By the endof session learners will be able
to;
Review communication process
Recognize the level of communication
Practice types of communication into
clinical setting
Identify the factors influence
communication
Determine the role and function of
administration in communication
3.
To be aneffective leader the nurses
needs the primary leadership skills as
skills of personal behavior,
communication, organization, and self
examination.
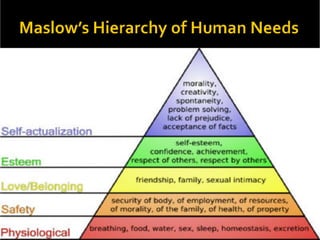
4.
Communication
is the processin which people affect one
another through the exchange of
information, ideas and feelings.
is the process that requires interpretation,
sensitivity, imagination, and active
participation.
(Jenner, 2007)
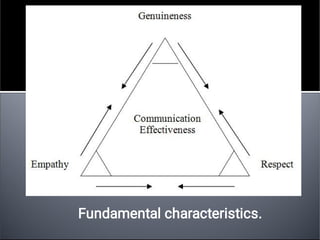
Respect and empathyfor the client .
Good communication skills .
Tolerance of values and beliefs different
from one’s own .
Unbiased attitudes .
Patience .
Awareness of gender issues.
15.
1.
2.
3.
4.
5.
1- Non-verbal communication
Iswhat is observed and send .
* Is often more important than verbal
communication it includes:
Paralanguage : (tone of voice , stream of
talk)
Kinesis : (all body languages and facial
movement ).
Proxemies : (the distance between the
sender and the receiver ).
Touch .
Cultural arte facts : (the way a person
dressed , make up ) .
16.
2- Verbal communication:
Iswhat is said and heard .
*It is the content of communication :
Use an appropriate tone of voice .
Give verbal encouragement .
Ask questions .
Paraphrase .
Seek clarification.
17.
“It is powerfulform of communication that
occurs within an individual. this level of
communication is also called self-talk, self-
verbalization, self-Instruction, inner thoughts and
inner Dialogue”. (Balzer-Riley, 1996)
People’s thoughts strongly influence perceptions,
feelings, behaviour and self-concept
Positive self-talk can be used as a tool to
improve the nurse’s or client’s health and self-
esteem.
Self instruction can provide a mental rehearsal
for difficult tasks or situations.
To develop self awareness and positive self-
concept that will enhance appropriate self-
expression.
18.
It is one-to -one interaction between the nurse
and another person that often occurs face to
face.
It is most frequently used level.
It takes place within a social context and
includes all the symbols and cues used to give
and receive meaning.
Meaningful interpersonal communication results
in exchange of ideas, problem solving
expression of feelings, decision making, goal
accomplishment, team building and personal
growth.
19.
Transpersonal communication isinteraction that
occurs within a person’s spiritual domain. Many
persons use prayer, meditation, guided reflection,
religious rituals, or other means to communicate
with their “higher power”
Sellers and Haag (1998) found that nurses
enhance the spirituality of clients and their
families through prayer, active listening and
therapeutic communication, conveying
acceptance, respect and a non-judgmental
attitude, instilling hope and using presence and
touch.
20.
Small-group communication isinteraction that occurs
when a small number of persons meet together.
Usually goal directed and requires an understanding of
group dynamics.
Nurses work on task forces or committees, lead client
support groups, form research teams, or participate in
client care conferences, a small-group communication
process is used.
More effective when they are a workable size, have an
appropriate meeting place, suitable seating
arrangements and cohesiveness and commitment
among group members.
21.
Public communication isinteraction with an
audience. Nurses have opportunities to speak
with groups of consumers about health-related
topics, present scholarly work to colleagues at
conferences, or lead classroom discussions
with peers or students.
Requires special adaptations in eye contact,
gestures, voice inflection and use of media
materials to communicate messages effectively.
Increases audience knowledge.
22.
Communication is anongoing, dynamic
and multidimensional process.
Nursing situations have many unique
aspects that influence the nature of
communication and interpersonal
relationships.
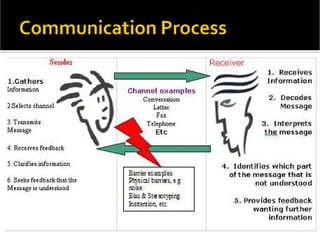
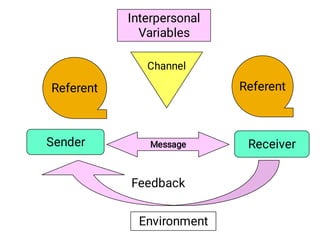
The referent motivatesone person to
communicate with another. In a health
care setting, sights, sounds, odours, time
schedules, messages, objects, emotions,
sensations, perceptions, ideas and other
cues initiate communication.
25.
The sender isthe person who encodes and
delivers the message and the receiver is the
person who receives and decodes the message.
The sender puts ideas or feelings into a form.
Responsible for the accuracy of its content and
emotional tone.
Acts as a referent for the receiver.
Sender and receiver roles are fluid and change
back and forth as two persons interact, sending
and receiving may even occur simultaneously.
Closer the relationship the more likely they will
accurately perceive one another’s meaning and
respond accordingly.
26.
The message isthe content of the
communication. It may contain verbal, non-
verbal and symbolic language.
Nurses can send effective messages by
expressing themselves dearly, directly and in a
manner familiar to the receiver.
Communication can be difficult when
participants have different levels of education
and experience.
The nurse must be sure clients can read before
sending messages in writing.
27.
Channels are meansof conveying and receiving
messages through visual, auditory and tactile
senses. Facial expressions send visual
messages, spoken words travel through auditory
channels and touch uses tactile channels. The
more channels the sender uses to convey a
message, the more clearly it is usually
understand.
They send and receive information in person by
informal or formal writing, over the telephone or
pager, by audiotape and videotape, through fax
and electronic mail and through computer
interactive and information sites.
28.
Factors within boththe sender and receiver :
Perception formed by one’s expectations and
experiences.
Each person senses, interprets and understands
events differently.
Educational levels
Developmental levels
Socio-cultural backgrounds
Values and beliefs, emotions, gender, physical
health status and roles and relationship.
Variables associated with illness, such as pain
anxiety and medication effects
29.
The environment isthe setting for sender-
receiver interaction.
Noise, temperature extremes, distractions
and lack of privacy or space may create
confusion, tension and discomfort.
Nurses must try to control the
environment as much as possible to
create favourable conditions for effective
communication.
30.
Communication is unsuccessfulif
senders and receivers cannot translate
each other’s words and phrases.
Medical jargon
Technical terminology used by health care
providers.
31.
Conversation is moresuccessful at an
appropriate speed or pace.
Pacing is improved by thinking before
speaking and by developing awareness of
the cadence of one’s speech.
32.
Tone of voicedramatically affects a
message’s meaning.
Simple question can express enthusiasm,
anger, concern, or indifference
A clients voice tone often provides
information about his or her emotional
state or energy
33.
Effective communication issimple, brief,
and direct.
Fewer words result in less confusion.
Clarity is achieved by speaking slowly,
enunciating clearly, and used examples to
make explanation easier to understand.
Repeat important part of message.
Brevity achieved by using short sentences
and words that express an idea simply
and directly. “Where is pain? is much
better than “I would like you to describe
for m e the location of your pain.”
34.
Timing is criticalin communication, even
though a message is clear, poor timing
can prevent it from being effective.
Messages are effective if relevant to the
situation.
Eg:“Client facing an emergency surgery,
discussing the risks of smoking, is less
relevant than explaining peri-operative
procedures.
Assessment:
Gather data aboutfactors that influence
communication these include the participant’s
internal factors and characteristics, the nature
of their relationship, the situation promoting
communication, the environment, and the
socio-cultural elements
Asking personal questions
Changingthe subject
Automatic responses
False reassurance
Sympathy
Asking Explanations
Approval or Disapproval
Defensive responses
Passive or aggressive responses
Arguing
40.
Maintain a nonjudgmentalinteraction
Guide patient to reinterpret experiences
rationally
Track verbal interaction with clarifying
statements. Avoid changing the subject
(unless in the best interest of client).
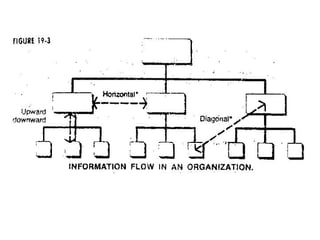
Upward communication
Managers filterthe messages
Suggestions appeals group meetings
open door policies
Crosswise communication
Horizontal flow.
Diagonal flow.
47.
Lack of planning.
Unclearassumptions.
Poorly expressed messages.
Loss of transmission and poor retention
Poor listening and pre mature evaluation.
Impersonal communication.
Distrust , threat and fear.
Information overload.
50.
Verbal message –content
Nonverbal message – process
Goal is to achieve congruence
Influence of culture
Brings about clientinsight, control of
symptoms, and healing
Nurse needs thorough understanding of
communication and how to build a
positive nurse-client relationship
54.
Basavanthappa,B.T.(2008). Nursing Administration.New
Delhi: jaypee brothers.
Erb, G., & Kozier, B. (1998). Loss, Grieving and Death.
Fundamental of Nursing: concept, process, and
practice. (5th ed.). Addison: Wesley
Mohr, W. K. (2003). Therapeutic Relationship and
Communication. Psychiatric-Mental Health Nursing.
(5th ed.). Philadelphia: Lipincott.
Potter, P. A., & Perry, A. J. (2003). Fundamental of nursing.
St Louis: Mosby
Sullivan, E. J; & Decker, P. J. (2001). Effective leadership
& management in nursing.
(5th ed.). Jew jersey: Prentice Hall.