CONTROL OF CARDIACCONTRACTILITY.
Cardiac contractility, the heart’s ability to squeeze and pump blood, is
controlled by a complex interplay of factors at the cellular level and by
the autonomic nervous system.
At the cellular level,calcium ions, electrical signals, and specific
proteins like troponin and myosin are crucial.The autonomic nervous
system through the sympathetic and parasympathetic
pathways,influences contractility through neurotransmitters and
hormones.
3.
Cellular Level Control:
Calcium :
Calcium ions are the primary regulators of cardiac muscle control.
When an action potential travels down the cardiac muscle cell
membrane, calcium ions flow into the cell,triggering the release of
more calcium from the sarcoplasm reticulum (SR).
This influx and release of calcium leads to the binding of calcium to
troponin,which in turn allows myosin to bind to actin, initiating the
muscle contraction.
4.
Electrical signals :
The heart’s electrical conduction system , which is part of
autonomic nervous system, controls the rate and rhythm of the heart
beats. Electrical signals propagate across the heart, causing the
muscle cells to contract in a coordinated manner.
Specific proteins :
Troponin and myosin are key contractile proteins. Troponin regulates
the interaction between actin and myosin, while myosin, with the
help of ATP, pulls on actin filaments, causing muscle shortening.
5.
Myosin Light ChainKinase (MLCK) :
MLCK, along with other kinases, regulates myosin light chain
phosphorylation, which affects the force and velocity of contraction.
Phospholipase C(PLC) and Inositol Triphosphate (IP3) :
PLC and IP3 are involved in regulating calcium release from
sarcoplasm reticulum, further influencing contractility.
6.
Autonomic Nervous SystemControl :
Sympathetic Nervous System :
The sympathetic nervous system releases norepinephrine
(noradrenalin), which binds to beta-adrenergic receptors on the heart
muscle cells. This activation increases calcium influx, leading to faster
and stronger contractions.
Parasympathetic Nervous System :
The parasympathetic nervous system releases acetylcholine, which binds
to muscarinic receptors, leading to a decrease in heart rate and a weaker
contraction.
7.
Catecholamines :
Catecholamines(epinephrine and norepinephrine ) released by the
adrenal glands also play a role in increasing heart rate and contractility.
Angiotensin II :
Angiotensin II, a hormone, can constrict blood vessels and indirectly
affect the heart’s pumping ability.
In summary,cardiac contractility is controlled by a combination of
intracellular calcium regulation, electrical signals, specific protein
interactions,and the influence of the autonomic nervous system and
other homones.
8.
CARDIAC ELECTROPHYSIOLOGY
Cardiacelectrophysiology is a branch of cardiology and basic science
focusing on the electrical activities of the heart.
The term is usually used in clinical context,to describe studies of such
phenomena by invasive (intracardiac) catheter recording of
spontaneous activity as well as of cardiac responses to programmed
electrical stimulation-clinical cardiac electrophysiology.
However,cardiac electrophysiology also encompasses basic research
and translational research components.
9.
Specialists studyingcardiac electrophysiology, either clinically or
solely through research,are known as cardiac electrophysiologists.
Electrophysiological studies are performed to assess complex
arrhythmias,elucidate symptoms,evaluate abnormal
electrocardiograms,assess risk of developing arrhythmias in the
future,and design treatment.
These procedures include therapeutic methods (typically
radiofrequency ablation ,or cryoablation) in addition to diagnostic
and prognostic procedures.
10.
Other therapeuticmodalities used in the field include antiarrhythmic
drug therapy and implantation of pacemakers and implantable
cardioverter-defibrillators.
Cardiac arrhythmia – improper beating of the heart,whether
irregular,too fast (tachycardia) or too slow (bradycardia). It occurs
when electrical impulses in the heart don’t work properly.
Key aspects of cardiac electrophysiology
Diagnosis –identifying the specific type of arrhythmia and the
underlying electrical pathways responsible for it.
11.
Evaluation
Assessing theseverity of the arrhythmia, its potential impact on the
heart, and the effectiveness of treatment options.
Treatment
Various therapies are offered, including medication management,
catheter ablation (a procedure that can disrupt the electrical
pathways causing the arrhythmia), and device implantation
(pacemakers, defibrillators.
Defibrillators -
12.
Types of electrophysiologystudies :
Basic electrophysiology study : This involves measuring baseline
intervals,atrial and ventricular pacing,and extrastimulus testing.
Invasive electrophysiology study : this is the most common
type,involving the insertion of catheters into the heart to record
electrical signals and perform pacing or ablation.
None-invasive electrophysiology study : this includes techniques like
remote device monitoring and ECG monitoring,which can assess the
heart’s electrical activity without invasive procedures.
13.
Research
Ongoing researchcontinues to improve diagnostic and therapeutic
techniques, including new methods for mapping the heart’s electrical
activity,developing more effective drugs, and using advanced imaging
techniques to visualize and understand the heart’s electrical
conduction.
BASIC CONCEPTS OFELECTROCARDIOGRAPHY
Electrocardiography is the branch of physiology that deals with the
recording and analysis of the electrical activities of the heart. The
heart generates the electrical impulses in form of electrical potentials.
The electrical impulses are propagated in form of time-dependent
waves of depolarization. By placing electrical contact point called
electrodes at suitable locations on or within the body,the electrical
impulses could be detected,amplified and transcribed into a graphic
record by the instrument called electrocardiograph (ECG Machine).
16.
The graphicrecord of the heart electrical activities recorded from the
body surface constitutes what is known as electrocardiogram (ECG) .
The term electrocardiogram was formally introduced by William
Einthoven in 1893 at a meeting of the Dutch Medical Association.
Electrocardiopgram (ECG) is the graphic record of the electrical activities
of the heart detected at the body surface by the aid of electrodes and
lead system.
17.
The electricsignals generate by the heart are detected by means of
the electrodes usually attached to the limbs and chest wall. The
electrocardiogram is a summation of a vast number of systematically
propagated electrical activities taking place within the heart.
The standard electrocardiogram (ECG) is a graphic record of the time-
dependent electrical potentials generated by the atrial and ventricular
muscle.
Ionic movement produces electric impulses across the membrane of
the cardiac cells. There is marked difference in the intracellular and
extracellular concentrations of sodium and potassium ions.
18.
At theresting phase,the concentration of sodium io is higher in
extracellular fluid (ECF) while that of potassium ions is higher in the
intracellular fluid (ICF).
Consequentially, the charge measured across the atrial and
ventricular cell membrane is approximately -90mV,with the inside
negative to outside which is positive. Hence,the cell is said to be
polarized.
When the cell is stimulated,the cell membrane becomes permeable to
the sodium ions ,which rapidly shift inside the cell.
19.
The sodiuminflux reverses the transmembrane potential even as
potassium moves out of the cell.The pole changes and the cell is said
to be depolarized in a process called depolarization.
With time, sodium-potassium ATPase (Na+-K+ ATPase),a pump in the
cell membrane actively pumps three sodium ions out of the cell in
exchange for two potassium ions brought into the cell .This restores
the relative negative charge within the cells and hence the resting
pole.This process is called repolarization.
20.
The electricalimpulses generated and propagated during the process
of depolarization and repolarization of the myocardial cells are
detected by electric contact points(electrodes) placed on the body
surface
With the aid of a machine called electrocardiograph, the detected
electrical impulses from the heart muscles are transcribed into a
graphic record called electrocardiogram (ECG).
The branch of physiology that study the recording and analysis of ECG
is called electrocardiography.The study of the normal electrical
activities of the heart is called electrocardiophysiology.
21.
The normallygenerated and propagated electrical impulses of the
heart are symbolically presented on the standard graph paper with a
unique standard denotations termed PQRST complex.
The denotations can be measured in terms of magnitude,
duration,orientation and shape. The various parameters had been
standardized.
Therefore, alterations in the standard pattern provide clues for the
diagnosis of some cardiac lesions at a particular time .
22.
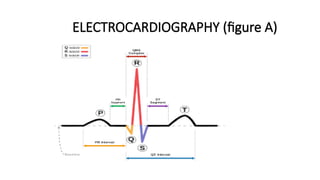
ELECTROCARDIOGRAM (ECG)
Electricalimpulses of the heart are in form of waves of depolarization
and repolarization. The waves represent the time-dependent
electrical activities of the different regions of the heart that are
transcribed on the graph paper as either upward(positive) or
downward (negative) deflections separated by isoelectric lines.
The pictogram formed from the deflections constitutes what is called
electrocardiogram as denoted by PQRST complex (figure A)
23.
STANDARD DESCRIPTIVE TERMSFOR ELECTROCARDIOGRAM
P wave : atrial depolarization
P-R segment : isoelectric line from the end of atrial depolarization to the
beginning of ventricular depolarization(QRS complex).
P-R interval : period from the onset of atrial depolarization to the beginning
of ventricular depolarization.
Q wave : first negative deflection in ventricular depolarization (QRS
complex).
24.
R wave: first positive deflection in ventricular depolarization.
S wave : second negative deflection in ventricular depolarization or the first
negative deflection after R wave’
Complex : a combination of two or more waves’
QRS complex : ventricular depolarization.
S-T segment : isoelectric line from the end of ventricular depolarization to the
beginning of ventricular repolarization.














![Shadechapter01.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter01-150421101218-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









