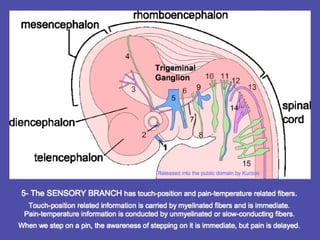
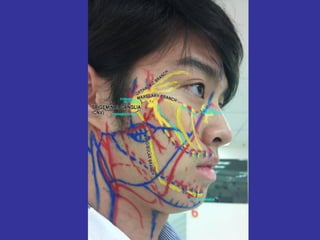
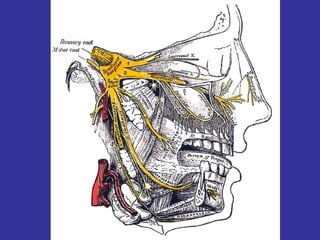
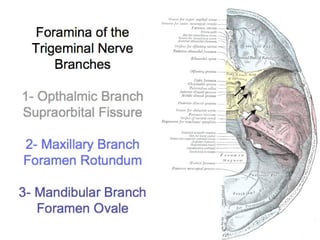
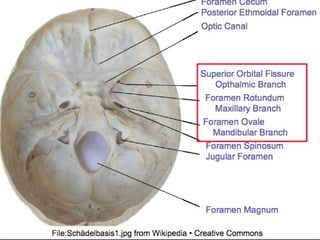
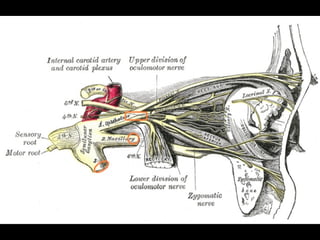
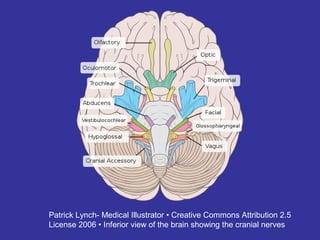
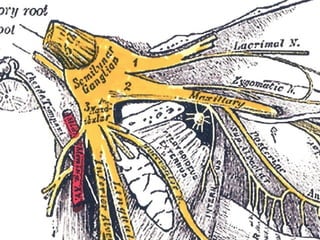
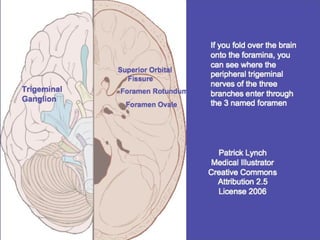
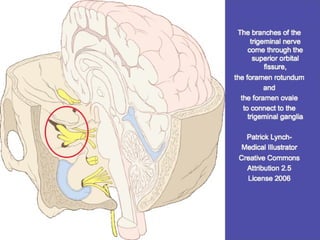
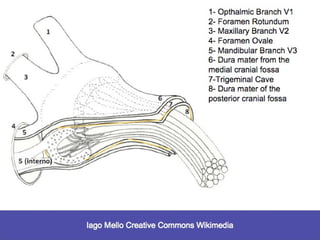
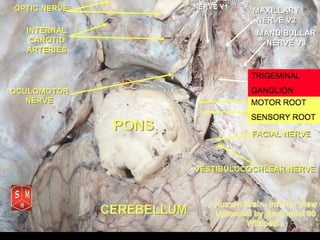
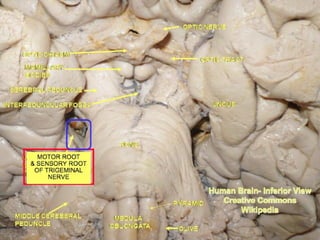
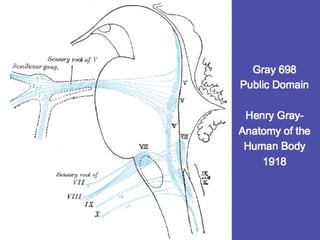
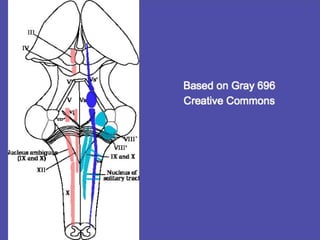
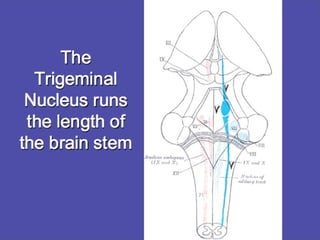
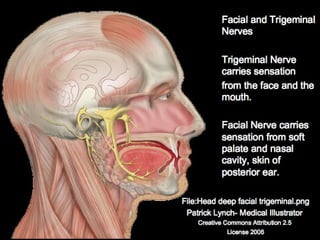
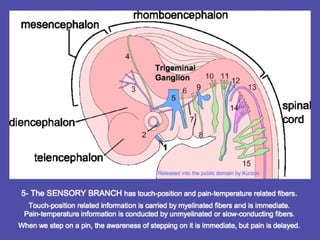
The trigeminal nerve is responsible for sensory innervation of the face and front parts of the head. It has three main branches that enter the skull through different openings and relay sensory information to the trigeminal ganglion and trigeminal nucleus in the brainstem. The trigeminal nucleus is a collection of nerve cells that receives all sensory information from the face, including touch, pain, and temperature. It contains a detailed map of the face and relates this sensory input to different areas of the brain. Disturbances in trigeminal nerve function can lead to pain conditions like trigeminal neuralgia.