Download to read offline
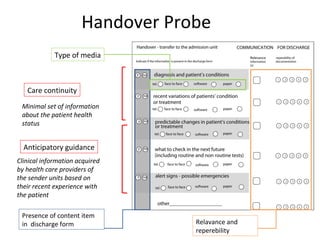
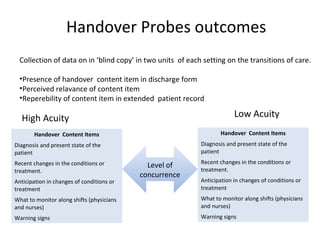
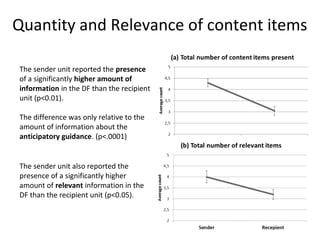
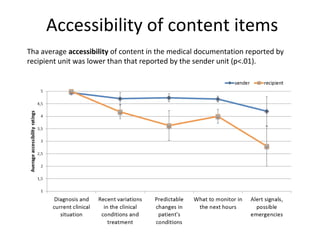
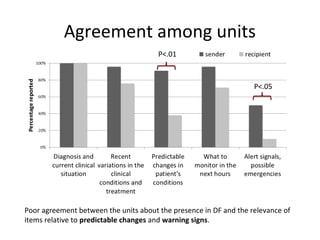
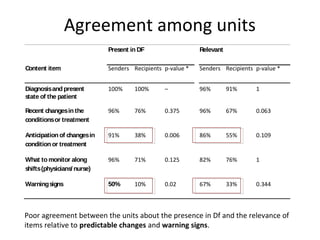

The document summarizes a study on handover processes between high acuity and low acuity care units. The study found poor agreement between units on the presence and relevance of information regarding anticipated changes to a patient's condition and warning signs. Sender units reported transmitting more overall information and anticipatory guidance than recipient units perceived receiving. The limited involvement of nursing staff in handovers may reduce the reliability of information transfer and contribute to adverse events. Further research is needed on improving common ground and information sharing between sender and recipient units.















































