from others. You can experience personal growth from the knowledge and experience you gain. And you get support from group members.
Group dynamics occur in every group. Different roles are assumed by group members in every group as they evolve. Some members are supportive. Some members are destructive. Some are natural leaders and some are negotiators and others just want to do the work.
Try to include some of the features listed in your groups. Be sure to have a comfortable, welcoming atmosphere. Stick to the task so people do not feel as though they are wasting time. Encourage creativity and open thinking but if there are conflicts try to use appropriate communication to resolve the issue.
You will be involved in many groups throughout your nursing career so it is important to know how to communicate effectively in a group and be the best group member you can be.
#39 Confidentiality is Included in the ANA code of ethics so from that we know this is one important hallmark of nursing communication. Our clients trust we will maintain confidentiality and the information they share with us is secure. It is the nurse’s duty to protect the client’s confidentiality. As a student nurse you are held to these same standards.
Information is only shared with those authorized to know. Only health care workers involved in the care of that client have access to health information.
The agency is the rightful owner of the client’s record but the client has a right to a copy of the original.
A client’s record is a legally private document. Take this seriously! Violations of confidentiality can have severe consequences. An example of a time when confidentiality may need to be broken is if the client informs the nurse of suicidal thoughts. The nurse would inform the client she or he would have to notify someone. Confidentiality may need to be breeched when certain communicable diseases must be reported to health authorities in order to protect the public.
#40 HIPPA was originally designed to make health insurance billing transferability easier but it was transformed into more confidentiality requirements and health care was required to make dramatic changes in fulfilling the obligations of the law. HIPPA requires that health information about clients be secured in such a way that only those with the right and need to acquire information are able to do so.
Some other considerations with HIPAA are: Do not give information to an insurance company unless client permission is obtained.
No information can be given even to family members unless they are authorized to receive it.
It is permissible for students to obtain information on clients they working with and we are bound by code of ethics and confidentiality.
When you begin clinical you cannot take client health information out of the clinical setting without the instructor’s review. No name can be associated with the information.
Only put initials on notes so there is no way to identify the client.
#41 As I mentioned before client records and health information cannot be removed from facility property. Do not share your computer password with others. As a student and a nurse you must abide by HIPAA requirements so it is important to be familiar with them and how they are applied in the work setting and clinical.
#42 Many of these protections you might be familiar with. Be especially aware of conversations you have about clients. They should not be held in the hallway, elevator or other public place where they could be overheard. You cannot discuss the information with family or friends. Even if you are out with classmates you should not discuss clients in the public setting – it may be overheard. Or putting information on facebook. This would constitute a breech of confidentiality. In clinical you are not allowed to remove personal health information from the property.
#43 As I mentioned before client records and health information cannot be removed from facility property. Do not share your computer password with others. As a student and a nurse you must abide by HIPAA requirements so it is important to be familiar with them and how they are applied in the work setting and clinical.
#45 Reports are an oral, written, or computer-based communication that conveys information to another. It might be at the change of shift or if a nurse from one facility talks to nurse in a facility to where a client will be transferred.
Records are written or computerized - an example is the client record. The process of making an entry into a client record is known as recording, charting or documenting.
A record is also known as a chart. It is a legal document and formal evidence of care that is given. There are several different kinds of documentation that will be discussed in future slides. The type used will depend on the work setting.
Joint Commission says charting must be :
Timely,
Complete,
Accurate,
Confidential and client specific.
#46 What are the purposes of client records?
Communication is one purpose. It is a method for all disciplines involved in the care of the client to interact.
It reduces duplication, repetition, fragmentation, & delays in care.
Documentation is an efficient and effective method of sharing information.
All members of team use the chart to plan care. Providers use data in the record to create a plan of care and document the evaluation of the effectiveness of care. For example the MD looks at vital signs and labs and as a result orders an antibiotic, PT, or a social worker or dietary consultation.
The auditing process uses client records where individuals monitor the care and competence of people giving care such as peer review or Joint Commission.
Documents are used for research. They are a rich source of data. Both past and present data might be used.
Education is an important purpose of charts. Students of all kinds can obtain a picture of the disease, treatment, strategies, and outcomes of a client’s care.
#47 Reimbursement is another use for records. Care provided must be in the chart for Medicare and other insurances to pay. Remember DRGs? Care must support the DRG. The documentation can also support additional care and justify additional billing.
A record is a legal document. The record can be subpoenaed and used in for evidence in court.
You might have heard the adage “if it is not charted - it is not done”. This holds true. If the care given is not in the client record it is assumed the care was not provided. To protect yourself as a nurse you must be thorough in your documentation of care that is provided to a client.
Health care analysis means charts are used to identify services used. It helps agencies determine costs and if services are appropriately used. For example how many nurses are needed in certain departments or shifts. All information is used for future planning and cost containment. Administration may use the information in client records to determine what generates revenue (such as the number of births, deaths, ER visits, or surgeries) - and where and how expenses can be managed.
#48 A client’s chart may include many different forms. Some examples are listed on the slide. It would important to know the various types of forms the nurse might find in a medical record and how they are used.
Flow sheets are forms used to document client care in a quick way. Examples of the use of flow sheets in client records are:
I&O –intake and output, Vital Signs, Bowel Movements, neuro checks, weights or a skin assessment.
There are others too depending on where the nurse works. Special reports or diagnostic records might be recorded on a flow sheet. The idea behind flow sheets is for someone to easily look and note the client’s progress or regression over time. The nurse would only need to look in one place to see the client’s vital signs for 24 hours, for example. Most facilities or nursing units have special flow sheets depending on the types of clients they usually care for. For example a neurological unit might have special flow sheets for neuro checks. Some forms in charts are universal such as the MAR or nursing progress notes. Although they might take on different formats they are in every client chart. Incident reports are not a part of the client record but are a form of documentation. They are usually kept with the risk manager of the facility.
Kardexs are widely used. A kardex is a concise method of organizing and recording data. Some places call them a worksheet or client schedule. They are usually done in pencil so they can be easily changed as the client’s condition changes. A kardex may or may not be a part of permanent record.
Examples of information on the kardex are: the client’s name, age, religion, or mental status.
The client’s physician, type of surgery, the diagnosis, or next of kin.
A list of meds and IV fluids, treatments and procedures may be found there. Diagnostics may be listed.
Allergies are typically on a kardex.
Physical needs such as bathing, nutritional needs, elimination needs and so forth are commonly included in a kardex. Or it might take the form of a problem list, goals, & interventions. Not all kardexs have all this information. It will depend on the place where you work. They do provide a quick and easy place to find out general information about a client.
Care plans can be traditional which are developed for each client and therefore unique to each client. Or they might be standardized. They are used for all clients with the same diagnosis. Standardized care plans are usually institution- based. They are determined by standards of practice. For example the obstetric unit may have care plans that are used for every OB client because some parts of OB client care are given to each client. Then the nurse adds information to customize it to a particular client. The advantage to standardized care plans is it reduces documentation time for the nurse. We will talk about what is in a care plan when we are in unit 5.
Nursing progress notes are either handwritten or computerized. Nurses document the client’s progress toward achieving desired outcomes. Nursing assessments, interventions or actions are documented along with the client's response to care.
Consult the text for more information on what would be part of a discharge summary.
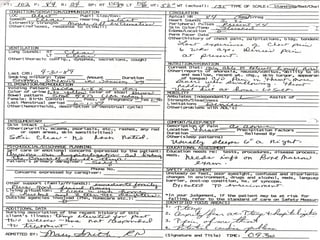
#49 This is a sample of a care plan. It will make more sense after we talk about the nursing process. It has categories of a nursing diagnosis, client goals, what the nurse plans to do to meet the goals and if the goals are met.
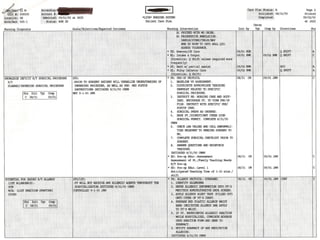
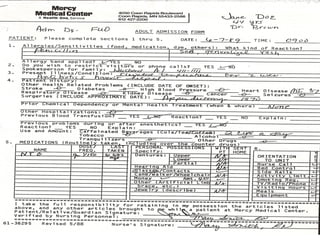
#50 This slide and the next is an example of an admission form. It is very busy. It gives you an idea of the amount of information and detail of information the nurse gathers at the time of admission.
#51 More of the admission form. As you can see the nurse collects data on the client by system to get a complete look at the client’s status and needs.
#52 Incident reports should not be used to penalize employees. The incident report should be used as a data collection tool and way to document an event. Not all accidents can be avoided. We are human and unintended events occur. The event should be recorded as accurately as possible to document what occurred and corrective action taken. The nurse who discovers the event or occurrence should be the nurse who completes the report and it should be done as soon as possible so the event is remembered as accurately as possible. Time has a way of distorting reality. Any witnesses to the event should complete a form as well.
An incident report is not kept in a client record nor the fact a form was filed. Just the event and corrective action are documented in the client chart. Usually they are maintained with the risk manager. It is his or her job then to review these reports. If it is noted there are several similar incidents corrective action on a facility level can occur. Say there are several injuries with a new piece of equipment. The risk manager might decide to have more training or talk to the manufacturer. The incident report should not be used in a punitive way but used to improve client care.
Information included in an incident report would be the client demographic data, the date, time and place of the incident. Describe the event as it occurred including the equipment involved or medication. Omit any conclusions or theories of what happened or caused it to happen. Be very factual. List any witnesses and the client account of what happened.
#53 Over the next few slides we will look at various types of client records. You should be familiar with the different types of client records.
Narrative records are a type of source-oriented record.
In a source oriented client record each discipline documents its own notes in a separate section of the chart. For example nursing has a section of the chart, PT, OT and so forth. It is the traditional charting method and is slowly being replaced by other methods.
What are source-oriented record components? Usually they include admission data, doctor’s orders, the medical history, nurse’s notes, and any special reports, flow sheets & diagnostic records.
Narrative charting is a written description of the client’s condition, specific nursing care given including teaching and client’s response. It includes client’s complaints and how the client is coping. It is written in long form just like a story. So it is important to keep it concise and pertinent so others do not have to read through extraneous information. Usually routine care is documented on flow sheets. Narrative documentation is charted in chronological order. Sometimes narrative charting is combined with other forms of charting. For example if charting by exception is used the nurse might want to expand on the information by including more information in a narrative format.
An advantage of narrative charting is each discipline can easily follow the client’s progress and what is done.
Disadvantages are
Information is all mixed up,
Communication between disciplines is reduced,
It might be hard to check on a problem because there are many places to look,
Information is fragmented and it may be hard to read. It is hard to be chronological between disciplines.
A lack of coordinated care could result and it may give an incomplete picture of the client.
#54 This is another narrative charting sample. You can see the client’s statements are in quotes. And it is written in phrases.
#55 In the problem oriented medical record (POMR) data are arranged by problem rather than the source. There is a care plan and progress note for each problem. In the SOAP charting system all problems are numbered. All disciplines chart by the problem and, contribute to problem list, care plan and progress notes. There are not separate sections in the chart for different disciplines.
SOAP records consist of:
A data base which contains all information on the client. This is constantly updated. The admission, health history, diagnostic tests, social and family history and nursing assessment are included in the data base.
A problem list is created from the data base and is numbered so care providers can chart on the problem. Problems are continually added to list and taken off as resolved.
The plan of care is started by the person who lists problem (it can be the physician or nurse) and other disciplines add to it.
Progress notes use SOAP for charting. As a problem from the problem list is documented it is numbered and SOAP charting is done.
S or subjective data is information obtained from what the client says. What the client says is usually quoted.
O is objective data. This is information that is measured or observed with the senses. What the nurse observes, palpates, hears and so forth is included in the O section of the charting.
A is for assessment. Here the nurse documents the interpretation or conclusions drawn about the subjective and objective data. A description of the client’s progress and is located here.
P is the plan. A plan of care is designed to resolve the stated problem. The plan is located here as well as any revisions.
Advantages are this type of documentation encourages collaboration and a problem list makes it easy to track client status. Disadvantages are it is hard to keep the problem list current and can be repetitive in charting. It is sometimes inefficient because each problem is charted on separately and everyone is not capable of keeping charting current due to differing abilities.
#56 Some new forms omit S&O and start with A for assessment. Others add the I, E and R after the P.
I is the intervention – what specifically is done for the client.
E stands for evaluation and includes the client’s responses to interventions of the nurse and physician.
R is revision. Here care plan modifications as suggested by evaluation are reflected.
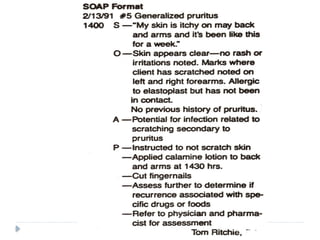
#57 This is a SOAP charting example. You can see the problem is # 5 which is generalized pruitis (this was listed on an earlier slide) and the SOAP documentation by the nurse about this problem only. If the client has several problems that required documentation each would have to be SOAP charted separately. So you can see where there might be duplication of documentation.
#58 In this system the chart includes assessment flow sheets and progress notes. After the data is collected the nurse determines the problem in nursing diagnosis format. We will talk about that more in unit 5. The problems are numbered. The interventions are listed that are developed to address the problems and the evaluation of those interventions is documented. This method eliminates a care plan form but it also means the nurse may have to search through the chart to find the information.
#59 Charting by exception or CBE utilizes standards of nursing practice as its framework. It lends itself to computerized charting but can be done in the traditional paper method as well.
The hospital must decide on what is “normal”. And it typically follows the body systems.
In some situations it may be unit specific. For example, the hospital might say “normal” parameters for the skin or integumentary system is skin is intact, warm and dry, turgor is brisk, there are no bruises or rashes or open wounds. If the client meets these criteria a check mark or other marker indicates the client meets the criteria. No other documentation is needed. But if the client has a stage one pressure ulcer, the client does not meet the criteria so it is an exception and needs to be documented in more detail.
Flow sheets are often used and check marks or other symbols are used to indicate if the data is within normal limits or if there are exceptions. For example a check mark meets the client meets the criteria. A asterisk might mean the client doesn’t meet criteria – therefore it is an exception and the nurse describes exceptions in probably a narrative type note.
Opponents to CBE think it may be too brief and not enough information is included to alert others to changes in condition. There is also the presumption the nurse assessed all the criteria for each system.
People who like it do so because it saves time and duplication. It is brief and changes in the client's condition are more obvious.
#60 Computerized charting is used for many parts of client care. Examples are admission data, care plans, medications or routine care.
Advantages are many.
It is legible. There is less of a chance of misinterpreting orders etc.
It saves time and reduces duplication. It can be easily updated.
It reinforces standards of care and there is less of a chance of the administration of inappropriate drugs.
Disadvantages are many too.
Everyone needs computer knowledge and the training is longer. Client privacy may be at risk.
It frequently costs more for equipment, software and training.
Someone may click on the wrong client or wrong field because of not double checking and put data in the wrong record. The nurse may accept what the computer says without thinking through it – leading to overdependence on the computer.
See more about advantages and disadvantages in your text.
What are some ways computers are being used?
To record care, meds, and client progress.
To collect assessment data, or for documentation of progress notes.
It is used for health care planning or med administration.
It can warn about medication contraindications or warn the nurse about dangerous parameters such as vital signs out of the standard range.
Nursing care plans are often computerized.
It might assist with staffing and client acuity stats.
It helps with care charges or use of equipment and supplies and ordering labs, x-rays, or dietary can be done quickly.
Key points to remember. Nurses still need to individualize care for each client and nurses are bound by professional ethics to maintain pt privacy and confidentiality.
#61 Nurses document evidence of nursing care given in the client’s chart or record. It is a legal document and must meet legal standards. If done correctly documentation is legal protection for the nurse as well. Remember the nurse uses the chart to obtain information about the client.
Documentation needs to reflect the nursing process. It needs to show the nurse assessed the client, planned and provided care and followed up. (Joint Commission reinforces this in its regulations.) A nursing responsibility is to protect and safe guard the confidentiality of client records.
What are some ways nurses protect confidentiality of charts?
There are some important guidelines to follow with documentation. Document as soon as possible after an assessment or intervention. There are many reasons for this. The information is fresh in your mind and there is less likelihood of forgetting to document important information. Others who might want to view the information such as the physician will have timely access to it. Document in chronological order. If the time sequence is altered the nurse will need to document the recording as a late entry.
Be sure you are documenting on the correct client record. Always check to be sure.
What are some documentation don’ts?
Do not chart in advance. Do not use vague words such “appears comfortable”. It means different things to different people and is open to interpretation. Do not chart for another care provider. There is no need to say “the client” or use the client’s name in the chart – it is assumed it is the client since it is his or her chart. Never alter a chart – this is falsification of records.
Some places have signature sheets you must sign so your initials can be aligned with a signature.
Review the information on this slide. Make sure each entry is dated and timed. As a nursing student you will sign the document with your first initial, last name and NS for nursing student. Do not leave any blank spaces on flowsheets or in narrative notes. Draw a line through any blank areas. This is to safeguard you so no one can document under your name. In addition to the information on the slide - make sure you are charting on the right chart. Accuracy is important. Double check the name. The name should be stamped or on computer screen.
#62 Be specific - use exact measurements instead of words such as “large”, good, bad, small, or normal.
Don’t use general words such as good or normal. They can lead to confusion and are open to interpretation.
Don’t use white out or erase a recording, or use pencil. Draw a line through the error, write mistaken entry and your initials. Use correct spelling – not doing so reduces your credibility as a professional. It also might lead to errors such as a medication that might be misspelled. Proofread your documentation. Write on every line. Leave no blank spaces or boxes. Cross out blanks.
Use only Joint Commission approved abbreviations and abbreviations accepted at your facility. If in doubt, spell it out. Be aware of the Joint Commission do not use abbreviation list. Abbreviations may save time but they can cause health care errors.
Use the nursing process as a guide when you record data. Record what is done as well as what is not done. If care was not performed you must provide information as to why it was not performed and who was notified. Reasons why care was not done might be client refusal or health condition.
Be objective & specific. For example saying “refused meds” versus “uncooperative”. Uncooperative shows a judgment is made on the part of the nurse. Be factual – do not make assumptions or interpretations that might be challenged or incorrect.
Chart all teaching and chart the client response to all care given.
Chart the client’s words and place them in quotes. Chart the client’s condition changes, interventions which were done and action taken. Documenting a client change in condition without charting the follow up care may show negligence on the part of the nurse. Charting should be complete yet concise. Sometimes this is hard at first but it is something you will learn as you go.
Items to chart would include nursing assessments, nursing interventions, client problems and comments, the client response and progress or regression and the nurse’s communication with other health care workers. Also record rationale for something that was not done.
Only chart what is appropriate to the client’s care and health. You may be accused of liable or invasion of privacy if inappropriate information is in the client record. For example documenting a client is involved in the sex trade after overhearing a conversation of a client with a prostitute would not be appropriate. Recording irrelevant information could be considered libelous.
#63 Do not chart what someone else assessed, heard, said, taught etc. If it is critical use quotations and attribute the remarks to the person. Do not chart ahead of time. The client’s condition may change. Charting care you did not give is fraudulent.
If you use flow sheets use the correct symbol. For example using a check mark on a flow sheet may indicate care was done, an asterisk might mean the care was not done.
#64 This slide is fairly self-explanatory. If you discover a concern about a client such as tachycardia you must chart what you did about it. Not doing so shows poor nursing care and may be considered malpractice or negligence.
What might you say instead of a large amount of drainage? How can you make it more precise? You might say, 3 cm area of serosangineous drainage on one dressing.
Info from www.Nso.Com
#65 Follow the guidelines on the slide when documenting. Be sure to document if a client refuses treatment or meds. Report this to the nurse manager and the physician.
#66 Be sure you know the 24 hour clock and abbreviations in your syllabus. There may be some agency specific abbreviations you will need to use where you work. Computerized charting uses less abbreviations. Abbreviations as a whole are used less frequently due to errors from misinterpretation. Joint Commission has recommended a listing of abbreviations that should be avoided. See the list in your text.
#67 Here are some actual notes from a client record. They may seem funny but the serious side is they reflect poorly on the person who wrote them and leave the person open to legal consequences and they may leave the reader confused.
#68 What is the purpose of the change of shift report?
It provides continuity of care and communicates specific information to a person or group. It is a summary of client needs and details of care given and the care to be given.
Some do’s and don’t for report that would be important to know are:
Do not give extraneous details
Be accurate and complete, & concise.
You might provide more detail on a new client. Pass on information on priorities of care that the next nurse might have to be aware of. For example perhaps the client is going for surgery and the day nurse will need to prep the client by 0900. Reduce distractions and stick with the responsibility of giving report. Try not to get sidetracked and avoid gossip and making judgments. Avoid discussing information that has always been normal or routine care.
Taped reports save time. And it leaves a nurse on the floor to cover clients. Some don’t like it because there is less of a chance to ask questions. Once the nurse gets report the nurse gives report to the CNA etc. Some places give report in person and others at the client’s bedside.
What to include in report -
Name, room, age, physician.
The reason for admission for new clients.
Any tests in the last 24 hours and the results.
Any significant changes in the client’s condition.
The nursing assessment, nursing diagnosis, plan, interventions, & evaluation.
Any PRN meds that were given and the results.
Emotional needs of the client and how they were met.
Any RN/MD orders and any care priorities that will occur at the start of shift such as a medication or prep for a test.
The text provides some handoff communication models you could try in clinical.
#69 Telephone reports might be used if transferring a client to long term care facility from the hospital.
When conducting a phone report have the chart ready, have all the data with you and be prepared with significant information such as vital signs. Tell the person what you observed and what you did. Document what was reported and to whom.
Include in the report
Demographics – age, sex and so forth.
Vital signs, lab data and nursing interventions are also included. For example how a wound was treated.
This conversation is also documented in the client’s permanent record.
If you are receiving the report be sure to repeat the information back for accuracy. Then document accurately and completely the information reported and who provided it and the date and time.
#70 How to take a telephone or verbal order is important. In some institutions, only registered nurses can take telephone orders from a physician. Sometimes in WI an LPN can take orders in long term care. In some organizations verbal orders are against policy because of the increased chance of error.
When you talk to the physician have the chart ready, have all data with you and be prepared with significant info such as vital signs and be able to relate what you observed and what you did.
When the physician gives the order, write it down and repeat it back to the physician for accuracy. This is the important point and is true for verbal orders as well as telephone orders. If the physician said, Polly, I'd like you to give Mrs. Jones 20 units of regular insulin subcutaneous now and call me in an hour with the blood sugar.” The nurse would repeat back to the physician “Dr. Smith I understand you to say you would like Mrs. Jones to have 20 units of insulin subcutaneous now and call you in an hour with her blood sugar. This allows the physician to hear the order and determine if it has been understood correctly.
Question any ambiguous, contraindicated or unusual orders. Ask for clarification and spelling. It is a good idea to have someone else listen in. Some facilities do not allow verbal orders.
As I mentioned before, once the nurse takes the order, the nurse will transcribe the order to the physician order sheet. The nurse will put T.O. And the physician and nurse’s name for the signature to indicate it was a telephone order. Then the physician will countersign the order at a later time. Document notification of the physician in your nursing notes and nursing actions taken. Many places are moving away from verbal orders to increase client safety.