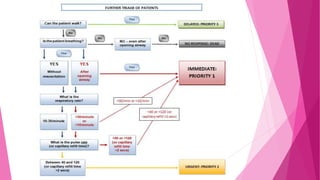
This document discusses triage in trauma care. It begins by defining triage as sorting patients based on need to receive the right care at the right time. The goals of triage are to rapidly identify urgent cases and ensure treatment is timely and appropriate. Patients are assessed and assigned a priority level based on factors like vital signs, injuries, and pain level. Cultural considerations must also be taken into account. The document then describes the roles of various professionals involved in trauma situations and transport of patients to facilities that can provide the necessary care.