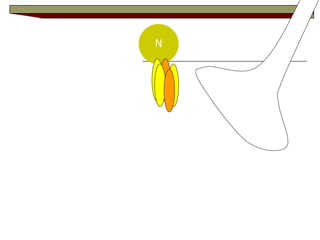
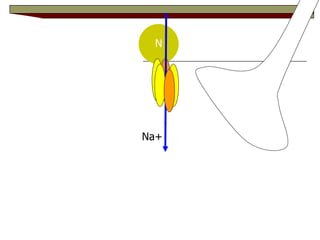
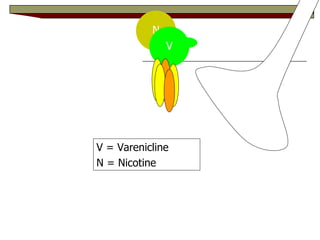
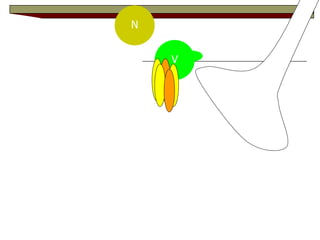
The document discusses treating tobacco dependence and cigarette smoking as a chronic disease. It describes the harms of cigarette smoking and factors that perpetuate tobacco dependence, including nicotine addiction, withdrawal symptoms, and conditioned responses. It recommends treating tobacco dependence as a chronic condition using behavioral interventions, pharmacotherapy like nicotine replacement therapy, bupropion, and varenicline, and relapse prevention strategies. Clinical guidelines emphasize identifying and treating every tobacco user with effective medications and counseling.




![FDA Drug Abuse Advisory Committee – June 9, 1997 “Tobacco dependence is a…[serious,] chronic, relapsing, life-threatening illness, that requires…long-term medical management.” Curtis Wright, MD, PhD Deputy Director, Div. of anesthetics, Critical Care, & Addiction Drug Products Food & Drug Administration](https://image.slidesharecdn.com/treatingtobaccodependencerevised2-100121205150-phpapp02/85/Treating-Tobacco-Dependence-Revised-2-11-320.jpg)