- This document presents the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines for Thyroid Carcinoma.
- Version 3.2022 was published on November 1st, 2022 and includes updates to systemic therapy recommendations for papillary, follicular, and Hürthle cell carcinomas.
- The guidelines provide evidence-based recommendations for the evaluation, diagnosis and treatment of the main types of thyroid carcinoma.














![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Papillary Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
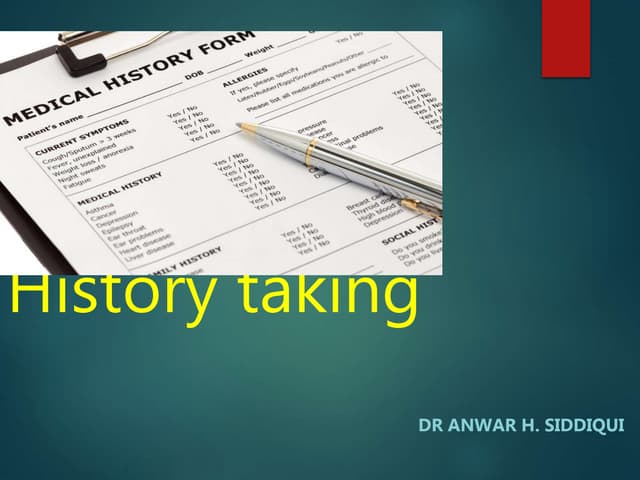
PAP‑8
• Rising or newly elevated Tg and
negative imaging
• Non‑resectable tumors
• Non‑radioiodine responsivez
Suppress TSH with levothyroxinej
Locoregional
recurrence
Surgery (preferred) if resectablebb
and
Consider Radioiodine treatment,aa if postoperative radioiodine imaging positive
or
Disease monitoring for non‑progressive disease that is stable and distant from
critical structures
or
For select patients with unresectable, non–radioiodine‑avid, and progressive disease,
consider:
EBRT (IMRT/stereotactic body radiation therapy [SBRT])n
and/or
Systemic therapies (Treatment of Metastatic Disease PAP‑9)
or
For select patients with limited burden nodal disease, consider local therapies when
available (ethanol ablation, radiofrequency ablation [RFA])
Metastatic disease
RAI therapy for iodine-avid diseasen
and/or
Local therapies when availablecc
and/or
If not amenable to RAI (Treatment of Metastatic Disease PAP‑9)
RECURRENT DISEASE
Continue surveillance with
unstimulated Tg,
ultrasound, and other imaging as
clinically indicated (PAP‑7)
• Progressively rising Tg (basal or stimulated)
• Scans (including PET) negative
Consider radioiodine therapy with ≥100 mCiaa
and
Post‑treatment iodine-131 imaging (category 3); additional RAI treatments should be
limited to patients who responded to previous RAI therapy (minimum of 6–12 months
between RAI treatments)
Consider preoperative
iodine total body scan
aa
The administered activity of RAI therapy should be adjusted
for pediatric patients. Principles of Radiation and RAI
Therapy (THYR-C).
bb Preoperative vocal cord assessment, if central neck
recurrence.
cc Ethanol ablation, cryoablation, RFA, etc.
j Principles of TSH Suppression (THYR‑A).
n Principles of Radiation and RAI Therapy (THYR-C).
z
Generally, a tumor is considered iodine‑responsive if follow‑up iodine-123 or low‑dose iodine-131 (1–3
mCi) whole body diagnostic imaging done 6–12 mo after iodine-131 treatment is negative or shows
decreasing uptake compared to pre‑treatment scans. It is recommended to use the same preparation
and imaging method used for the pre‑treatment scan and therapy. Favorable response to iodine-131
treatment is additionally assessed through change in volume of known iodine‑concentrated lesions by
CT/MRI, and by decreasing unstimulated or stimulated Tg levels.
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-17-320.jpg)
![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Papillary Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
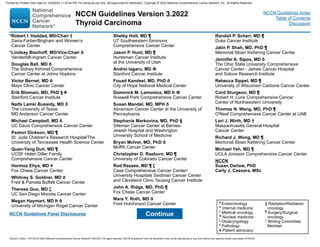
PAP‑9
CNS metastases
(PAP‑11)
TREATMENT OF LOCALLY RECURRENT, ADVANCED, AND/OR METASTATIC DISEASE NOT AMENABLE TO RAI THERAPY
j Principles of TSH Suppression (THYR‑A).
n Principles of Radiation and RAI Therapy (THYR-C).
cc Ethanol ablation, cryoablation, RFA, etc.
dd
Kinase inhibitor therapy may not be appropriate for patients with stable or slowly
progressive indolent disease. Principles of Kinase Inhibitor Therapy (THYR‑B).
ee
Commercially available small‑molecule kinase inhibitors (such as axitinib,
everolimus, pazopanib, sunitinib, vandetanib, vemurafenib [BRAF positive], or
dabrafenib [BRAF positive] [all are category 2A]) can be considered if clinical
trials are not available or appropriate.
ff
Cytotoxic chemotherapy has been shown to have minimal efficacy, although most
studies were small and underpowered.
Structurally
persistent/recurrent
locoregional or
distant metastatic
disease not
amenable to RAI
therapy
Bone
metastases
(PAP‑10)
Soft tissue
metastases
(eg, lung, liver,
muscle) excluding
central nervous
system (CNS)
metastases (see
below)
• Continue to
suppress TSH with
levothyroxinej
• For advanced,
progressive, or
threatening disease,
genomic testing to
identify actionable
mutations (including
ALK, NTRK, and
RET gene fusions),
DNA mismatch
repair (dMMR),
microsatellite
instability (MSI), and
tumor mutational
burden (TMB)
• Consider clinical trial
• Consider systemic therapy for progressive and/or symptomatic
disease
Preferred Regimens
◊ Lenvatinib (category 1)dd
Other Recommended Regimens
◊ Sorafenib (category 1)dd
Useful in Certain Circumstances
◊ Cabozantinib (category 1) if progression after lenvatinib and/
or sorafenib
◊ Larotrectinib or entrectinib for patients with NTRK gene
fusion-positive advanced solid tumors
◊ Selpercatinib or pralsetinib for patients with RET-fusion
positive tumors
◊ Pembrolizumab for patients with tumor mutational burden-
high (TMB-H) (≥10 mutations/megabase [mut/Mb]) tumors
◊ Dabrafenib/trametinib for patients with BRAF V600E mutation
that has progressed following prior treatment with no
satisfactory alternative treatment options
◊ Other therapies are available and can be considered for
progressive and/or symptomatic disease if clinical trials or
other systemic therapies are not available or appropriateee,ff
• Consider resection of distant metastases and/or EBRT (SBRT/
IMRTn/other local therapiescc when available to metastatic
lesions if progressive and/or symptomatic (Locoregional disease
PAP‑8)
• Disease monitoring is often appropriate in asymptomatic patients
with indolent disease assuming no brain metastasisdd (PAP‑7)
• Best supportive care, see the NCCN Guidelines for Palliative Care
Unresectable
locoregional
recurrent/
persistent disease
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-18-320.jpg)
![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Papillary Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
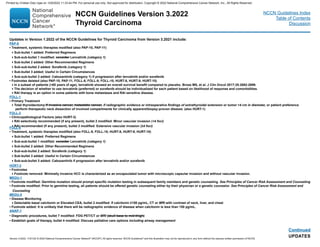
PAP‑10
• Consider surgical palliation and/or EBRT/SBRT/other local therapiescc when available if symptomatic, or asymptomatic in
weight‑bearing sites. Embolization prior to surgical resection of bone metastases should be considered to reduce the risk of
hemorrhage
• Consider embolization or other interventional procedures as alternatives to surgical resection/EBRT/IMRT in select cases
• Consider intravenous bisphosphonate or denosumabhh
• Disease monitoring may be appropriate in asymptomatic patients with indolent diseasedd (PAP‑7)
• Consider systemic therapy for progressive and/or symptomatic disease
Preferred Regimens
◊ Lenvatinib (category 1)dd
Other Recommended Regimens
◊ Sorafenib (category 1)dd
Useful in Certain Circumstances
◊ Cabozantinib (category 1) if progression after lenvatinib and/or sorafenib
◊ Larotrectinib or entrectinib for patients with NTRK gene fusion-positive advanced solid tumors
◊ Selpercatinib or pralsetinib for patients with RET-fusion positive tumors
◊ Pembrolizumab or patients with TMB-H (≥10 mut/Mb) tumors
◊ Dabrafenib/trametinib for patients with BRAF V600E mutation that has progressed following prior treatment with no
satisfactory alternative treatment options
◊ Other therapies are available and can be considered for progressive and/or symptomatic disease if clinical trials or other
systemic therapies are not available or appropriatedd,ee,ff
• Best supportive care, see the NCCN Guidelines for Palliative Care
Bone
metastases
TREATMENT OF METASTATIC DISEASE NOT AMENABLE TO RAI THERAPYgg
ccEthanol ablation, cryoablation, RFA, etc.
dd Kinase inhibitor therapy may not be appropriate for patients with stable or slowly progressive
indolent disease. Principles of Kinase Inhibitor Therapy (THYR‑B).
ee
Commercially available small‑molecule kinase inhibitors (such as axitinib, everolimus,
pazopanib, sunitinib, vandetanib, vemurafenib [BRAF positive], or dabrafenib [BRAF positive]
[all are category 2A]) can be considered if clinical trials are not available or appropriate.
ff Cytotoxic chemotherapy has been shown to have minimal efficacy, although most studies were
small and underpowered.
gg
RAI therapy is an option in some patients with bone metastases and RAI-sensitive disease.
hh
Denosumab and intravenous bisphosphonates can be associated with severe hypocalcemia;
patients with hypoparathyroidism and vitamin D deficiency are at increased risk of
hypocalcemia. Discontinuing denosumab can cause rebound atypical vertebral fractures.
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-19-320.jpg)
![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Papillary Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
PAP‑11
TREATMENT OF METASTATIC DISEASE NOT AMENABLE TO RAI THERAPYgg
• For solitary CNS lesions, either neurosurgical resection or stereotactic radiosurgeryn is preferred or
• For multiple CNS lesions, consider radiotherapy, including whole brain radiotherapy or stereotactic radiosurgery,n and/or
resection in select cases
and/or
• Consider systemic therapy for progressive and/or symptomatic disease
Preferred Regimens
◊ Lenvatinib (category 1) dd,ii,jj
Other Recommended Regimens
◊ Sorafenib (category 1) dd,ii,jj
Useful in Certain Circumstances
◊ Cabozantinib (category 1) if progression after lenvatinib and/or sorafenib
◊ Larotrectinib or entrectinib for patients with NTRK gene fusion-positive advanced solid tumors
◊ Selpercatinib or pralsetinib for patients with RET-fusion positive tumors
◊ Pembrolizumab for patients with TMB-H (≥10 mut/Mb) tumors
and/or
◊ Dabrafenib/trametinib for patients with BRAF V600E mutation that has progressed following prior treatment with no
satisfactory alternative treatment options
◊ Other therapies are available and can be considered for progressive and/or symptomatic disease if clinical trials or other
systemic therapies are not available or appropriatedd,ee,ff,hh
• Best supportive care, see the NCCN Guidelines for Palliative Care
CNS
metastases
n Principles of Radiation and RAI Therapy (THYR-C).
dd Kinase inhibitor therapy may not be appropriate for patients with stable or slowly progressive
indolent disease. Principles of Kinase Inhibitor Therapy (THYR‑B).
ee
Commercially available small‑molecule kinase inhibitors (such as axitinib, everolimus,
pazopanib, sunitinib, vandetanib, vemurafenib [BRAF positive], or dabrafenib [BRAF positive]
[all are category 2A]) can be considered if clinical trials are not available or appropriate.
ff Cytotoxic chemotherapy has been shown to have minimal efficacy, although most studies were
small and underpowered.
gg
RAI therapy is an option in some patients with bone metastases and RAI-sensitive disease.
hh
Denosumab and intravenous bisphosphonates can be associated with severe hypocalcemia;
patients with hypoparathyroidism and vitamin D deficiency are at increased risk of
hypocalcemia. Discontinuing denosumab can cause rebound atypical vertebral fractures.
ii
After consultation with neurosurgery and radiation oncology, data on the efficacy of lenvatinib or
sorafenib for patients with brain metastases have not been established.
jj
Tyrosine kinase inhibitor (TKI) therapy should be used with caution in otherwise untreated CNS
metastases due to bleeding risk.
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-20-320.jpg)





![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Follicular Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
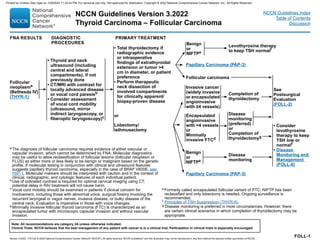
Unresectable
locoregional
recurrent/
persistent disease
CNS metastases
(FOLL‑10)
TREATMENT OF LOCALLY RECURRENT, ADVANCED, AND/OR METASTATIC DISEASE NOT AMENABLE TO RAI THERAPY
• Consider systemic therapy for progressive and/or symptomatic
disease
Preferred Regimens
◊ Lenvatinib (category 1)bb
Other Recommended Regimens
◊ Sorafenib (category 1)bb
Useful in Certain Circumstances
◊ Cabozantinib if progression after lenvatinib and/or sorafenib
◊ Larotrectinib or entrectinib for patients with NTRK gene
fusion-positive advanced solid tumors
◊ Selpercatinib or pralsetinib for patients with RET-fusion
positive tumors
◊ Pembrolizumab for patients with tumor mutational burden-
high (TMB-H) (≥10 mutations/megabase [mut/Mb]) tumors
◊ Dabrafenib/trametinib for patients with BRAF V600E mutation
that has progressed following prior treatment with no
satisfactory alternative treatment options
◊ Other therapies are available and can be considered for
progressive and/or symptomatic disease if clinical trials or
other systemic therapies are not available or appropriatecc,dd
• Consider resection of distant metastases and/or EBRT (SBRT/
IMRT)i/other local therapiesaa when available to metastatic
lesions if progressive and/or symptomatic. (Locoregional disease
FOLL‑7)
• Disease monitoring is often appropriate in asymptomatic patients
with indolent disease assuming no brain metastasis.dd (FOLL‑6)
• Best supportive care, see the See NCCN Guidelines for Palliative
Care
f See Principles of TSH Suppression (THYR‑A).
i See Principles of Radiation and RAI Therapy (THYR-C).
aa Ethanol ablation, cryoablation, RFA, etc.
bb
Kinase inhibitor therapy may not be appropriate for patients with stable or
slowly progressive indolent disease. See Principles of Kinase Inhibitor Therapy
(THYR‑B).
cc Commercially available small‑molecule kinase inhibitors (such as axitinib,
everolimus, pazopanib, sunitinib, vandetanib, vemurafenib [BRAF positive], or
dabrafenib [BRAF positive] [all are category 2A]) can be considered if clinical
trials are not available or appropriate.
dd Cytotoxic chemotherapy has been shown to have minimal efficacy, although
most studies were small and underpowered.
FOLL‑8
Structurally
persistent/recurrent
locoregional or
distant metastatic
disease not
amenable to RAI
therapy
Bone metastases
(FOLL‑9)
• Continue to
suppress TSH with
levothyroxinef
• For advanced,
progressive, or
threatening disease,
genomic testing to
identify actionable
mutations
(including ALK,
NTRK, and RET
gene fusions),
dMMR, MSI, and
TMB
• Consider clinical
trial
Soft tissue
metastases (eg,
lung, liver, muscle)
excluding CNS
metastases (see
below)
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-28-320.jpg)
![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Follicular Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
FOLL‑9
TREATMENT OF METASTATIC DISEASE NOT AMENABLE TO RAI THERAPYee
• Consider surgical palliation and/or EBRT/SBRT/other local therapiesaa when available if symptomatic, or asymptomatic in
weight‑bearing sites. Embolization prior to surgical resection of bone metastases should be considered to reduce the risk of
hemorrhage
• Consider embolization or other interventional procedures as alternatives to surgical resection/EBRT/IMRT in select casesi
• Consider intravenous bisphosphonate or denosumabff
• Disease monitoring may be appropriate in asymptomatic patients with indolent diseasebb (FOLL‑6)
• Consider systemic therapy for progressive and/or symptomatic disease
Preferred Regimens
◊ Lenvatinib (category 1)bb
Other Recommended Regimens
◊ Sorafenib (category 1)bb
Useful in Certain Circumstances
◊ Cabozantinib if progression after lenvatinib and/or sorafenib
◊ Larotrectinib or entrectinib for patients with NTRK gene fusion-positive advanced solid tumors
◊ Selpercatinib or pralsetinib for patients with RET-fusion positive tumors
◊ Pembrolizumab for patients with TMB-H (≥10 mut/Mb) tumors
◊ Dabrafenib/trametinib for patients with BRAF V600E mutation that has progressed following prior treatment with no
satisfactory alternative treatment options
◊ Other therapies are available and can be considered for progressive and/or symptomatic disease if clinical trials or other
systemic therapies are not available or appropriatebb,cc,dd
• Best supportive care, see the NCCN Guidelines for Palliative Care
Bone
metastases
i See Principles of Radiation and RAI Therapy (THYR-C).
aa Ethanol ablation, cryoablation, RFA, etc.
bb
Kinase inhibitor therapy may not be appropriate for patients with stable or
slowly progressive indolent disease. See Principles of Kinase Inhibitor Therapy
(THYR‑B).
cc
Commercially available small‑molecule kinase inhibitors (such as axitinib,
everolimus, pazopanib, sunitinib, vandetanib, vemurafenib [BRAF positive], or
dabrafenib [BRAF positive] [all are category 2A]) can be considered if clinical
trials are not available or appropriate.
dd
Cytotoxic chemotherapy has been shown to have minimal efficacy, although
most studies were small and underpowered.
ee
RAI therapy is an option in some patients with bone metastases and RAI-
sensitive disease.
ff
Denosumab and intravenous bisphosphonates can be associated with severe
hypocalcemia; patients with hypoparathyroidism and vitamin D deficiency are at
increased risk of hypocalcemia. Discontinuing denosumab can cause rebound
atypical vertebral fractures.
TREATMENT OF METASTATIC DISEASE NOT AMENABLE TO RAI THERAPYee
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-29-320.jpg)
![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Follicular Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
i Principles of Radiation and RAI Therapy (THYR-C).
aa Ethanol ablation, cryoablation, RFA, etc.
bb
Kinase inhibitor therapy may not be appropriate for patients with stable or slowly
progressive indolent disease. Principles of Kinase Inhibitor Therapy (THYR‑B).
cc
Commercially available small‑molecule kinase inhibitors (such as axitinib, everolimus,
pazopanib, sunitinib, vandetanib, vemurafenib [BRAF positive], or dabrafenib [BRAF
positive] [all are category 2A]) can be considered if clinical trials are not available or
appropriate.
dd
Cytotoxic chemotherapy has been shown to have minimal efficacy, although most studies
were small and underpowered.
ee
RAI therapy is an option in some patients with bone metastases and RAI-sensitive
disease.
ff
Denosumab and intravenous bisphosphonates can be associated with severe
hypocalcemia; patients with hypoparathyroidism and vitamin D deficiency are at increased
risk of hypocalcemia. Discontinuing denosumab can cause rebound atypical vertebral
fractures.
gg
After consultation with neurosurgery and radiation oncology; data on the efficacy of
lenvatinib or sorafenib for patients with brain metastases have not been established.
hh TKI therapy should be used with caution in otherwise untreated CNS metastases due to
bleeding risk.
FOLL‑10
CNS
metastases
• For solitary CNS lesions, either neurosurgical resection or stereotactic radiosurgery is preferred
or
• For multiple CNS lesions, consider radiotherapy,i including whole brain radiotherapy or stereotactic radiosurgery,i and/or
resection in select cases
and/or
• Consider systemic therapy for progressive and/or symptomatic disease
Preferred Regimens
◊ Lenvatinib (category 1)bb,gg,hh
Other Recommended Regimens
◊ Sorafenib (category 1) bb,gg,hh
Useful in Certain Circumstances
◊ Cabozantinib if progression after lenvatinib and/or sorafenib
◊ Larotrectinib or entrectinib for patients with NTRK gene fusion-positive advanced solid tumors
◊ Selpercatinib or pralsetinib for patients with RET-fusion positive tumors
◊ Pembrolizumab for patients with TMB-H (≥10 mut/Mb) tumors
and/or
◊ Dabrafenib/trametinib for patients with BRAF V600E mutation that has progressed following prior treatment with no
satisfactory alternative treatment options
◊ Other therapies are available and can be considered for progressive and/or symptomatic disease if clinical trials or
other systemic therapies are not available or appropriatebb,cc,dd,ff
• Best supportive care, see the NCCN Guidelines for Palliative Care
TREATMENT OF METASTATIC DISEASE NOT AMENABLE TO RAI THERAPYee
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-30-320.jpg)







![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Hürthle Cell Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
HÜRT‑8
Unresectable
locoregional
recurrent/
persistent disease
Soft tissue
metastases
(eg, lung, liver,
muscle) excluding
CNS metastases
(see below)
CNS
metastases
(HÜRT‑10)
TREATMENT OF LOCALLY RECURRENT, ADVANCED, AND/OR METASTATIC DISEASE NOT AMENABLE TO RAI THERAPY
• Consider systemic therapy for progressive and/or symptomatic
disease
Preferred Regimens
◊ Lenvatinib (category 1)cc
Other Recommended Regimens
◊ Sorafenib (category 1)cc
Useful in Certain Circumstances
◊ Cabozantinib if progression after lenvatinib and/or sorafenib
◊ Larotrectinib or entrectinib for patients with NTRK gene
fusion-positive advanced solid tumors
◊ Selpercatinib or pralsetinib for patients with RET-fusion
positive tumors
◊ Pembrolizumab for patients with TMB-H (≥10 mut/Mb) tumors
◊ Dabrafenib/trametinib for patients with BRAF V600E mutation
that has progressed following prior treatment with no
satisfactory alternative treatment options
◊ Other therapies are available and can be considered for
progressive and/or symptomatic disease if clinical trials or
other systemic therapies are not available or appropriatedd,ee
• Consider resection of distant metastases and/or EBRT (SBRT/
IMRT)j/other local therapiesbb when available to metastatic
lesions if progressive and/or symptomatic (Locoregional disease,
HÜRT‑7)
• Disease monitoring is often appropriate in asymptomatic patients
with indolent disease assuming no brain metastasiscc (HÜRT‑6)
• Best supportive care, see the NCCN Guidelines for Palliative Care
f Principles of TSH Suppression (THYR‑A).
j Principles of Radiation and RAI Therapy (THYR-C).
bb Ethanol ablation, cryoablation, RFA, etc.
cc
Kinase inhibitor therapy may not be approriate for patients with stable or slowly
progressive indolent disease. Principles of Kinase Inhibitor Therapy (THYR‑B).
dd
Commercially available small‑molecule kinase inhibitors (such as axitinib,
everolimus, pazopanib, sunitinib, vandetanib, vemurafenib [BRAF positive], or
dabrafenib [BRAF positive] [all are category 2A]) can be considered if clinical
trials are not available or appropriate.
ee
Cytotoxic chemotherapy has been shown to have minimal efficacy, although
most studies were small and underpowered.
Structurally
persistent/
recurrent
locoregional
or distant
metastatic
disease not
amenable to
RAI therapy
Bone metastases
(HÜRT‑9)
• Continue to
suppress
TSH with
levothyroxinef
• For advanced,
progressive,
or threatening
disease, genomic
testing to identify
actionable
mutations
(including ALK,
NTRK, and RET
gene fusions),
dMMR, MSI, and
TMB
• Consider clinical
trial
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-38-320.jpg)
![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Hürthle Cell Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
• Consider surgical palliation and/or EBRT/SBRT/other local therapiesbb when available if symptomatic, or asymptomatic in
weight‑bearing sites. Embolization prior to surgical resection of bone metastases should be considered to reduce the risk of
hemorrhage
• Consider embolization or other interventional procedures as alternatives to surgical resection/EBRT/IMRT in select casesj
• Consider intravenous bisphosphonate or denosumabgg
• Disease monitoring may be appropriate in asymptomatic patients with indolent diseaseee (HÜRT‑6)
• Consider systemic therapy for progressive and/or symptomatic disease
Preferred Regimens
◊ Lenvatinib (category 1)cc
Other Recommended Regimens
◊ Sorafenib (category 1)cc
Useful in Certain Circumstances
◊ Cabozantinib if progression after lenvatinib and/or sorafenib
◊ Larotrectinib or entrectinib for patients with NTRK gene fusion-positive advanced solid tumors
◊ Selpercatinib or pralsetinib for patients with RET-fusion positive tumors
◊ Pembrolizumab for patients with TMB-H (≥10 mut/Mb) tumors
◊ Dabrafenib/trametinib for patients with BRAF V600E mutation that has progressed following prior treatment with no
satisfactory alternative treatment options
◊ Other therapies are available and can be considered for progressive and/or symptomatic disease if clinical trials or other
systemic therapies are not available or appropriatecc,dd,ee
• Best supportive care, see the NCCN Guidelines for Palliative Care
Bone
metastases
TREATMENT OF METASTATIC DISEASE NOT AMENABLE TO RAI THERAPYff
HÜRT‑9
j Principles of Radiation and RAI Therapy (THYR-C).
bb Ethanol ablation, cryoablation, RFA, etc.
cc
Kinase inhibitor therapy may not be appropriate for patients with stable or slowly
progressive indolent disease. Principles of Kinase Inhibitor Therapy (THYR‑B).
dd Commercially available small‑molecule kinase inhibitors (such as axitinib,
everolimus, pazopanib, sunitinib, vandetanib, vemurafenib [BRAF positive], or
dabrafenib [BRAF positive] [all are category 2A]) can be considered if clinical
trials are not available or appropriate.
ee
Cytotoxic chemotherapy has been shown to have minimal efficacy, although
most studies were small and underpowered.
ff
RAI therapy is an option in some patients with bone metastases and RAI-sensitive
disease.
gg
Denosumab and intravenous bisphosphonates can be associated with severe
hypocalcemia; patients with hypoparathyroidism and vitamin D deficiency are at
increased risk of hypocalcemia. Discontinuing denosumab can cause rebound
atypical vertebral fractures.
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-39-320.jpg)
![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Hürthle Cell Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
• For solitary CNS lesions, either neurosurgical resection or stereotactic radiosurgeryj is preferred
or
• For multiple CNS lesions, consider radiotherapy,j including whole brain radiotherapyj or stereotactic radiosurgery,j and/or
resection in select cases
• Consider systemic therapy For progressive and/or symptomatic disease
Preferred Regimens
◊ Lenvatinib (category 1)cc,hh,ii
Other
◊ Sorafenib (category 1) cc,hh,ii
Useful in Certain Circumstances
◊ Cabozantinib if progression after lenvatinib and/or sorafenib
◊ Larotrectinib or entrectinib for patients with NTRK gene fusion-positive advanced solid tumors
◊ Selpercatinib or pralsetinib for patients with RET-fusion positive tumors
◊ Pembrolizumab for patients with TMB-H (≥10 mut/Mb) tumors
and/or
◊ Dabrafenib/trametinib for patients with BRAF V600E mutation that has progressed following prior treatment with no
satisfactory alternative treatment options
◊ Other therapies are available and can be considered for progressive and/or symptomatic disease if clinical trials or other
systemic therapies are not available or appropriatecc,dd,ee,gg
• Best supportive care, see the NCCN Guidelines for Palliative Care
CNS
metastases
TREATMENT OF METASTATIC DISEASE NOT AMENABLE TO RAI THERAPYdd
j Principles of Radiation and RAI Therapy (THYR-C).
bb Ethanol ablation, cryoablation, RFA, etc.
cc
Kinase inhibitor therapy may not be appropriate for patients with stable or slowly
progressive indolent disease. Principles of Kinase Inhibitor Therapy (THYR‑B).
dd Commercially available small‑molecule kinase inhibitors (such as axitinib,
everolimus, pazopanib, sunitinib, vandetanib, vemurafenib [BRAF positive], or
dabrafenib [BRAF positive] [all are category 2A]) can be considered if clinical
trials are not available or appropriate.
ee
Cytotoxic chemotherapy has been shown to have minimal efficacy, although
most studies were small and underpowered.
gg
Denosumab and intravenous bisphosphonates can be associated with severe
hypocalcemia; patients with hypoparathyroidism and vitamin D deficiency are at
increased risk of hypocalcemia. Discontinuing denosumab can cause rebound
atypical vertebral fractures.
hh
After consultation with neurosurgery and radiation oncology; data on the efficacy
of lenvatinib or sorafenib for patients with brain metastases have not been
established.
ii
TKI therapy should be used with caution in otherwise untreated CNS metastases
due to bleeding risk.
HÜRT‑10
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-40-320.jpg)




![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Medullary Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
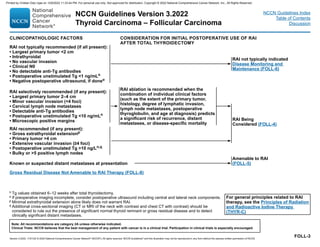
MEDU‑6
RECURRENT OR PERSISTENT
LOCOREGIONAL DISEASE
Locoregional
Recurrent or
Persistent Disease;
Distant Metastases
(MEDU‑7)
s Increasing tumor markers, in the absence of structural disease progression, are not an indication for treatment with systemic therapy.
t Kinase inhibitor therapy may not be appropriate for patients with stable or slowly progressive indolent disease. Principles of Kinase Inhibitor Therapy in Advanced
Thyroid Carcinoma (THYR‑B).
u Treatment with systemic therapy is not recommended for increasing calcitonin/CEA alone.
v Only health care professionals and pharmacies certified through the vandetanib Risk Evaluation and Mitigation Strategy (REMS) program, a restricted distribution
program, will be able to prescribe and dispense the drug.
w Genomic testing including TMB or RET somatic genotyping in patients who are germline wild-type or germline unknown.
TREATMENT
• Surgical resection is the preferred treatment modality
• EBRT/IMRT can be considered for unresectable disease
or, less commonly, after surgical resection
• Consider systemic therapys for unresectable disease
that is symptomatic or progressing by RECIST criteriat,u
Preferred Regimens
◊ Vandetanibv (category 1)
◊ Cabozantinib (category 1)
◊ Selpercatinib (RET mutation-positive)w
◊ Pralsetinib (RET mutation-positive)w
Useful in Certain Circumstances
◊ Pembrolizumab (TMB-H [≥10 mut/Mb])w
• Disease monitoring
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-46-320.jpg)
![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Medullary Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
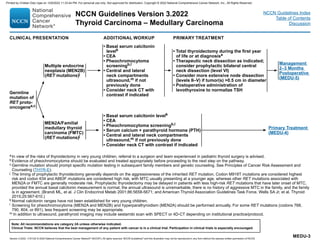
MEDU‑7
RECURRENT OR PERSISTENT DISEASE
DISTANT METASTASES
Asymptomatic
disease
Symptomatic disease
or
Progressiont
• Systemic therapy or clinical trial
Preferred Regimens
◊ Vandetanib (category 1)x
◊ Cabozantinib (category 1)x
◊ Selpercatinib (RET mutation-positive)w
◊ Pralsetinib (RET mutation-positive)w
Other Recommended Regimens
◊ Consider other small‑molecule kinase inhibitorsy
◊ Dacarbazine (DTIC)‑based chemotherapyz
Useful in Certain Circumstances
◊ Pembrolizumab (TMB-H [≥10 mut/Mb])w
• EBRT/IMRT for local symptoms
• Consider intravenous bisphosphonate or denosumabaa therapy for bone
metastases
• Consider palliative resection, ablation (eg, RFA, embolization,
other regional therapy), or other regional treatment
• Best supportive care, see the NCCN Guidelines for Palliative Care
Progressive disease,
see pathway below
sIncreasing tumor markers, in the absence of structural disease progression, are not an indication for
treatment with systemic therapy.
t Kinase inhibitor therapy may not be appropriate for patients with stable or slowly progressive indolent
disease. Principles of Kinase Inhibitor Therapy in Advanced Thyroid Carcinoma (THYR‑B).
uTreatment with systemic therapy is not recommended for increasing calcitonin/CEA alone.
v Only health care professionals and pharmacies certified through the vandetanib Risk Evaluation and
Mitigation Strategy (REMS) program, a restricted distribution program, will be able to prescribe and
dispense the drug.
wGenomic testing including TMB or RET somatic genotyping in patients who are germline wild-type or
germline unknown.
xClinical benefit can be seen in both sporadic and familial MTC.
y
While not FDA-approved for treatment of medullary thyroid cancer, other commercially available
small‑molecule kinase inhibitors (such as sorafenib, sunitinib, lenvatinib, or pazopanib) can be
considered if clinical trials or preferred systemic therapy options are not available or appropriate, or if
the patient progresses on preferred systemic therapy options.
zDoxorubicin/streptozocin alternating with fluorouracil/dacarbazine or fluorouracil/dacarbazine
alternating with fluorouracil/streptozocin.
aaDenosumab and intravenous bisphosphonates can be associated with severe hypocalcemia; patients
with hypoparathyroidism and vitamin D deficiency are at increased risk.
• Disease monitoring
• Consider resection (if possible), ablation (eg, RFA, embolization, other
regional therapy)
• Systemic therapys if not resectable and progressing by RECIST criteriat,u
Preferred Regimens
◊ Vandetanibt,v (category 1)
◊ Cabozantinib (category 1)
◊ Selpercatinib (RET mutation-positive)w
◊ Pralsetinib (RET mutation-positive)w
Useful in Certain Circumstances
◊ Pembrolizumab (TMB-H [≥10 mut/Mb])w
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-47-320.jpg)

![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Anaplastic Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
STAGEd
R0/R1 resectione
achieved (usually
as incidentally
discovered, very
small ATC)
Adjuvant EBRT/IMRTf
with radiosensitizing
chemotherapyg when
clinically appropriate
EBRT/IMRTf with chemotherapyg
when clinically appropriate
or
Consider molecularly targeted
neoadjuvant therapyh for borderline
resectable disease when safe to do so
Surgery can be
reconsidered after
neoadjuvant therapy
depending on
response
Stage IVA or IVBa,c
(locoregional
disease)
Total thyroidectomy
with therapeutic lymph
node dissection
Resectable
Unresectablee
a Consider core or open biopsy if FNA is “suspicious” for ATC or is not definitive. Morphologic diagnosis combined with immunohistochemistry is necessary to exclude
other entities such as poorly differentiated thyroid cancer, medullary thyroid cancer, squamous cell carcinoma, and lymphoma.
c Preoperative evaluations need to be completed as quickly as possible and involve integrated decision-making in a multidisciplinary team and with the patient. Consider
referral to multidisciplinary high‑volume center with expertise in treating ATC.
d Staging (ST‑1).
e Resectability for locoregional disease depends on extent of involved structures, potential morbidity, and mortality associated with resection. In most cases, there is no
indication for a debulking surgery. Staging (ST‑1) for definitions of R0/R1/R2.
f Principles of Radiation and RAI Therapy (THYR-C).
g Adjuvant/Radiosensitizing Chemotherapy Regimens for Anaplastic Thyroid Carcinoma (ANAP‑A [1 of 3]).
h Regimens that may be used for neoadjuvant therapy include dabrafenib/trametinib for BRAF V600E mutations; selpercatinib or pralsetinib for RET-fusion positive
tumors; and larotrectinib or entrectinib for patients with NTRK gene fusion-positive tumors.
TREATMENT
Incomplete
(R2 resection)
ANAP‑2
Disease
Monitoring
and Management
(ANAP-3)
EBRT/IMRTf with
chemotherapyg when
clinically appropriate
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-49-320.jpg)
![Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Anaplastic Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
ANAP‑3
b Molecular testing should include BRAF, NTRK, ALK, RET, MSI, dMMR, and tumor mutational burden.
d Staging (ST‑1).
i Consider dabrafenib/trametinib if BRAF V600E mutation positive (Subbiah V, et al. J Clin Oncol 2018;36:7‑13); larotrectinib or entrectinib if NTRK gene fusion positive
(Drilon A, et al. N Engl J Med 2018;378:731‑739; Doebele RC, et al. Lancet Oncol 2020;21:271-282); selpercatinib or pralsetinib if RET fusion positive (Wirth L,
et al. Presented at the Annual Meeting of the European Society for Medical Oncology in Barcelona, Spain; September 27-October 1, 2019. Oral presentation.); or
pembrolizumab for TMB-H (Marabelle A, et al. Presented at the Annual Meeting of ESMO in Barcelona, Spain; September 30, 2019).
j Consider use of intravenous bisphosphonates or denosumab. Denosumab and intravenous bisphosphonates can be associated with severe hypocalcemia; patients
with hypoparathyroidism and vitamin D deficiency are at increased risk.
k Systemic Therapy Regimens for Metastatic Disease (ANAP-A [2 of 3]).
DISEASE MONITORING AND MANAGEMENT
• Cross‑sectional imaging
(CT or MRI with contrast)
of brain, neck, chest,
abdomen, and pelvis
at frequent intervals as
clinically indicated
• Consider FDG PET/CT 3–6
months after initial therapy
• Continued disease
monitoring if no
evidence of disease
(NED)
• Palliative locoregional
radiation therapy
• Local lesion control (eg,
bone,j brain metastases)
• Second‑line systemic
therapyk or clinical trial
• Best supportive
care, see the NCCN
Guidelines for Palliative
Care
Stage IVCd
Aggressive
therapy
Palliative
care
• Total thyroidectomy with therapeutic
lymph node dissection if resectable
(R0/R1)
• Consider tracheostomy
• Locoregional radiation therapy
• Systemic therapy (See ANAP‑A [2 of 3])
• Molecular testing for actionable
mutationsi if not previously doneb
• Consider clinical trial
• Palliative locoregional radiation
therapy
• Local lesion control with surgery or
radiation (eg, bone,j brain metastases)
• Consider tracheostomy
• NCCN Guidelines for Central Nervous
System Cancers
• Best supportive care
METASTATIC
DISEASE
TREATMENT
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-50-320.jpg)

![Paclitaxel8
60–90 mg/m² IV
or
135–200 mg/m²
Weekly
Every 3–4 weeks
Doxorubicin8
20 mg/m² IV
or
60–75 mg/m² IV
Weekly
Every 3 weeks
Paclitaxel/carboplatin1 (category 2B)
Paclitaxel 60–100 mg/m2
, carboplatin AUC 2 IV
or
Paclitaxel 135–175 mg/m2
, carboplatin AUC 5–6 IV
Weekly
Every 3–4 weeks
Docetaxel/doxorubicin1 (category 2B)
Docetaxel 60 mg/m2
IV, doxorubicin 60 mg/m2
IV (with pegfilgrastim)
or
Docetaxel 20 mg/m2
IV, doxorubicin 20 mg/m2
IV
Every 3–4 weeks
Weekly
Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma – Anaplastic Carcinoma
NCCN Guidelines Index
Table of Contents
Discussion
ANAP‑A
2 OF 3
SYSTEMIC THERAPY
Systemic Therapy Regimens for Metastatic Disease
Preferred Regimens
Dabrafenib/trametinib2
(BRAF V600E mutation positive)
Dabrafenib 150 mg PO
and
Trametinib 2 mg PO
Twice daily
Once daily
Larotrectinib3
(NTRK gene fusion positive) 100 mg PO Twice daily
Entrectinib4
(NTRK gene fusion positive) 600 mg PO Once daily
Pralsetinib5
(RET fusion positive) 400 mg PO Once daily
Selpercatinib6
(RET fusion positive)
120 mg PO (50 kg)
or
160 mg PO (≥50 kg)
Twice daily
Other Recommended Regimens
Useful in Certain Circumstances
Doxorubicin/cisplatin8 Doxorubicin 60 mg/m² IV, cisplatin 40 mg/m² IV Every 3 weeks
Pembrolizumab7
(TMB-H [≥10 mut/Mb])
200 mg IV
or
400 mg IV
Every 3 weeks
Every 6 weeks
References
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-52-320.jpg)




![NCCN Guidelines Version 3.2022
Thyroid Carcinoma
Version 3.2022, 11/01/22 © 2022 National Comprehensive Cancer Network®
(NCCN®
), All rights reserved. NCCN Guidelines®
and this illustration may not be reproduced in any form without the express written permission of NCCN.
Note: All recommendations are category 2A unless otherwise indicated.
Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
NCCN Guidelines Index
Table of Contents
Discussion
THYR‑C
2 OF 5
PRINCIPLES OF RADIATION AND RADIOACTIVE IODINE THERAPY
IODINE-131 ADMINISTRATION
Administered Activity
See special circumstances below for pediatric dose adjustment.
• Remnant ablation:
30–50 mCi
◊ If RAI ablation is used in T1b/T2 (1–4 cm), clinical N0 disease, in
the absence of other adverse pathologic, laboratory, or imaging
features, 30–50 mCi of iodine-131 is recommended (category 1)
following either thyrotropin alfa stimulation or thyroid hormone
withdrawal. This dose of 30–50 mCi may also be considered
(category 2B) for patients with T1b/T2 (1–4 cm) with small-
volume N1a disease (fewer than 5 lymph node metastases 2
mm in diameter) and for patients with primary tumors 4 cm,
clinical M0 with minor extrathyroidal extension.4,5
• Adjuvant therapy:
50–150 mCi
◊ For higher likelihood of residual disease based on operative
pathology or pretherapy radioiodine scan
• Treatment of known disease
100–200 mCi
◊ For proven unresectable or metastatic disease based on
pathology or pretherapy radioiodine scan
Dosimetry can be used to determine maximal dose at high-volume
centers for documented nonresectable, large-volume, iodine-
concentrating, residual, or recurrent disease. Generally, the
maximum 48-hour whole-body dose should not exceed ~80 mCi to
avoid pulmonary fibrosis in the case of diffuse lung metastases,
and the bone marrow retention maximum should not exceed ~120
mCi at 48 hours.1
Special Circumstances
• Pediatric patients:
Chest imaging using non-contrast CT prior to treatment to assess
for lung metastases
Weight-based dose adjustment for pediatric patients assuming
routine dosing for 70 kg adult (ie, a 150 mCi dose for a 70 kg adult
would translate to 2.15 mCi/kg for the pediatric patient)6
Special Circumstances
• RAI after imaging study or procedure using iodine contrast agent:
Wait 2 months to allow for free iodine levels to decrease (100
mcg/24 hours) and allow for optimal RAI uptake7,8
Consider measurement of 24-hour urine iodine to confirm a normal
free iodine prior to preparing for dosing.
• Breastfeeding patients:
Wait 3–6 months after cessation of lactation or with normalization
of serum prolactin levels.
Complete cessation of breastfeeding after iodine-123 or iodine-131
administration for the current infant. There should be no increased
risk to mother or infant for breastfeeding with subsequent births
assuming no radioiodine is administered around the subsequent
birth/breastfeeding period.9
• Decreased glomerular filtration rate (GFR)/end-stage renal disease
(ESRD)/hemodialysis:
Special consideration to administered dose, and timing with
respect to dialysis to maximize therapeutic effect and minimize
non-thyroid uptake/exposure10
Multidisciplinary involvement including close monitoring by
radiation safety to coordinate administration, monitoring, and
minimization of exposure to others
• Patients desiring pregnancy
Patients should be counseled to wait at least 6 months after
iodine-131 therapy to attempt pregnancy to avoid adverse
pregnancy outcomes (such as fetal hypothyroidism, malformation,
increased malignancy risk in the child, or fetal demise [with
high doses]) related to RAI. For many patients a longer interval
before attempting pregnancy may be recommended to confirm
disease-free status at 6–12 months post-RAI. In these cases,
earlier pregnancy is inadvisable as it would interfere with disease
detection and further management.
In selective cases when doses are high or other considerations
are present, integrating care with reproductive endocrinology/
oncofertility for men and women may be appropriate.
References
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-57-320.jpg)












![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-5
System for Reporting Thyroid Cytopathology.61
As of the 2021 update to
the NCCN Guidelines for Thyroid Carcinoma, management
recommendations are no longer provided for nodules classified as
Bethesda I and Bethesda II. Pathology and cytopathology slides should be
reviewed at the treating institution by a pathologist with expertise in the
diagnosis of thyroid disorders. Although FNA is a very sensitive test—
particularly for papillary carcinoma—false-negative results are sometimes
obtained; therefore, a reassuring FNA should not override worrisome
clinical or radiographic findings.62,63
Molecular diagnostic testing to detect individual mutations (eg, BRAF
V600E, RET/PTC, RAS, PAX8/PPAR [peroxisome proliferator-activated
receptor] gamma) or pattern recognition approaches using molecular
classifiers may be useful in the evaluation of FNA samples that are
indeterminate to assist in management decisions.64-72
The BRAF V600E
mutation occurs in about 45% of patients with papillary carcinoma and is
the most common mutation.73
Some studies have linked the BRAF V600E
mutation to poor prognosis, especially when occurring with TERT
promoter mutation.74-77
The choice of the precise molecular test depends
on the cytology and the clinical question being asked.78-81
Indeterminate
groups include: 1) follicular or Hürthle cell neoplasms (Bethesda IV); and
2) AUS/FLUS (Bethesda III).82-84
The NCCN Panel recommends
consideration of molecular diagnostic testing for these indeterminate
groups.85,86
Historically, studies have shown that molecular diagnostics do not perform
well for Hürthle cell neoplasms.83,87,88
More recently, modern genomic
classifiers have shown promise for diagnosis of Hürthle cell-containing
specimens, with sensitivity values ranging from 88.9% to 92.9% and
specificity values ranging from 58.8% to 69.3% for detecting Hürthle cell
cancers.89,90
Molecular diagnostic testing may include multigene assays or
individual mutational analysis. In addition to their utility in diagnostics,
molecular markers are beneficial for making decisions about targeted
therapy options for advanced disease and for informing eligibility for some
clinical trials. In addition, the presence of some mutations may have
prognostic importance.
A minority of panelists expressed concern regarding active nodule
surveillance of follicular lesions because they were perceived as
potentially pre-malignant lesions with a very low, but unknown, malignant
potential if not surgically resected (leading to recommendations for either
nodule surveillance or considering lobectomy in lesions classified as
benign by molecular testing). Clinical risk factors, sonographic patterns,
and patient preference can help determine whether nodule surveillance or
surgery is appropriate for these patients. Guidance regarding nodule
surveillance from the ATA and the ACR TI-RADS should be followed.3,59
A
systematic review including 27 studies that evaluated repeat FNA in
AUS/FLUS nodules showed that 48% (95% CI, 43%–54%) of nodules
were reclassified as benign, with a negative predictive value (NPV) greater
than 96%.91
FNA may be repeated for AUS/FLUS, especially if molecular
diagnostics are technically inadequate.
Rather than proceeding to immediate surgical resection to obtain a
definitive diagnosis for these indeterminate FNA cytology groups (follicular
lesions), patients can be followed with nodule surveillance if the
application of a specific molecular diagnostic test (in conjunction with
clinical and ultrasound features) results in a predicted risk of malignancy
that is comparable to the rate seen in cytologically benign thyroid FNAs
(approximately ≤5%). It is important to note that the predictive value of
molecular diagnostics may be significantly influenced by the pre-test
probability of disease associated with the various FNA cytology groups.
Furthermore, in the cytologically indeterminate groups, the risk of
malignancy from FNA can vary widely between institutions.61,92
Because
the published studies have focused primarily on adult patients with thyroid
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-71-320.jpg)


![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-8
with thyroid carcinoma—especially those who are older than 40 years—
may be regarded with special concern.121
Familial Syndromes
Familial, non-medullary carcinoma accounts for about 5% of PTCs and, in
some cases, may be clinically more aggressive than the sporadic
form.122,123
For patients to be considered as having familial papillary
carcinoma, most studies require at least three first-degree relatives to be
diagnosed with papillary carcinoma because the finding of cancer in a
single first-degree relative may just be a chance event. Microscopic
familial papillary carcinoma tends to be multifocal and bilateral, often with
vascular invasion, lymph node metastases, and high rates of recurrence
and distant metastases.124
Other familial syndromes associated with
papillary carcinoma are familial adenomatous polyposis,125
Carney
complex (multiple neoplasia and lentiginosis syndrome, which affects
endocrine glands),126
and Cowden syndrome (multiple hamartomas).127
The prognosis for patients with all of these syndromes is not different from
the prognosis of those with spontaneously occurring papillary carcinoma.
Tumor Variables Affecting Prognosis
Some tumor features have a profound influence on prognosis.111,128-130
The
most important features are tumor histology, primary tumor size, local
invasion, necrosis, vascular invasion, BRAF V600E mutation status, and
metastases.74,131,132
For example, vascular invasion (even within the
thyroid gland) is associated with more aggressive disease and with a
higher incidence of recurrence.133-136
The CAP protocol provides
definitions of vascular invasion and other terms (see Protocol for the
Examination of Specimens From Patients With Carcinomas of the Thyroid
Gland on the CAP website).96
In patients with sporadic medullary
carcinoma, a somatic RET oncogene mutation confers an adverse
prognosis.137
A meta-analysis including 13 studies showed that PD-L1
expression is associated with lower disease-free survival (DFS) (hazard
ratio [HR], 3.37; 95% CI, 2.54–4.48; P .00001) and overall survival (OS)
(HR, 2.52; 95% CI, 1.20–5.32; P = .01) in patients with thyroid cancer.138
Another meta-analysis including 15 studies also showed a significant
association between PD-L1 expression and lower DFS (HR, 1.90; 95% CI,
1.33–2.70; P .001), but OS was not significantly associated with PD-L1
expression.139
Subgroup analyses showed that the association between
PD-L1 expression and DFS was significant for papillary carcinoma (HR,
2.18; 95% CI, 1.08–4.39), but not for poorly differentiated or anaplastic
thyroid carcinoma (HR, 1.63; 95% CI, 0.62–4.32).
Histology
Although survival rates with typical papillary carcinoma are quite good,
cancer-specific mortality rates vary considerably with certain histologic
subsets of tumors.1
A well-defined tumor capsule, which is found in about
10% of PTCs, is a particularly favorable prognostic indicator. A worse
prognosis is associated with anaplastic tumor transformation; tall-cell
papillary variants, which have a 10-year mortality of up to 25%; columnar
variant papillary carcinoma (a rapidly growing tumor with a high mortality
rate); hobnail variant papillary carcinoma, which is associated with
increased rates of local and distant metastasis; and diffuse sclerosing
variants, which infiltrate the entire gland.37,140-142
NIFTP, formerly known as noninvasive encapsulated follicular variant of
papillary thyroid carcinoma (EFVPTC), is characterized by its follicular
growth pattern, encapsulation or clear demarcation of the tumor from
adjacent tissue with no invasion, and nuclear features of papillary
carcinoma.143,144
NIFTP tumors have a low risk for adverse outcomes and,
therefore, require less aggressive treatment.144-148
NIFTP was re-classified
in 2016 to prevent overtreatment of this indolent tumor type as well as the
psychological consequences of a cancer diagnosis on the patient.143,144
A
systematic review including 29 studies showed that the pooled prevalence
rates of NIFTP within EFVPTC and PTC were 43.5% (95% CI, 33.5%–
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-74-320.jpg)




![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-13
However, some prominent thyroid cancer specialists (including some at
NCCN Member Institutions) oppose this view and advocate unilateral
lobectomy for most patients with papillary and follicular carcinoma based
on 1) the low mortality among most patients (ie, those patients categorized
as low risk by the AMES and other prognostic classification schemes); and
2) the high complication rates reported with more extensive
thyroidectomy.117,191,207
The large thyroid remnant remaining after
unilateral lobectomy, however, may complicate long-term follow-up with
serum Tg determinations and whole body iodine-131 imaging. Panel
members recommend total lobectomy (without RAI ablation) for patients
with papillary carcinoma who have incidental small-volume pathologic N1A
metastases (5 involved nodes with no metastasis 5 mm, in largest
dimension).208
NCCN Panel Members believe that lobectomy alone is adequate
treatment for papillary microcarcinomas provided the patient has not been
exposed to radiation, has no other risk factors, and has a tumor 1 cm or
smaller that is unifocal and confined to the thyroid without vascular
invasion (see Primary Treatment in the NCCN Guidelines for Papillary
[Thyroid] Carcinoma).3,209-212
Total lobectomy alone is also adequate
treatment for NIFTP pathologies (see Tumor Variables Affecting
Prognosis, Histology) and minimally invasive follicular thyroid carcinomas
(see Primary Treatment in the NCCN Guidelines for Follicular [Thyroid]
Carcinoma). However, completion thyroidectomy is recommended for any
of the following: tumor larger than 4 cm in diameter, positive resection
margins, gross extrathyroidal extension, macroscopic multifocal disease
(ie, 1 cm), macroscopic nodal metastases, confirmed contralateral
disease, or vascular invasion.3
Note that “gross extrathyroidal extension”
refers to spread of the primary tumor outside of the thyroid capsule with
invasion into the surrounding structures such as strap muscles, trachea,
larynx, vasculature, esophagus, and/or recurrent laryngeal nerve.131,213,214
Completion Thyroidectomy
This procedure is recommended when remnant ablation is anticipated or if
long-term follow-up is planned with serum Tg determinations and with (or
without) whole body iodine-131 imaging. Large thyroid remnants are
difficult to ablate with iodine-131.206
Completion thyroidectomy has a
complication rate similar to that of total thyroidectomy. Some experts
recommend completion thyroidectomy for routine treatment of tumors 1
cm or larger, because approximately 50% of patients with cancers of this
size have additional cancer in the contralateral thyroid lobe.174,215-221
In
patients with local or distant tumor recurrence after lobectomy, cancer is
found in more than 60% of the resected contralateral lobes.218
Miccoli et al studied irradiated children from Chernobyl who developed
thyroid carcinoma and were treated by lobectomy; they found that 61%
had unrecognized lung or lymph node metastases that could only be
identified after completion thyroidectomy.120
In another study, patients who
underwent completion thyroidectomy within 6 months of their primary
operation developed significantly fewer lymph node and hematogenous
recurrences, and they survived significantly longer than did those in whom
the second operation was delayed for more than 6 months.219
Surgical Complications
The most common significant complications of thyroidectomy are
hypoparathyroidism and recurrent laryngeal nerve injury, which occur
more frequently after total thyroidectomy.222
Transient clinical
hypoparathyroidism postoperatively is common in adults223
and
children120,224
undergoing total thyroidectomy. The rates of long-term
recurrent laryngeal nerve injury and hypoparathyroidism, respectively,
were 3% and 2.6% after total thyroidectomy and 1.9% and 0.2% after
subtotal thyroidectomy.225
One study reported hypocalcemia in 5.4% of
patients immediately after total thyroidectomy, persisting in only 0.5% of
patients 1 year later.226
Another study reported a 3.4% incidence of
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-79-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-14
long-term recurrent laryngeal nerve injury and a 1.1% incidence of
permanent hypocalcemia.227
When experienced surgeons perform
thyroidectomies, complications occur at a lower rate. A study of 5860
patients found that surgeons who performed more than 100
thyroidectomies a year had the lowest overall complication rate (4.3%),
whereas surgeons who performed fewer than 10 thyroidectomies a year
had four times as many complications.228
Radioactive Iodine—Diagnostics and Treatment
Diagnostic Whole Body Imaging and Thyroid Stunning
When indicated, diagnostic whole body iodine-131 imaging is
recommended after surgery to assess the completeness of thyroidectomy
and to assess whether residual disease is present (see RAI Being
Considered Based on Clinicopathologic Features in the NCCN Guidelines
for Papillary, Follicular, and Hürthle Cell Carcinoma). However, a
phenomenon termed “stunning” may occur when imaging doses of iodine-
131 induce follicular cell damage.229
Stunning decreases uptake in the
thyroid remnant or metastases, thus impairing the therapeutic efficacy of
subsequent iodine-131.230
To avoid or reduce the stunning effect, the
following have been suggested: 1) the use of small doses of iodine-131
(1–2 mCi) or iodine-123 (2–4 mCi); and/or 2) a shortened interval (48–72
hours) between the diagnostic iodine-131 dose and the therapeutic dose.
Iodine-123 is more expensive, and smaller iodine-131 doses have reduced
sensitivity when compared with larger iodine-131 doses.229-231
In addition,
a large thyroid remnant may obscure detection of residual disease with
iodine-131 imaging. Some experts recommend that diagnostic iodine-131
imaging be avoided completely with decisions based on the combination
of tumor stage and serum Tg.229
Other experts advocate that whole body
iodine-131 diagnostic imaging may alter therapy, for example: 1) when
unsuspected metastases are identified; or 2) when an unexpectedly large
remnant is identified that requires additional surgery or a reduction in RAI
dosage to avoid substantial radiation thyroiditis.3,229,232,233
If iodine contrast
agent was used with imaging, then RAI should not begin for at least 2
months after the procedure in order to allow for free iodine levels to
decrease and thus allow for optimal RAI uptake.234,235
Note that diagnostic imaging is used less often for patients at low risk. A
false-negative pretreatment scan is possible and should not prevent use of
RAI if otherwise indicated (see Eligibility for Postoperative Radioactive
Iodine [RAI] in this Discussion, below). For known or suspected distant
metastatic disease, diagnostic whole body iodine-123 or iodine-131
imaging before postoperative RAI may be considered.
Eligibility for Postoperative Radioactive Iodine (RAI)
The NCCN Panel recommends a selective use approach to postoperative
RAI administration. The three general, but overlapping, functions of
postoperative RAI administration include: 1) ablation of the normal thyroid
remnant, which may help in surveillance for recurrent disease (see below);
2) adjuvant therapy to try to eliminate suspected micrometastases; or 3)
RAI therapy to treat known persistent disease. The NCCN Guidelines
have three different pathways for postoperative RAI administration based
on clinicopathologic factors: 1) RAI typically recommended; 2) RAI
selectively recommended; and 3) RAI not typically recommended (see
Clinicopathologic Factors in the NCCN Guidelines for Papillary, Follicular,
and Hürthle Cell Carcinoma).
Postoperative RAI is typically recommended for patients at high risk of
having persistent disease remaining after total thyroidectomy and includes
patients with any of the following factors: 1) gross extrathyroidal extension;
2) a primary tumor greater than 4 cm; 3) postoperative unstimulated Tg
greater than 10 ng/mL; or 4) 6 or more positive lymph nodes or bulky
lymph nodes. In the case of follicular or Hürthle cell carcinoma, extensive
vascular invasion (≥4 foci) is another indication for postoperative RAI.
Postoperative RAI is also frequently recommended for patients with
known/suspected distant metastases at presentation (see
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-80-320.jpg)

![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-16
Therefore, in patients at low and intermediate risk, the clinical benefit of
routine remnant ablation as a requirement for optimal follow-up remains
uncertain.
Thyroid hormone withdrawal may be recommended to increase uptake
from RAI treatment.250
Duration of time off thyroid hormone depends on
the extent of thyroidectomy and approach to hormone replacement in the
initial postoperative setting. Two retrospective studies showed that
patients with distantly metastatic RAI-avid differentiated thyroid cancer
who received recombinant human TSH in preparation for RAI treatment
did not differ significantly in treatment response or survival, compared to
patients who received RAI treatment after thyroid hormone
withdrawal.251,252
However, thyroid hormone withdrawal continues to be
preferred by the NCCN Panel for preparation of RAI treatment compared
to thyrotropin alfa, due to an increased likelihood of augmentation of the
delivered radiation dose. Guidance for preparing the patient and managing
iodine-131 administration can be found in the Principles of Radiation and
Radioactive Iodine Therapy: Iodine-131 Administration in the NCCN
Guidelines for Thyroid Carcinoma.
Data suggest that lower doses of RAI are as effective as higher doses—30
versus 100 mCi—for ablation in patients with low-risk thyroid cancer (eg,
T1b/T2 [1–4 cm], clinical N0 disease).35,36,253
The NCCN Guidelines reflect
a more cautious approach to using RAI ablation based on these
randomized trials.254
If RAI ablation is used, the NCCN Guidelines
recommend (category 1) 30 mCi of iodine-131 for RAI ablation in patients
at low risk based on these randomized trials. This same ablation dose—30
mCi—may be considered (category 2B) in patients at slightly higher risk.255
RAI ablation is not recommended in patients at very low risk.
RAI therapy for thyroid cancer carries the risk of possible adverse effects
including salivary gland dysfunction, lacrimal gland dysfunction, transient
gonadal dysfunction, and secondary primary malignancies.256
The possible
benefits of RAI should be weighed with the risk of adverse effects as part
of treatment decision-making.254
Adverse effects may be minimized by
using lower doses of RAI.35
Historically, the three methods of determining iodine-131 therapy activities
(doses) have included: empiric fixed doses, quantitative dosimetry, and
upper-bound limits that are set by blood dosimetry.3,229,257,258
Most patients
at NCCN Member Institutions receive postoperative RAI based on empiric
fixed dosing; a few centers use a combination of blood dosimetry and
quantitative lesional dosimetry. In the past, hospitalization was required to
administer therapeutic doses of iodine-131 greater than 30 mCi (1110
MBq). However, hospitalization is no longer necessary in most states,
because a change in federal regulations permits the use of much larger
iodine-131 doses in patients who are ambulatory.257
However, iodine-131
therapy with high doses (200 mCi) is best done in medical centers with
experience using high doses. Dosimetry can be used to determine the
maximal safe dose for treatment of unresectable, large-volume, iodine-
concentrating, residual, or recurrent disease.
Administration of a fixed dose of iodine-131 is the most widely used and
simplest method. Most clinics use this method regardless of the
percentage uptake of iodine-131 in the remnant or metastatic lesion.
Patients with uptake in tumor are routinely treated with large, fixed
amounts of iodine-131. Lymph node metastases may be treated with
about 100 to 175 mCi (3700–6475 MBq) of iodine-131. Cancer growing
through the thyroid capsule (and incompletely resected) is treated with 150
to 200 mCi (5550–7400 MBq). Patients with distant metastases are
usually treated with 100 to 200 mCi (3700–7400 MBq) of iodine-131,
which typically will not induce radiation sickness or produce serious
damage to other structures but may exceed generally accepted safety
limits to the blood in the elderly and in those with impaired kidney
function.259,260
Diffuse pulmonary metastases that concentrate 50% or
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-82-320.jpg)

![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-18
alfa is well tolerated; nausea (10.5%) and transient mild headache (7.3%)
are its main adverse effects.265
It is associated with significantly fewer
symptoms and dysphoric mood states than hypothyroidism induced by
thyroid hormone withdrawal.269
An international study was performed to assess the effects of two rhTSH
dosing schedules on whole body iodine-131 imaging and serum Tg levels
when compared with imaging and Tg levels obtained after thyroid
hormone withdrawal.265
Data showed that the combination of rhTSH–
stimulated whole body imaging and serum Tg measurements detected
100% of metastatic carcinoma.265
In this study, 0.9 mg of rhTSH was given
intramuscularly every day for 2 days, followed by a minimum of 4 mCi of
iodine-131 on the third day. Whole body imaging and Tg measurements
were performed on the fifth day. Whole body iodine-131 images were
acquired after 30 minutes of imaging or after obtaining 140,000 counts,
whichever came first. A serum Tg of 2.0 ng/mL or higher, obtained 72
hours after the last rhTSH injection, indicates that thyroid tissue or thyroid
carcinoma is present, regardless of the whole body imaging findings.265,270
Measuring Serum Tg and Anti-Tg Antibodies
Serum Tg measurement is the best means of detecting thyroid tissue,
including carcinoma. Tg can be measured when TSH has been
stimulated—either by thyroid hormone withdrawal or by thyrotropin alfa—
because in this setting, serum Tg has a lower false-negative rate than
whole body iodine-131 imaging.264,265,268,271
Serum Tg levels vary in
response to the increase in serum TSH after thyroid hormone withdrawal
or TSH stimulation. Serum Tg generally does not increase as much after
thyrotropin alfa as after withdrawal of thyroid hormone. The conditions for
TSH–stimulated, whole body iodine-131 imaging stipulate using 4-mCi
iodine-131 doses (based on the trial)265
and an imaging time of 30 minutes
or until 140,000 counts are obtained. Tg measurements may also be
obtained without stimulating TSH using ultrasensitive assays (ie, second-
generation Tg immunometric assays [TgIMAs]).267,272
Evaluation of serum
Tg and anti-Tg antibody levels is helpful for the purpose of obtaining a
postoperative baseline.
Functional sensitivity less than or equal to 0.1 ng/mL for Tg and 0.9 ng/mL
for TgAb are reported for newer generation assays, compared to 1.0
ng/mL for Tg and 20 ng/mL for TgAb for older generation assays.266,267
With the availability of next-generation assays, it is now widely accepted
that stimulated Tg is no longer necessary. Anti-Tg antibodies should be
measured in the same serum sample taken for Tg assay, because these
antibodies (which are found in ≤25% of patients with thyroid carcinoma)
invalidate serum Tg measurements in most assays.272-274
These antibodies
typically falsely lower the Tg value in immunochemiluminometric assays
(ICMAs) and immunoradiometric assays (IRMAs), while raising the value
in older radioimmunoassays. Although the clinical importance of anti-Tg
antibodies is unclear, their persistence for more than 1 year after
thyroidectomy and RAI ablation probably indicates the presence of
residual thyroid tissue and possibly an increased risk of recurrence.274
In one study, 49% of patients had a recurrence if they had undetectable
serum Tg and serum anti-Tg antibody levels of 100 units/mL or more when
compared with only 3% of patients with undetectable serum Tg and serum
anti-Tg antibodies of less than 100 units/mL.275
In patients with coexistent
autoimmune thyroid disease at the time of surgery, anti-Tg antibodies may
persist for far longer. In a study of 116 patients with anti-Tg antibodies
before thyroidectomy, antibodies remained detectable for up to 20 years in
some patients without detectable thyroid tissue, and the median time to
disappearance of antibodies was 3 years.276
Patients with persistently
undetectable serum Tg and anti-Tg antibody levels have longer DFS when
compared with patients who have detectable levels.277
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-84-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-19
Treating Patients with Positive Tg and Negative Imaging
Post-treatment iodine-131 imaging may indicate the location of
metastases when the serum Tg level is increased, but a tumor [or
metastases] cannot be found by physical examination or other localizing
techniques such as diagnostic iodine-131 imaging, neck ultrasonography,
CT, MRI, or PET. Pulmonary metastases may be found only after
administering therapeutic doses of iodine-131 and obtaining whole body
imaging within a few days of treatment.278
In a study of 283 patients
treated with 100 mCi (3700 MBq) of iodine-131, 6.4% had lung and bone
metastases detected after treatment that had been suspected based on
high serum Tg concentrations alone but that had not been detected after
2-mCi (74 MBq) diagnostic imaging.279
Unfortunately, most patients who are diagnostic imaging–negative and
Tg-positive are not rendered disease free by iodine-131 therapy; however,
the tumor burden may be diminished.280
Thus, most patients with residual
or recurrent disease confined to the neck undergo reoperation rather than
RAI therapy in the hopes of a cure. RAI therapy is more commonly
considered for those with distant metastases or inoperable local disease.
Patients not benefiting from this therapy can be considered for clinical
trials, especially those patients with progressive metastatic disease. When
a large tumor is not visible on diagnostic whole body imaging, its ability to
concentrate iodine-131 is very low; thus, the tumor will not respond to
iodine-131 therapy.
Thyroid Hormone Suppression of TSH
The use of postoperative levothyroxine to decrease TSH levels is
considered optimal in treatment of patients with papillary, follicular, or
Hürthle cell carcinoma, because TSH is a trophic hormone that can
stimulate the growth of cells derived from thyroid follicular epithelium.246,281-
283
However, the optimal serum levels of TSH have not been defined
because of a lack of specific data; therefore, the NCCN Panel
recommends tailoring the degree of TSH suppression to the risk of
recurrence and death from thyroid cancer for each individual patient. For
patients with known residual carcinoma or those at high risk for
recurrence, the recommended TSH level is below 0.1 mU/L. For patients
at low risk and for those patients with an excellent response to initial
therapy who are in remission, the recommended TSH level is either
slightly below or slightly above the lower limit of the reference range (0.5–
2 mU/L). The risks and benefits of TSH-suppressive therapy must be
balanced for each individual patient because of the potential toxicities
associated with TSH-suppressive doses of levothyroxine, including cardiac
tachyarrhythmias (especially in the elderly), bone demineralization
(particularly in post-menopausal women), and frank symptoms of
thyrotoxicosis.3,284,285
An adequate daily intake of calcium (1200 mg/day)
and vitamin D (1000 units/day) is recommended for patients whose TSH
levels are chronically suppressed. However, reports do not suggest that
bone mineral density is altered in patients receiving levothyroxine.286,287
Decreased recurrence and cancer-specific mortality rates for differentiated
thyroid carcinoma have been reported for patients treated with thyroid
hormone suppressive therapy.12,240,243,283,288-290
The average dosage
needed to attain serum TSH levels in the euthyroid range is higher in
patients who have been treated for thyroid carcinoma (2.11 mcg/kg per
day) than in those patients with spontaneously occurring primary
hypothyroidism (1.62 mcg/kg per day).290
Even higher doses are required
to suppress serum TSH in patients who have been treated for thyroid
carcinoma. The optimal TSH level to be achieved is uncertain in patients
who have been treated for thyroid carcinoma. Superior outcomes were
associated with aggressive thyroid hormone suppression therapy in
patients at high risk but were achieved with modest suppression in
patients with stage II disease.243
Excessive TSH suppression (into the
undetectable, thyrotoxic range) is not required to prevent disease
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-85-320.jpg)

![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-21
disease.309
Novel treatments for patients with metastatic differentiated
thyroid carcinoma have been evaluated.310-317
Agents include multitargeted
kinase inhibitors, such as lenvatinib,310,313,318-325
sorafenib,326-333
sunitinib,331,334,335
axitinib,336-338
everolimus,339,340
vandetanib,341
cabozantinib,311,342
and pazopanib343
; BRAF V600E mutant inhibitors, such
as vemurafenib or dabrafenib344-347
; tropomyosin receptor kinase (TRK)
inhibitors, such as larotrectinib or entrectinib348,349
; RET inhibitors such as
selpercatinib or pralsetinib350,351
; and anti-PD-1 antibodies such as
pembrolizumab.352
Data suggest that anaplastic lymphoma kinase (ALK)
inhibitors may be effective in patients with papillary carcinoma who have
ALK gene fusion.353-356
Clinical trials suggest that kinase inhibitors have a clinical benefit (partial
response rates plus stable disease) in 50% to 60% of subjects, usually for
about 12 to 24 months.313,321,331,343,357-359
Lenvatinib is the preferred
systemic therapy option for the treatment of patients with RAI-refractory
differentiated thyroid cancer (see Papillary Thyroid Carcinoma in this
Discussion and the NCCN Guidelines for Papillary [Thyroid] Carcinoma).
Vandetanib and cabozantinib, oral kinase inhibitors, are preferred
systemic therapy options for the treatment of medullary carcinoma in
patients with unresectable locally advanced or metastatic disease, and
RET inhibitors (selpercatinib and pralsetinib) are preferred options for RET
mutation-positive disease (see Medullary Thyroid Carcinoma in this
Discussion and the NCCN Guidelines for Medullary [Thyroid] Carcinoma).
Cabozantinib is also an option for RAI-refractory differentiated thyroid
carcinoma that has progressed on VEGFR-targeted therapies such as
lenvatinib and sorafenib.360
Severe or fatal side effects from kinase
inhibitors include bleeding, hypertension, stroke, and liver toxicity;
however, most side effects can be managed and are reversible with
discontinuation of the drug.320,321,361-366
Dose modifications of kinase
inhibitors may be required. Pazopanib has been reported to cause
reversible hypopigmentation.367
Papillary Thyroid Carcinoma
Surgical Therapy
Imaging is performed before surgery to ascertain the extent of disease and
to aid in the surgical decision-making process. A cervical ultrasound,
including the thyroid and the central and lateral compartments, is the
recommended principal imaging modality.368
In one report, cervical
ultrasound performed before primary surgery for newly diagnosed thyroid
cancer identified metastatic sites not appreciated on physical examination
in 20% of patients, and surgical strategy was altered in 39% of patients.369
Surgeon-performed preoperative ultrasound identified nonpalpable
metastatic lymph nodes in 24% of patients.370
In more than 700 patients
with PTC, preoperative ultrasound detected nonpalpable nodal
metastases in 33% of subjects.371
Preoperative ultrasound findings altered
the operation in more than 40% of cases. In another report,372
operative
management was altered in 23% of the total group due to findings on the
preoperative ultrasound. These studies indicate that preoperative
ultrasound has a high sensitivity for nodal disease and will detect
nonpalpable nodal metastases in 20% to 33% of patients, and ultrasound
should alter the index operation in a similar percentage of patients. In most
cases, lesions suspicious for locoregional recurrence, which are amenable
to needle biopsy, should be interrogated with FNA biopsy before surgery.
Tg washout assay is a useful adjunct to FNA biopsy in these cases,
particularly if cytology is negative. Cross-sectional imaging (CT or MRI)
should be performed for locally advanced disease (eg, if the thyroid lesion
is fixed, bulky, or substernal) or for vocal cord paresis. Iodinated contrast
is required for optimal cervical imaging with CT, although iodinated
contrast will delay treatment with RAI; delaying RAI treatment is not
harmful. Assessment of vocal cord mobility is recommended for patients
with abnormal voice, a surgical history involving the recurrent laryngeal or
vagus nerves, invasive disease, or bulky disease of the central neck.
Evaluation is essential in patients with voice changes. Vocal cord mobility
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-87-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-22
may be evaluated by ultrasound, mirror indirect laryngoscopy, or fiber-
optic laryngoscopy.373
The NCCN Panel agreed on the characteristics of patients at higher risk
who require total thyroidectomy as the primary treatment (see
Preoperative or Intraoperative Decision-Making Criteria in the NCCN
Guidelines for Papillary [Thyroid] Carcinoma).3,374,375
A total thyroidectomy
is recommended for patients with any one of the following factors,
including: known distant metastases, extrathyroidal extension, tumor
larger than 4 cm in diameter, lateral cervical lymph node metastases or
gross central neck lymph node metastases, or poorly differentiated
histology. Total thyroidectomy may be considered for patients with bilateral
nodularity or a prior exposure to radiation (category 2B for radiation
exposure). Clinically positive and/or biopsy-proven nodal metastases
should be treated with a formal compartmental resection. In the central
neck, this is achieved through a unilateral or bilateral level VI dissection. In
the lateral compartment, a formal modified radical neck dissection
including levels II, III, IV, and Vb should be performed.376
Extending the
dissection field into levels I or Va may be necessary when these levels are
clinically involved. Based on the results of two randomized controlled
trials, the panel does not recommend prophylactic central neck dissection
if the cervical lymph nodes are clinically negative. Two trials of randomized
patients with cN0 PTC to receive either total thyroidectomy alone or total
thyroidectomy plus central neck dissection showed no difference in
outcomes between the two groups.377,378
Central neck dissection will be
required ipsilateral to a modified radical neck dissection done for clinically
involved lateral neck lymph nodes in most cases. Selective dissection of
individual nodal metastases (ie, cherry picking) is not considered adequate
surgery for nodal disease in a previously undissected field.
The NCCN Panel did not uniformly agree about the preferred primary
surgery for patients with PTC who are assumed to be at lower risk of
cancer-specific mortality. As previously mentioned, the extent of thyroid
resection—ipsilateral lobectomy versus total thyroidectomy—is very
controversial for lower-risk PTC, and lobectomy is preferred for these
patients, while total thyroidectomy is a category 2B option (see Ipsilateral
Lobectomy Versus Total Thyroidectomy in this Discussion). Lobectomy
plus isthmusectomy is recommended for patients who cannot (or refuse
to) take thyroid hormone replacement therapy for the remainder of their
lives.222
Note that some patients prefer to have total thyroidectomy to
avoid having a second surgery (ie, completion thyroidectomy). Other
patients prefer to have a lobectomy in an attempt to avoid thyroid hormone
replacement therapy. Most guidelines (eg, NCCN, ATA3
) do not
recommend active surveillance for patients with PTC. However, for PTC 1
cm or smaller and no concerning lymph node involvement or risk features
(eg, posterior location, abutting the trachea or apparent invasion), surgery
may not be warranted, and active surveillance with ultrasound may be
sufficient.379-382
A study of more than 5000 patients found that survival of patients after
partial thyroidectomy was similar to the survival after total thyroidectomy
for patients at low and high risk.383
An observational study (SEER
database) in more than 35,000 patients with PTC limited to the thyroid
gland suggests that survival is similar whether (or not) patients are treated
in the first year after diagnosis and whether they undergo lobectomy or
total thyroidectomy.384
Another study of 2784 patients with differentiated
thyroid carcinoma (86% with PTC) found that total thyroidectomy was
associated with increased survival in patients at high risk.243
A study in
52,173 patients found that total thyroidectomy reduces recurrence rates
and improves survival in patients with PTC of 1 cm or larger when
compared with lobectomy.385
For patients at lower risk who undergo lobectomy plus isthmusectomy,
completion of thyroidectomy is recommended for any one of the following
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-88-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-23
risk factors: large tumor (4 cm), gross positive resection margins, gross
extrathyroidal extension, confirmed contralateral disease, vascular
invasion, poorly differentiated disease, or confirmed nodal metastases.
While a retrospective study using the National Cancer Database has
shown that a sizable percentage of patients with differentiated thyroid
cancer receive RAI therapy following lobectomy,386
the panel does not
support this practice due to a lack of data showing benefit. Therefore, RAI
is not recommended following lobectomy for differentiated thyroid cancer.
PTC with lymphatic invasion or macroscopic multifocal disease (1 cm)
may warrant a completion thyroidectomy (see Primary Treatment in the
NCCN Guidelines for Papillary [Thyroid] Carcinoma); disease monitoring
(category 2B) is another option for these patients. Measurement of Tg and
anti-Tg antibodies may be useful for obtaining a postoperative baseline,
but data to interpret these antibodies in the setting of an intact thyroid lobe
are lacking.387
Levothyroxine therapy can be considered for these patients
to maintain low or normal TSH levels (see Principles of TSH Suppression
in the NCCN Guidelines for Thyroid Carcinoma). Disease monitoring is
sufficient for tumors resected with lobectomy with all of the following:
negative resection margins, no contralateral lesion, no suspicious lymph
node(s), and small (≤4 cm) PTCs. Levothyroxine therapy to reduce serum
TSH to low or low-normal concentrations can be considered for these
patients (see Principles of TSH Suppression in the NCCN Guidelines for
Thyroid Carcinoma).
Radioactive Iodine Therapy
Postoperative RAI administration is recommended when a number of
clinical factors predict a significant risk of recurrence, distant metastases,
or disease-specific mortality. Clinicopathologic factors can be used to
guide decisions about whether to use initial postoperative RAI (see
Clinicopathologic Factors in the NCCN Guidelines for Papillary [Thyroid]
Carcinoma). Algorithms can assist in decision-making about use of RAI in
different settings: 1) RAI is not typically indicated for patients classified as
having a low risk of recurrence/disease-specific mortality; 2) RAI is not
recommended after lobectomy; 3) RAI may be considered for patients
without gross residual disease, but data are conflicting regarding the
benefit of RAI in this setting; and 4) RAI is often used for patients with
known or suspected distant metastatic disease at presentation. However,
some patients may have metastatic disease that may not be amenable to
RAI therapy, which is also known as iodine-refractory disease (see
Treatment of Metastatic Disease Not Amenable to RAI Therapy in the
NCCN Guidelines for Papillary [Thyroid] Carcinoma). Even in the absence
of thyroid bed uptake, postoperative RAI treatment may be considered.
RAI is also often used to reduce the risk of recurrent thyroid cancer in
patients deemed higher-risk based on surgical pathology, even if there is
no evidence of structural or biochemical disease present initially in the
postoperative period (see Recurrent Disease in this Discussion).
All patients should be examined, and cross-sectional imaging (CT or MRI
of neck with contrast) should be used to evaluate gross residual disease.
Palpable neck disease should be surgically resected before any RAI
treatment. A negative pregnancy test is required before the administration
of RAI in women of childbearing potential. The administered activity of RAI
therapy should be adjusted for pediatric patients.388
Dose should also be
modified if higher than expected uptake, such as in the event of residual
thyroid uptake or distant metastasis.
For patients with unresectable gross residual disease in the neck (RAI
uptake absent) that is refractory to RAI, EBRT or IMRT can be considered
if disease is threatening vital structures, is viscerally invasive, or is rapidly
progressing (see Postsurgical Evaluation in the NCCN Guidelines for
Papillary [Thyroid] Carcinoma).3,299,300,389-391
Enrollment in a neoadjuvant
clinical trial should be considered. Patients with bulky, locoregional,
viscerally invasive disease or rapid progression should be referred to a
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-89-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-24
high-volume multidisciplinary institution, including referral to a radiation
oncologist. Patients with unresectable gross residual disease who
received upfront EBRT or IMRT and with absent RAI should be monitored,
or systemic therapy treatment may be considered.
Surveillance and Maintenance
The recommendations for surveillance and maintenance are described in
the algorithm (see Disease Monitoring in the NCCN Guidelines for
Papillary [Thyroid] Carcinoma). About 85% of patients are considered to
be low risk after surgery for papillary thyroid cancer.246
In patients treated
with lobectomy, disease monitoring following surgery includes physical
examination, TSH assessment, and periodic neck ultrasound. If abnormal
contralateral nodule or lymph nodes are found, then biopsy should be
carried out.
In patients who have had total (or near total) thyroidectomy and thyroid
remnant ablation, the ATA Guidelines define the absence of persistent
tumor (also known as no evidence of disease [NED]) as: 1) absence of
clinical evidence of tumor; 2) absence of imaging evidence of tumor; and
3) undetectable Tg levels (during either TSH suppression or TSH
stimulation) and absence of anti-Tg antibodies.3
Patients treated with total
thyroidectomy should be followed with physical examination and
measurement of TSH, Tg, and Tg ab. RAI imaging (TSH-stimulated
[during either TSH suppression or TSH stimulation]) can be considered in
patients at high risk for persistent or recurrent disease, distant metastases,
or disease-specific mortality; patients with previous RAI-avid metastases;
or patients with abnormal Tg levels, stable or increasing Tg ab, or
abnormal ultrasound results. A tumor is considered iodine-responsive if
follow-up iodine-123 or low-dose iodine-131 whole body diagnostic
imaging done 6 to 12 months after iodine-131 treatment is negative or
shows decreasing uptake compared to pretreatment scans.3
Favorable
response to iodine-131 treatment is also assessed through change in
volume of known iodine-concentrated lesions by CT or MRI, as well as by
decreasing unstimulated or stimulated Tg levels.3
A subgroup of patients at low risk (eg, micropapillary carcinomas entirely
confined to the thyroid gland) may only require periodic neck ultrasound
follow-up (without stimulated Tg or follow-up whole body imaging) as long
as their basal Tg remains low (see Disease Monitoring in the NCCN
Guidelines for Papillary [Thyroid] Carcinoma). Otherwise, long-term
ultrasound follow-up is not required. Note that Tg should be measured
using the same laboratory and the same assay, because Tg levels vary
widely between laboratories.3
Patients with clinically significant residual
disease can typically be identified by the trend in Tg levels over time.3
Non-RAI imaging—such as ultrasound of the central and lateral neck
compartments, neck CT, chest CT, or FDG-PET/CT—may be considered
if RAI imaging is negative and stimulated Tg is greater than 2 to 5 ng/mL.
High-risk factors include incomplete tumor resection, macroscopic tumor
invasion, and distant metastases in patients at high risk for persistent or
recurrent disease, distant metastases, or disease-specific mortality (see
Consideration for Initial Postoperative RAI Therapy in the NCCN
Guidelines for Papillary [Thyroid] Carcinoma).3
Recurrent Disease
The NCCN Panel agrees that surgery is the preferred therapy for
locoregional recurrent disease if the tumor is resectable (see Recurrent
Disease in the NCCN Guidelines for Papillary [Thyroid] Carcinoma).
Cervical ultrasound, including the central and lateral compartments, is the
principal imaging modality when locoregional recurrence is suspected.3
Cross-sectional imaging with CT or MRI may also be valuable for
evaluation and surgical planning, especially when reliable high-resolution
diagnostic ultrasound is unavailable and/or there is suspicion of invasion
into the aerodigestive tract. In most cases, lesions suspicious for
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-90-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-25
locoregional recurrence, which are amenable to needle biopsy, should be
interrogated with FNA biopsy before surgery. Tg washout assay may be a
useful adjunct to FNA biopsy in these cases, particularly if cytology is
negative. Preoperative iodine whole body scan can be used to guide
subsequent use of RAI or other follow-up approach.
Clinically significant nodal recurrence in a previously undissected nodal
basin should be treated with a formal compartmental resection.3
In the
central neck, this is usually achieved through a unilateral level VI
dissection and, occasionally, a level VII dissection. In the lateral
compartment, a formal modified radical neck dissection—including levels
II, III, IV, and Vb—should be performed. Extending the dissection field into
levels I or Va may be necessary when these levels are clinically involved.
Selective dissection of individual nodal metastases (cherry picking) is not
considered adequate surgery for nodal disease in a previously
undissected field, and is not recommended in the NCCN Guidelines for
Thyroid Carcinoma. Clinically significant nodal recurrence detected in a
previously dissected nodal basin may be treated with a more focused
dissection of the region containing the metastatic disease. For example, a
level II recurrence detected in a patient who underwent a modified radical
neck dissection as part of the primary treatment may only require selective
dissection of level II. Likewise, a central neck recurrence detected in a
patient who underwent a central neck dissection as part of the primary
treatment may only require a focused resection of the region of
recurrence.
For unresectable locoregional recurrence, RAI treatment and EBRT or
IMRT are recommended if the iodine-131 imaging is positive.392
Local
therapies, such as ethanol ablation or RFA, are also an option if
available.393
EBRT or IMRT alone is another option in the absence of
iodine-131 uptake for select patients not responsive to other
therapies.300,394
EBRT improves local control in patients with gross residual
non-RAI–avid disease following surgery.293
When recurrent disease is
suspected based on progressively rising Tg values (basal or stimulated)
and negative imaging studies (including PET scans), RAI therapy can be
considered using an empirically determined dose of greater than or equal
to 100 mCi of iodine-131 (see Recurrent Disease in the NCCN Guidelines
for Papillary [Thyroid] Carcinoma). The NCCN Panel had a major
disagreement (category 3) about recommending post-treatment iodine-131
imaging in this setting, because some do not feel that these patients
should have imaging. No study has shown a decrease in morbidity or
mortality in patients treated with iodine-131 on the basis of increased Tg
measurements alone. In a long-term follow-up study, no survival
advantage was associated with empiric high-dose RAI in patients with
negative imaging.395
Further, potential long-term side effects (ie,
xerostomia, nasolacrimal duct stenosis, bone marrow and gonadal
compromise, the risk of hematologic and other malignancies) may negate
any benefit.396,397
Active surveillance may be considered for patients with
low-volume disease that is stable and distant from critical structures.
Metastatic Disease
RAI therapy may be used to treat metastatic disease that is iodine-avid, or
local therapies such as ethanol ablation, cryoablation, or RFA may be
used for these patients, if available. For metastatic disease not amenable
to RAI therapy, several therapeutic approaches are recommended,
depending on the site and number of tumor foci (see Treatment of
Metastatic Disease Not Amenable to RAI Therapy in the NCCN Guidelines
for Papillary [Thyroid] Carcinoma).3,398
Patients should continue to receive
levothyroxine to suppress TSH levels. If not already done, then genomic
testing should be done to identify potentially actionable mutations (eg,
ALK, NTRK, and RET gene fusions; DNA mismatch repair deficiency
[dMMR]; microsatellite instability [MSI]; tumor mutational burden [TMB]).
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-91-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-26
For skeletal metastases, consider surgical palliation for symptomatic or
asymptomatic tumors in weight-bearing extremities; other therapeutic
options are EBRT, SBRT, or other local therapies.303,304,399-401
Intravenous
bisphosphonate (eg, pamidronate or zoledronic acid) or denosumab
therapy may be considered for bone metastases; data show that these
agents prevent skeletal-related events.402-404
Embolization (or other
interventional procedures) of metastases can also be considered either
prior to resection or as an alternative to resection.399,405
RAI is not likely to
be curative, but improved survival has been observed in these
patients.184,406
For solitary or limited CNS lesions, either neurosurgical resection or SRS
is preferred (see the NCCN Guidelines for Central Nervous System
Cancers).305,306
For multiple CNS lesions, EBRT can be considered,293
as
well as surgical resection for select cases such as for acute
decompression (see Treatment of Metastatic Disease Not Amenable to
RAI Therapy in the NCCN Guidelines for Papillary [Thyroid] Carcinoma).
For multiple or extensive CNS lesions, radiotherapy (SRS or whole brain
RT) is recommended, with resection in select cases. If whole brain RT is
used, then 30 Gy in 10 daily fractions, or 45 Gy in 1.8 Gy daily fractions if
good performance status, are acceptable dosing schedules.407
For clinically progressive or symptomatic disease, systemic therapy should
be considered. Recommended systemic therapy options include: 1)
lenvatinib (preferred) or sorafenib;320,326
2) clinical trials; 3) other small-
molecule kinase inhibitors if a clinical trial is not available; or 4) resection
of distant metastases and/or EBRT or IMRT.408,409
Lenvatinib and
sorafenib are category 1 options in this setting based on phase 3
randomized trials.320,326
The NCCN Panel feels that lenvatinib is the
preferred agent in this setting based on a response rate of 65% for
lenvatinib when compared with 12% for sorafenib, although these agents
have not been directly compared.318,320,326
The decision to use lenvatinib or
sorafenib should be individualized for each patient based on likelihood of
response and comorbidities. The efficacy of lenvatinib or sorafenib for
patients with brain metastases has not been established; therefore,
consultation with neurosurgeons and radiation oncologists is
recommended. Kinase inhibitors have been used as second-line therapy
for thyroid cancer.321,410
Lenvatinib was compared with placebo in patients with metastatic
differentiated thyroid cancer that was refractory to RAI in a phase 3
randomized trial.320
Patients receiving lenvatinib had a progression-free
survival (PFS) of 18.3 months compared with 3.6 months for those
receiving placebo (HR, 0.21; 99% CI, 0.14–0.31; P .001). Six treatment-
related deaths occurred in the lenvatinib group. A prespecified subset
analysis of this trial found that the PFS benefit of lenvatinib compared to
placebo was maintained in both older (65 years) and younger (≤65 years)
patients. Furthermore, a longer median OS was observed in older patients
treated with lenvatinib compared to placebo (HR, 0.27; 95% CI, 0.31–0.91;
P = .20), although older patients also had higher rates of grade 3 and
greater adverse effects from treatment. These results suggest that
lenvatinib is an appropriate treatment option for patients of any age with
RAI-refractory differentiated thyroid cancer.411
Another phase 3 randomized trial compared sorafenib with placebo in
patients with RAI-refractory metastatic differentiated thyroid cancer.326
Patients receiving sorafenib had a PFS of 10.8 months compared with 5.8
months for those receiving placebo (HR, 0.59; 95% CI, 0.45–0.76; P
.0001). One treatment-related death occurred in the sorafenib group.
Hand-foot syndrome is common with sorafenib and may require dose
adjustments.
A phase 3 randomized trial compared cabozantinib to placebo in patients
with RAI-refractory differentiated thyroid cancer that progressed during or
after treatment with one or two vascular endothelial growth factor receptor
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-92-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-27
(VEGFR) TKIs (including lenvatinib and sorafenib).360
Analyses of the ITT
population (n = 187) showed that the median PFS was not reached in
patients receiving cabozantinib, compared with 1.9 months for those
receiving placebo (HR, 0.22; 99% CI, 0.13–0.36; P .0001). Serious
treatment-related adverse events occurred in 16% of patients in the
cabozantinib arm, compared with 2% in the placebo arm, though no
treatment-related deaths occurred. Cabozantinib is a category 1 option for
patients with disease progression after lenvatinib and/or sorafenib.
Other commercially available small-molecule kinase inhibitors may also be
considered for progressive and/or symptomatic disease if a clinical trial is
not available—including vemurafenib or dabrafenib (for BRAF-positive
disease), larotrectinib or entrectinib (for NTRK gene fusion-positive
disease), selpercatinib or pralsetinib (for RET fusion-positive disease),
axitinib, everolimus, pazopanib, sunitinib, vandetanib, or cabozantinib—
although some of these have not been approved by the FDA for
differentiated thyroid cancer (see Principles of Kinase Inhibitor Therapy in
Advanced Thyroid Carcinoma in the NCCN Guidelines for Thyroid
Carcinoma). Note that kinase inhibitor therapy may not be appropriate for
patients with stable or slowly progressive indolent disease,320,326,362,412,413
and caution should be used in patients with untreated CNS metastases
due to the associated bleeding risk.414
The anti-PD-1 antibody
pembrolizumab is also an option for patients with TMB-high (TMB-H) (≥10
mutations/megabase [mut/Mb]) disease.352
Active surveillance is often
appropriate for asymptomatic patients with indolent disease and no brain
metastasis.321,362
Palliative care is recommended as indicated for patients
with advanced and progressive disease (see the NCCN Guidelines for
Palliative Care, available at www.NCCN.org).
Follicular Thyroid Carcinoma
The diagnosis and treatment of papillary and follicular thyroid carcinoma
are similar; therefore, only the important differences in the management of
follicular carcinoma are highlighted. The diagnosis of follicular thyroid
carcinoma requires evidence of invasion through the capsule of the nodule
or the presence of vascular invasion.48,415
Unlike PTC, FNA is not specific
for follicular thyroid carcinoma and accounts for the main differences in
management of the two tumor types.56,62,97,416
The FNA cytologic diagnosis
of “[suspicious for] follicular neoplasm” will prove to be a benign follicular
adenoma in 80% of cases. However, 20% of patients with follicular
neoplasms on FNA are ultimately diagnosed with follicular thyroid
carcinoma when the final pathology is assessed. Molecular diagnostic
testing may be useful to determine the status of follicular lesions or lesions
of indeterminate significance (including follicular neoplasms, AUS, or
FLUS) as more or less likely to be malignant based on the genetic profile.
Because most patients with follicular neoplasms on FNA actually have
benign disease, total thyroidectomy is recommended only if radiographic
evidence or interoperative findings of extrathyroidal extension or tumor
larger than 4 cm in diameter are apparent at the time of surgery, or if the
patient opts for total thyroidectomy to avoid a second procedure (ie,
completion thyroidectomy) if cancer is found at pathologic review.415,417
Otherwise, lobectomy plus isthmusectomy is advised as the initial surgery.
If invasive follicular thyroid carcinoma (widely invasive or encapsulated
angioinvasive with four or more vessels) is found on the final histologic
sections after lobectomy plus isthmusectomy, prompt completion of
thyroidectomy is recommended (see Primary Treatment in the NCCN
Guidelines for Follicular [Thyroid] Carcinoma).
Completion thyroidectomy may also be recommended for tumors that, on
final histologic sections after lobectomy plus isthmusectomy, are identified
as minimally invasive follicular thyroid carcinomas or encapsulated
angioinvasive with less than four vessels. Minimally invasive cancer is
characterized as an encapsulated tumor with microscopic capsular
invasion and without vascular invasion.3
It is preferred for minimally
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-93-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-28
invasive cancers, as well as NIFTP tumors, to simply be followed carefully,
because minimally invasive follicular carcinomas and NIFTP usually have
an excellent prognosis. Although deaths attributed to minimally invasive
follicular carcinoma do occasionally occur, the panel feels that the benefit
of completion thyroidectomy for small minimally invasive follicular cancers
may not justify the additional morbidity.
The other features of management and follow-up for follicular thyroid
carcinoma are similar to those of PTC. Clinicopathologic factors can be
used to guide decisions about whether to administer initial postoperative
RAI (see Clinicopathologic Factors in the NCCN Guidelines for Follicular
[Thyroid] Carcinoma). The NCCN Guidelines provide algorithms to assist
in decision-making about use of RAI in different settings: 1) RAI is not
typically indicated for patients classified as having a low risk of
recurrence/disease-specific mortality; 2) RAI may be considered for
patients without gross residual disease, but data are conflicting regarding
the benefit of RAI in this setting; and 3) RAI is often used for patients with
known or suspected distant metastatic disease (see Clinicopathologic
Factors in the NCCN Guidelines for Follicular [Thyroid] Carcinoma).
RAI ablation may be used to destroy residual thyroid tissue when RAI
uptake is absent; alternatively, these patients may be followed without RAI
ablation. Iodine-131 ablation and post-treatment imaging (with
consideration of dosimetry for distant metastasis) are recommended for
suspected or proven iodine-131–avid metastatic foci (see RAI Being
Considered Based on Clinicopathologic Features in the NCCN Guidelines
for Follicular [Thyroid] Carcinoma). In patients with known or suspected
distantly metastatic disease, radioiodine diagnostic imaging (iodine-123 or
iodine-131) with adequate TSH stimulation (thyroid withdrawal or
thyrotropin alfa) before iodine-131 therapy is administered may be
considered, but the problem of stunning should be considered (see section
on Diagnostic Whole Body Imaging and Thyroid Stunning in this
Discussion). For patients who have a central neck recurrence,
preoperative vocal cord assessment should be considered (see Recurrent
Disease in the NCCN Guidelines for Follicular [Thyroid] Carcinoma).
Hürthle Cell Carcinoma
This tumor (also known as oxyphilic cell carcinoma) is usually assumed to
be a variant of follicular thyroid carcinoma,189,418
although the prognosis of
Hürthle cell carcinoma is worse.164,415,417,419,420
The Hürthle cell variant of
PTC is rare and seems to have a prognosis similar to follicular
carcinoma.421
Historically, studies showed that molecular diagnostics did
not perform well for Hürthle cell neoplasms.83,87,88
However, with the
advent of newer genomic tests, the validity for Hürthle cell carcinoma is
improving (see FNA Results in this Discussion, above).88,89
The management of Hürthle cell carcinoma is almost identical to follicular
thyroid carcinoma, except that 1) locoregional nodal metastases may be
more common, and therefore therapeutic lymph node dissections of the
affected compartment may be needed for clinically apparent biopsy-
proven disease; and 2) metastatic Hürthle cell tumors are less likely to
concentrate iodine-131 (see Papillary Thyroid Carcinoma: Surgical
Therapy in this Discussion).422
Postoperative EBRT or IMRT can be
considered for: 1) unresectable primary Hürthle cell lesions that do not
concentrate iodine-131 if disease is threatening vital structures; and 2)
unresectable locoregional recurrence (see Postsurgical Evaluation and
Recurrent Disease in the NCCN Guidelines for Hürthle Cell [Thyroid]
Carcinoma), similar to the management for follicular thyroid carcinoma.
Clinicopathologic factors can be used to guide decisions about whether to
use initial postoperative RAI (see Clinicopathologic Factors in the NCCN
Guidelines for Hürthle Cell [Thyroid] Carcinoma). The NCCN Guidelines
provide algorithms to assist in decision-making about use of RAI in
different settings: 1) RAI is not typically indicated for patients classified as
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-94-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-29
having a low risk of recurrence/disease-specific mortality; 2) RAI may be
considered for patients without gross residual disease, but data are
conflicting regarding the benefit of RAI in this setting; and 3) RAI is often
used for patients with known or suspected distant metastatic disease (see
Clinicopathologic Factors in the NCCN Guidelines for Hürthle cell [Thyroid]
Carcinoma).
RAI therapy has been reported to decrease the risk of locoregional
recurrence and is recommended for unresectable disease with positive
iodine-131 imaging. Iodine-131 therapy (100–150 mCi) may be considered
after thyroidectomy for patients with rising or newly elevated Tg levels who
have negative scans (including FDG-PET) (see Recurrent Disease in the
NCCN Guidelines for Hürthle Cell [Thyroid] Carcinoma).164
Pretreatment
radioiodine diagnostic imaging (iodine-123 or iodine-131) with adequate
TSH stimulation (thyroid withdrawal or thyrotropin alfa) may be considered
in patients with known or suspected distantly metastatic disease (see RAI
Being Considered Based on Clinicopathologic Features in the NCCN
Guidelines for Hürthle Cell [Thyroid] Carcinoma). Since Hürthle cell
carcinoma tends to be non–iodine-avid, negative scans that were done
without single-photon emission CT (SPECT) are likely to have missed
distant structural disease. Therefore, if Tg is high and/or pathology is high-
risk, then FDG-PET is indicated.
Medullary Thyroid Carcinoma
Medullary thyroid carcinoma (MTC) arises from the neuroendocrine
parafollicular C cells of the thyroid.423-426
Sporadic MTC accounts for about
80% of all cases of the disease. The remaining cases consist of inherited
tumor syndromes, such as: 1) MEN type 2A (MEN2A), which is the most
common type; and 2) MEN2B.427,428
Familial MTC is now viewed as a
variant of MEN2A.423,424,429
Sporadic disease typically presents in the fifth
or sixth decade of life. Inherited forms of the disease tend to present at
earlier ages.423,424
The 5-year relative survival for stages I to III is about
93%, whereas 5-year survival for stage IV is about 28%.168,189
Because the
C cells are predominantly located in the upper portion of each thyroid lobe,
patients with sporadic disease typically present with upper pole nodules.
Metastatic cervical adenopathy appears in about 50% of patients at initial
presentation. Symptoms of upper aerodigestive tract compression or
invasion are reported by up to 15% of patients with sporadic disease.430
Distant metastases in the lungs or bones cause symptoms in 5% to 10%
of patients. Many patients with advanced MTC can have diarrhea, Cushing
syndrome, or facial flushing, because the tumor can secrete calcitonin and
sometimes other hormonally active peptides (ie, adrenocorticotropic
hormone [ACTH], calcitonin gene-related peptide [CGRP]). Treatment with
somatostatin analogs (eg, octreotide, lanreotide) may be useful in patients
with these symptoms.431
Patients with unresectable or metastatic disease
may have either slowly progressive or rapidly progressive disease.
Nodule Evaluation and Diagnosis
Patients with MTC can be identified by using pathologic diagnosis or by
prospective genetic screening. Separate pathways are included in the
algorithm (see Clinical Presentation in the NCCN Guidelines for Medullary
[Thyroid] Carcinoma) depending on the method of identification.
Sporadic MTC
Sporadic MTC is usually suspected after FNA of a solitary nodule (see
Nodule Evaluation in the NCCN Guidelines for Thyroid Carcinoma).
Reports suggest that about 3% of patients with nodular thyroid disease will
have an increased serum calcitonin level when measured by a sensitive
immunometric assay; 40% of these patients will have MTC at
thyroidectomy.432-434
However, routine measurement of the basal serum
calcitonin concentration is not recommended by the NCCN Panel for
evaluating a patient with nodular thyroid disease because of: 1) the
expense of screening all thyroid nodules and only finding a few cases of
MTC; 2) the lack of confirmatory pentagastrin stimulation testing; and 3)
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-95-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-30
the resulting need for thyroidectomy in some patients who have benign
thyroid disease.435,436
The ATA is equivocal about routine calcitonin
measurement.3
Inherited MTC
For patients with known kindreds with inherited MTC, prospective family
screening with testing for mutant RET genes can identify disease carriers
long before clinical symptoms or signs are noted.425,426
The traditional
approach of stimulating secretion of calcitonin by either pentagastrin or
calcium infusion to identify patients with MTC is no longer recommended,
because elevated calcitonin is not a specific or adequately sensitive
marker for MTC437
and because pentagastrin is no longer available in the
United States. When MEN2A is suspected, the NCCN Guidelines
recommend measurement of calcium levels with (or without) serum intact
parathyroid hormone levels (see Additional Workup in the NCCN
Guidelines for Medullary [Thyroid] Carcinoma). Compared with sporadic
disease, the typical age of presentation for familial disease is the third or
fourth decade of life, without gender preference. In patients with MEN2A,
signs or symptoms of hyperparathyroidism or pheochromocytoma rarely
present before those of MTC, even in the absence of screening.
All familial forms of MTC and MEN2 are inherited in an
autosomal-dominant fashion. Mutations in the RET proto-oncogene are
found in at least 95% of kindreds with MEN2A and 88% of cases of familial
MTC.425,426,438
The RET proto-oncogene codes for a cell
membrane-associated tyrosine kinase receptor for a glial, cell line-derived
neurotrophic factor. Mutations associated with MEN2A and familial MTC
have been primarily identified in several codons of the cysteine-rich
extracellular domains of exons 10, 11, and 13; MEN2B and some familial
MTC mutations are found within the intracellular exons 14 to 16.423,424
Somatic mutations in exons 11, 13, and 16 have also been found in at
least 25% of sporadic MTC tumors—particularly the codon 918 mutation
that activates the tyrosine kinase function of the receptor—and are
associated with poorer prognosis of the patient.
About 6% of patients with clinically sporadic MTC carry a germline RET
mutation, leading to identification of new kindreds with multiple (previously
undiagnosed) affected individuals.439,440
Germline testing for RET
proto-oncogene mutations with genetic counseling by a physician or
genetic counselor is recommended for all patients with newly diagnosed,
clinically apparent, sporadic MTC.441
If a germline RET mutation is found,
then mutation testing should also be done for family members. MTC can
involve difficult ethical decisions for clinicians if parents or guardians
refuse screening and/or treatment for children with possible MTC.442
Principles regarding genetic risk assessment can be found in the NCCN
Guidelines for Genetic/Familial High-Risk Assessment: Breast, Ovarian,
and Pancreatic (available at www.NCCN.org).
The generally accepted preoperative workup includes measurement of
serum markers (basal serum calcitonin and serum carcinoembryonic
antigen [CEA]) and screening of patients with germline RET
proto-oncogene mutations for pheochromocytoma (MEN2A and MEN2B)
and hyperparathyroidism (MEN2A). Before surgery for MTC, it is important
to diagnose and address coexisting pheochromocytoma to avoid
hypertensive crisis during surgery (see
Pheochromocytoma/Paraganglioma in the NCCN Guidelines for
Neuroendocrine Tumors, available at www.NCCN.org).
Pheochromocytoma can be removed using laparoscopic
adrenalectomy.423,424,443
Preoperative thyroid and neck ultrasound
(including central and lateral neck compartments) is recommended.
Contrast-enhanced CT of neck/chest and liver MRI or 3-phase CT of liver
can be considered as clinically indicated, such as in cases of high burden
of disease, calcitonin greater than 400 pg/mL, or elevated CEA levels.
Distant metastasis does not contraindicate surgery.423,424
Liver imaging is
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-96-320.jpg)

![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-32
Patients with pheochromocytomas must be treated preoperatively with
alpha-adrenergic blockade (phenoxybenzamine) or with
alpha-methyltyrosine to avoid a hypertensive crisis during surgery. Forced
hydration and alpha-blockade are necessary to prevent hypotension after
the tumor is removed. After institution of alpha-blockade and hydration,
beta-adrenergic blockade may be necessary to treat tachyarrhythmia.
Total thyroidectomy and bilateral central neck dissection (level VI) are
indicated in all patients with MTC whose tumor is 1 cm or larger or who
have bilateral thyroid disease; total thyroidectomy is recommended and
neck dissection can be considered for those whose tumor is smaller than 1
cm and for unilateral thyroid disease (see Primary Treatment in the NCCN
Guidelines for Medullary [Thyroid] Carcinoma).374,430
Given the risks of
thyroidectomy in very young children, referral to a surgeon and team with
experience in pediatric thyroid surgery is advised.
If a patient with inherited disease is diagnosed early enough, the
recommendation is to perform a prophylactic total thyroidectomy by age 5
years or when the mutation is identified (in older patients), especially in
patients with codon 609, 611, 618, 620, 630, or 634 RET
mutations.423,424,458
Note that C634 mutations are the most common
mutations.423,424
Total thyroidectomy is recommended in the first year of
life or at diagnosis for patients with MEN2B who have codon 883 RET
mutations, 918 RET mutations, or compound heterozygous (V804M +
E805K, V804M + Y806C, or V804M + S904C) RET mutations (see Clinical
Presentation in the NCCN Guidelines for Medullary [Thyroid] Carcinoma),
because these RET mutations carry the highest risk for MTC (ie, level
D).423,424,459
However, for patients with codon 768, 790, 791, 804, and 891 RET (risk
level A) mutations, the lethality of MTC may be lower than with other RET
mutations.423,424,459,460
In patients with these less high-risk (ie, lower-risk
level A) RET mutations, annual basal calcitonin testing and annual
ultrasound are recommended; total thyroidectomy and central node
dissection may be deferred if these tests are normal, there is no family
history of aggressive MTC, and the family agrees to defer surgery (see
Additional Workup in the NCCN Guidelines for Medullary [Thyroid]
Carcinoma).423,424,461,462
Delaying thyroidectomy may also be appropriate
for children with lower-risk mutations (ie, level A) because of the late onset
of MTC development.423,424,460,461,463
A study found no evidence of
persistent or recurrent MTC 5 years or more after prophylactic total
thyroidectomy in young patients with RET mutations for MEN2A; longer
follow-up is necessary to determine if these patients are cured.464
Variations in surgical strategy for MTC depend on the risk for locoregional
node metastases and on whether simultaneous parathyroid resection for
hyperparathyroidism is necessary.423,424
A bilateral central neck dissection
(level VI) can be considered for all patients with MEN2B. For those
patients with MEN2A who undergo prophylactic thyroidectomy, therapeutic
ipsilateral or bilateral central neck dissection (level VI) is recommended if
patients have an increased calcitonin or CEA test or if ultrasound shows a
thyroid or nodal abnormality. Similarly, more extensive lymph node
dissection (levels II–V) is considered for these patients with primary
tumor(s) 1 cm or larger in diameter (0.5 cm for patients with MEN2B) or
for patients with central compartment lymph node metastases (see
Primary Treatment in the NCCN Guidelines for Medullary [Thyroid]
Carcinoma).
With a concurrent diagnosis of hyperparathyroidism in MEN2A or familial
MTC, the surgeon should leave or autotransplant the equivalent mass of
one normal parathyroid gland if multiglandular hyperplasia is present.
Cryopreservation of resected parathyroid tissue should be considered to
allow future implantation in the event of iatrogenic hypoparathyroidism.
Disfiguring radical node dissections do not improve prognosis and are not
indicated. In the presence of grossly invasive disease, more extended
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-98-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-33
procedures with resection of involved neck structures may be appropriate.
Function-preserving approaches are preferred. In some patients, MTC is
diagnosed after thyroid surgery. In these patients, additional workup is
recommended to ascertain whether they have RET proto-oncogene
mutations (eg, exons 10, 11, 13–16), which will determine whether they
need additional surgery (eg, completion thyroidectomy and/or neck
dissection) (see Additional Workup in the NCCN Guidelines for Medullary
[Thyroid] Carcinoma).
Adjuvant RT
EBRT and IMRT have not been adequately studied as adjuvant therapy in
MTC.301,423,465
Slight improvements in local DFS have been reported after
EBRT for selected patients, such as those with extrathyroidal invasion or
extensive locoregional node involvement.466
However, most centers do not
have extensive experience with adjuvant EBRT or IMRT for this disease.
While therapeutic EBRT or IMRT may be considered for grossly
incomplete resection when additional attempts at surgical resection have
been ruled out, adjuvant EBRT or IMRT is rarely recommended (see
Primary Treatment in the NCCN Guidelines for Medullary [Thyroid]
Carcinoma).423,424
EBRT or IMRT can also be given to palliate painful or
progressing bone metastases.303,304,401,423,424
There is little evidence
regarding appropriate treatment volumes for use of RT for MTC, but
guidance regarding EBRT dose and fractionation is provided in the
Principles of Radiation and Radioactive Iodine Therapy: External Beam
Radiation Therapy in the NCCN Guidelines for Thyroid Carcinoma.
Persistently Increased Calcitonin
Basal serum concentrations of calcitonin and CEA should be measured 2
or 3 months postoperatively. About 80% of patients with palpable MTC
and 50% of those with nonpalpable but macroscopic MTC who undergo
supposedly curative resection have serum calcitonin values indicative of
residual disease. Those patients with residual disease may benefit from
further evaluation to detect either residual resectable disease in the neck
or the presence of distant metastases. Patients with detectable basal
calcitonin or elevated CEA who have negative imaging and who are
asymptomatic may be followed (see Surveillance in the NCCN Guidelines
for Medullary [Thyroid] Carcinoma). Patients with a basal serum calcitonin
value greater than 1000 pg/mL—and with no obvious MTC in the neck and
upper mediastinum—probably have distant metastases, most likely in the
liver. However, occasionally patients have relatively low serum CEA and
calcitonin levels but have extensive metastatic disease; initial
postoperative imaging is therefore reasonable despite the absence of very
high serum markers.
The prognosis for patients with postoperative hypercalcitoninemia
depends primarily on the extent of disease at the time of initial surgery. In
a study of 31 patients (10 patients with apparently sporadic disease, 15
patients with MEN2A, and 6 patients with MEN2B), the 5- and 10-year
survival rates were 90% and 86%, respectively.467
Two studies have
reported higher mortality rates for patients with high postoperative serum
calcitonin values, with more than 50% of patients having a recurrence
during a mean follow-up of 10 years.449,468
Routine lymphadenectomy or
excision of palpable tumor generally fails to normalize the serum calcitonin
concentrations in such patients; therefore, some have focused on
detection and eradication of microscopic tumor deposits with a curative
intent in patients without distant metastases. Extensive dissection to
remove all nodal and perinodal tissue from the neck and upper
mediastinum was first reported to normalize the serum calcitonin levels in
4 of 11 patients at least 2 years postoperatively.469
In subsequent larger
studies, 20% to 40% of patients undergoing microdissection of the central
and bilateral neck compartments were biochemically cured, with minimal
perioperative morbidity.470,471
When repeat surgery is planned for curative
intent, preoperative assessment should include locoregional imaging (ie,
ultrasonography of the neck and upper mediastinum) and attempts to
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-99-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-34
exclude patients with distant metastases, which may include
contrast-enhanced CT or MRI of the neck, chest, and abdomen.471
Postoperative Management and Surveillance
Calcitonin is very useful for surveillance, because this hormone is only
produced in the parafollicular cells. Thus, measurements of serum
calcitonin and CEA levels are the cornerstone of postoperative
assessment for residual disease (see Management 2–3 Months
Postoperative in the NCCN Guidelines for Medullary [Thyroid] Carcinoma).
For patients with a detectable basal calcitonin or elevated CEA level, neck
ultrasound is recommended. Patients with undetectable calcitonin levels
and normal CEA levels can subsequently be followed with annual
measurements of serum markers. Additional studies or more frequent
testing can be done for those with significantly rising calcitonin or CEA.
Nonetheless, the likelihood of significant residual disease is very low in
patients with an undetectable basal calcitonin level in a sensitive assay. If
the patient has MEN2, annual screening for pheochromocytoma (MEN2B
or MEN2A) and hyperparathyroidism (MEN2A) should also be performed.
For some low-risk RET mutations (eg, codons 768, 790, 804, or 891), less
frequent screening may be appropriate.
Patients with detectable serum markers (ie, calcitonin levels ≥150 pg/mL)
should have CT or MRI of the neck, chest, and liver. Bone scan and MRI
of axial skeleton should be considered in select patients such as those
with very elevated calcitonin levels.423,424
The NCCN Panel recognizes that
many different imaging modalities may be used to examine for residual or
metastatic tumor, but there is insufficient evidence to recommend any
particular choice or combination of tests.423,424
For patients with asymptomatic disease and detectable markers in whom
imaging fails to identify foci of disease, the NCCN Panel recommends
conservative surveillance with repeat measurement of the serum markers
every 6 to 12 months. Additional imaging studies (eg, FDG PET/CT, Ga-
68 DOTATATE, or MRI with contrast of the neck, chest, and abdomen with
liver protocol) may be indicated depending on calcitonin/CEA doubling
time. For patients who are asymptomatic with abnormal markers and
repeated negative imaging, continued disease monitoring or consideration
of cervical reoperation is recommended if primary surgery was incomplete.
For the patient with increasing serum markers, more frequent imaging may
be considered. Outside of clinical trials, no therapeutic intervention is
recommended on the basis of abnormal markers alone.
Recurrent or Persistent Disease
Kinase inhibitors may be appropriate for select patients with recurrent or
persistent MTC that is not resectable (see Recurrent or Persistent Disease
in the NCCN Guidelines for Medullary [Thyroid] Carcinoma). Although
kinase inhibitors may be recommended for patients with MTC, it is
important to note that kinase inhibitors may not be appropriate for patients
with stable or slowly progressing indolent disease.321,472,473
Vandetanib and
cabozantinib are oral receptor kinase inhibitors that increase PFS in
patients with metastatic MTC.454,457,474-476
RET inhibitors that are FDA-
approved for RET-mutated MTC include selpercatinib and pralsetinib.350,351
Vandetanib is a multitargeted kinase inhibitor; it inhibits RET, VEGFR, and
endothelial growth factor receptor (EGFR).454
In a phase III randomized
trial in patients with unresectable, locally advanced, or metastatic MTC (n
= 331), vandetanib increased PFS when compared with placebo (HR,
0.46; 95% CI, 0.31–0.69; P .001); OS data are not yet available.454
A
post-hoc subgroup analysis including 184 patients with symptomatic and
progressive disease at baseline also showed increased PFS (HR, 0.43;
95% CI, 0.28–0.64; P .001) in patients who received vandetanib,
compared to the placebo, although time to worsening pain was not
significantly different between the two groups (HR, 0.67; 95% CI, 0.43–
1.04; P = .07).477
In this subgroup, the overall response rate (ORR) was
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-100-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-35
37% in the patients who received vandetanib and 2% in patients who
received the placebo (P .001). The FDA approved the use of vandetanib
for patients with locally advanced or metastatic MTC who are not eligible
for surgery and whose disease is causing symptoms or growing.455
However, access is restricted through a vandetanib Risk Evaluation and
Mitigation Strategy (REMS) program because of potential cardiac
toxicity.478
The NCCN Panel recommends vandetanib (category 1) as a
preferred option for patients with recurrent or persistent MTC (see
Recurrent or Persistent Disease in the NCCN Guidelines for Medullary
[Thyroid] Carcinoma).
Cabozantinib is a multitargeted kinase inhibitor that inhibits RET,
VEGFR2, and MET. In a phase 3 randomized trial (EXAM) in patients with
locally advanced or metastatic MTC (n = 330), cabozantinib increased
median PFS when compared with placebo (11.2 vs. 4.0 months; HR, 0.28;
95% CI, 0.19–0.40; P .001).457
Following long-term follow-up, the
median OS for patients treated with cabozantinib was 26.6 months
compared to 21.1 months for placebo, although this difference was not
statistically significant (stratified HR, 0.85; 95% CI, .64–1.12, P = .24).479
Exploratory analyses have suggested that cabozantinib may have a
greater clinical benefit for medullary thyroid cancers harboring RET M918T
or RAS mutations, although prospective trials are needed to confirm.479,480
In 2012, the FDA approved the use of cabozantinib for patients with
progressive, metastatic MTC.456
The NCCN Panel recommends
cabozantinib (category 1) as a preferred option based on the phase III
randomized trial and FDA approval (see Recurrent or Persistent Disease
in the NCCN Guidelines for Medullary [Thyroid] Carcinoma). Rare adverse
events with cabozantinib include severe bleeding and gastrointestinal
perforations or fistulas; severe hemorrhage is a contraindication for
cabozantinib.
RET mutations account for a significant percentage of MTC cases,481,482
supporting investigation into the impact of recently developed RET
inhibitors on RET-mutated MTC. The phase I–II LIBRETTO-001 study
evaluated the efficacy of the RET inhibitor selpercatinib in 143 patients
with RET-mutant MTC.350
In patients previously treated with vandetanib or
cabozantinib (n = 55), the ORR and 1-year PFS rates were 69% (95% CI,
55%–81%) and 82% (95% CI, 69%–90%), respectively. In patients with no
previous vandetanib or cabozantinib treatment (n = 88), the ORR and 1-
year PFS rates were 73% (95% CI, 62%–82%) and 92% (95% CI, 82%–
97%), respectively. The most commonly reported toxicities (grade 3 and 4)
were hypertension (21%), increased alanine aminotransferase (11%),
increased aspartate aminotransferase (9%), hyponatremia (8%), and
diarrhea (6%). Dose reductions due to treatment-related adverse events
were reported in 30% of patients. Pralsetinib, another RET inhibitor, was
evaluated in the phase I–II ARROW study, which included 92 patients with
RET-mutant MTC.483
The ORR was 60% (95% CI, 46%–74%) in patients
previously treated with vandetanib or cabozantinib (n = 61) and 74% (95%
CI, 49%–91%) in patients with no previous vandetanib or cabozantinib
treatment (n = 22). Pralsetinib was generally well-tolerated, with the most
commonly reported grade 3–4 treatment-related adverse events being
hypertension (11%) and neutropenia (10%). These results are currently
reported in abstract form, and the ARROW study is ongoing and
continuing to enroll patients. In 2020, the FDA approved both of these
RET inhibitors for RET-mutated MTC requiring systemic therapy. Based
on the data and the FDA approvals, the NCCN Panel recommends
selpercatinib and pralsetinib as preferred options for patients with RET-
mutant disease (see Recurrent or Persistent Disease in the NCCN
Guidelines for Medullary [Thyroid] Carcinoma). RET somatic genotyping
may be done in patients who are germline wild-type or if germline status is
unknown.
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-101-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-36
When locoregional disease is identified in the absence of distant
metastases, surgical resection is recommended with (or without)
postoperative EBRT or IMRT. For unresectable locoregional disease that
is symptomatic or progressing by Response Evaluation Criteria in Solid
Tumors (RECIST) criteria,484
the following options can be considered: 1)
RT (EBRT or IMRT); or 2) systemic therapy. Treatment can be considered
for symptomatic distant metastases (eg, those in bone); recommended
options include: 1) palliative resection, ablation (eg, radiofrequency,
embolization), or other regional treatment; 2) vandetanib (category 1); or
3) cabozantinib (category 1) (see Recurrent or Persistent Disease in the
NCCN Guidelines for Medullary [Thyroid] Carcinoma). These interventions
may be considered for asymptomatic distant metastases (especially for
progressive disease), but disease monitoring is acceptable given the lack
of data regarding alteration in outcome. If systemic therapy is indicated,
then vandetanib and cabozantinib are category 1 preferred options.
Selpercatinib or pralsetinib are preferred options for patients with RET-
mutation positive disease. Pembrolizumab is also an option for patients
with TMB-H (≥10 mut/Mb) disease, based on results of the phase II
KEYNOTE-158 trial, which included two patients with thyroid cancer.352
The NCCN Panel does not recommend treatment with systemic therapy
for increasing calcitonin or CEA alone.
In the setting of symptomatic disease or progression, the NCCN Panel
recommends systemic therapy or enrollment in a clinical trial. As stated
above for locoregional disease, preferred systemic therapy options include
vandetanib (category 1), cabozantinib (category 1), and selpercatinib or
pralsetinib for patients with RET-mutation positive disease. Other small-
molecule kinase inhibitors (ie, sorafenib, sunitinib, lenvatinib, pazopanib)
may be considered if clinical trials or the NCCN-preferred systemic
therapy options are not available or are not appropriate.334,485-490
If the
patient progresses on a preferred option, then systemic chemotherapy can
be administered using dacarbazine or combinations including
dacarbazine.423,491-493
Pembrolizumab is also an option for patients with
TMB-H (≥10 mut/Mb) disease (useful in certain circumstances).352
EBRT
or IMRT can be used for local symptoms. Intravenous bisphosphonate
therapy or denosumab can be considered for bone metastases.402-404
Best
supportive care is also recommended.
Results from clinical trials have shown the effectiveness of novel
multitargeted therapies including sunitinib,334,335
sorafenib,412,486
lenvatinib,489
and pazopanib488
in MTC. Severe or fatal side effects from
kinase inhibitors include bleeding, hypertension, and liver toxicity;
however, many side effects can be managed.362,365,408,413
Because some
patients may have indolent and asymptomatic disease, potentially toxic
therapy may not be appropriate.362
Novel therapies and the management of aggressive MTC have been
reviewed.315,423,494-497
Of interest, calcitonin levels decreased dramatically
after vandetanib therapy, which did not directly correlate with changes in
tumor volume; thus, calcitonin may not be a reliable marker of tumor
response in patients receiving RET inhibitor therapy.498
A phase 2 trial in
patients with progressive metastatic MTC assessed treatment using
pretargeted anti–CEA radioimmunotherapy with iodine-131.499
OS was
improved in the subset of patients with increased calcitonin doubling
times.500
Anaplastic Thyroid Carcinoma
ATCs are aggressive undifferentiated tumors, with a disease-specific
mortality approaching 100%.501
Patients with anaplastic carcinoma are
older than those with differentiated carcinomas, with a mean age at
diagnosis of approximately 71 years.502
Fewer than 10% of patients are
younger than 50 years, and 60% to 70% of patients are women.108,502
The
incidence of ATC is decreasing because of better management of
differentiated thyroid cancer and because of increased iodine in the
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-102-320.jpg)


![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-39
Systemic Therapy
Systemic therapy recommendations are described in the algorithm (see
Systemic Therapy for Anaplastic Thyroid Carcinoma in the NCCN
Guidelines for Anaplastic [Thyroid] Carcinoma). When systemic therapy is
indicated, targeted therapy options are preferred. Dabrafenib plus
trametinib combination is an option for BRAF V600E mutation-positive
tumors,530
larotrectinib or entrectinib are options for NTRK gene fusion-
positive tumors,348,349,531
selpercatinib or pralsetinib are options for RET
fusion-positive disease,350,351
and pembrolizumab is an option for TMB-H
(≥10 mut/Mb) disease.352
Other recommended regimens include paclitaxel
and doxorubicin monotherapies.510
Doxorubicin combined with cisplatin is
an option based on a small randomized trial.532
Paclitaxel combined with
carboplatin and docetaxel combined with doxorubicin are also systemic
therapy options for patients with metastatic ATC, but these are category
2B options based on low-quality evidence510
and less panel consensus.
The NCCN Panel recommends molecular testing to help inform decisions
regarding systemic therapy and to determine eligibility for clinical trials.
The dosage and frequency of administration of all the recommended
systemic therapy agents are provided in the algorithm. Either concurrent
chemoradiation or chemotherapy alone regimens may be used depending
on the clinical setting; however, chemoradiation is generally more toxic. If
using chemoradiation, the ATA Guidelines recommend using weekly
chemotherapy regimens.510
A phase 2, open-label trial of 16 patients with BRAF V600E-mutated ATC
evaluated the efficacy and safety of dabrafenib 150 mg, twice daily, in
combination with trametinib 2 mg, once daily.530
The confirmed ORR was
69% (95% CI, 41%–89%), with seven responses ongoing. While duration
of response, PFS, and OS were not yet reached, the 12-month estimates
were 90%, 79%, and 80%, respectively. The combination was found to be
well-tolerated as evaluated in 100 patients across seven rare tumor types;
common adverse events included fatigue (38%), pyrexia (37%), and
nausea (35%).530
Based on these data, the FDA approved
dabrafenib/trametinib for ATC with BRAF V600E mutation in 2018.
A pooled analysis of three studies (a phase 1 including adults, a phase 1/2
involving children, and a phase 2 involving adolescents and adults)
studied the safety and efficacy of larotrectinib in patients with NTRK gene
fusion-positive tumors, including seven patients with thyroid cancer of
which one patient had ATC.348,533
For the whole population, the ORR was
75% (95% CI, 61%–85%) by independent review and 80% (95% CI, 67%–
90%) by investigator assessment.348,533
One hundred percent of the thyroid
cancers in this study responded to larotrectinib, with one complete
response and four partial responses.533
Larotrectinib was found to be well-
tolerated, as the majority (93%) of adverse events were grades 1 or 2 and
no treatment-related adverse events of grades 3 or 4 occurred in more
than 5% of patients.348
A pooled analysis from a phase II trial and two
phase I trials including 54 patients with NTRK gene fusion-positive cancer
(9% having thyroid cancer) showed an objective response rate of 57.4%
for entrectinib, another TRK inhibitor.349
Based on these data, the FDA
approved larotrectinib and entrectinib for treatment of patients with NTRK
gene fusion-positive tumors, and the panel also recommends NTRK
therapy options such as larotrectinib or entrectinib for patients with NTRK
gene fusion-positive metastatic ATC.
The phase I–II LIBRETTO-001 study evaluated the efficacy of the RET
inhibitor selpercatinib in 19 patients with previously treated RET fusion-
positive thyroid cancer (2 patients with anaplastic disease).350
The ORR
was 79% (95% CI, 54%–94%), and 1-year PFS was 64% (95% CI, 37%–
82%). In the ongoing phase I–II ARROW study, pralsetinib, another RET
inhibitor, is being evaluated in patients with RET fusion-positive disease
(NCT03037385). In an analysis including 9 patients with RET fusion-
positive thyroid cancer, the ORR was 89% (95% CI, 52%–100%) with
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-105-320.jpg)
![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-40
durable responses (100% DCR).351
In 2020, the FDA approved both of
these RET inhibitors for RAI-refractory RET fusion-positive thyroid cancer
requiring systemic therapy.
The FDA approved the anti-PD-1 antibody pembrolizumab for treatment of
previously treated TMB-H (≥10 mut/Mb) solid tumors in 2020 based on
results of the phase II KEYNOTE-158 trial, which included two patients
with thyroid cancer.352
For the whole sample, the ORR was 29% (95% CI,
21%–39%). Grade 3–5 treatment-related adverse events were reported in
15% of the patients. A phase II study evaluated another anti-PD-1
antibody, spartalizumab, in 42 patients with locally advanced or metastatic
ATC.534
The ORR was only 19% (95% CI, 8.6%–34.1%), but was higher
for patients with PD-L1–positive disease (29%; 95% CI, 13.2%–48.7%)
and highest in patients with PD-L1 greater than 50% (35%; 95% CI,
14.2%–61.7%).
Treatment with anthracyclines and taxanes is generally not very effective
for advanced anaplastic disease, although some patients may show
disease response or have stable disease.510,527
Single-agent doxorubicin is
approved by the FDA for ATC. A randomized trial including 84 patients
with advanced thyroid cancer (not limited to ATC) showed an 11.6%
complete response rate in patients who received doxorubicin combined
with cisplatin, compared to a complete response in 0 patients who
received single-agent doxorubicin.532
ORR did not differ significantly
between the study arms (26% vs. 17%, respectively). Single-agent
paclitaxel may benefit some patients with newly diagnosed ATC;
increased survival has been reported in patients with stage IVB
disease.535-537
If weekly paclitaxel is used, the ATA Guidelines510
recommend using paclitaxel at 60 to 90 mg/m2
IV weekly and not the dose
previously reported in the study by Ain et al.537
Given the poor outcome with current standard therapy, all patients—
regardless of surgical resection—should be considered for clinical trials.
Previous clinical trials for ATC have tested therapies including
fosbretabulin (and its parent drug, combretastatin A4 phosphate [CA4P],
and crolibulin [EPC2407], which are vascular disrupting agents),
efatutazone (an oral PPAR gamma agonist), and novel multitargeted
therapies including bevacizumab with doxorubicin, sorafenib, sunitinib,
imatinib, and pazopanib.335,538-546
A trial in 80 patients (FACT) reported that
the addition of fosbretabulin—to a carboplatin/paclitaxel regimen—resulted
in a nonsignificant increase in median survival (5.2 vs. 4.0 months).538,547
Preliminary data suggest that ALK inhibitors may be effective in a subset
of patients with papillary thyroid cancer who have ALK gene fusions;
however, these ALK gene fusions are rarely reported in patients with
ATC.353-356
Hyperfractionated EBRT, combined with radiosensitizing doses of
doxorubicin, may increase the local response rate to about 80%, with a
subsequent median survival of 1 year.548
Distant metastases then become
the leading cause of death.549
Similar improvement in local disease control
has been reported with a combination of hyperfractionated RT and
doxorubicin-based regimens, followed by debulking surgery in responsive
patients or other multimodality approaches.527,550-552
IMRT may be useful to
reduce toxicity.465,510,553-557
However, the addition of larger doses of other
chemotherapeutic drugs has not been associated with improved control of
distant disease or with improved survival. Other radiosensitizing agents
that may be considered include docetaxel and paclitaxel with or without
carboplatin.535,537,554,558
Although optimal results have been reported with
hyperfractionated EBRT combined with chemotherapy, the NCCN Panel
acknowledges that considerable toxicity is associated with such treatment
and that prolonged remission is uncommonly reported.559
Multimodality therapy is recommended in patients with locally resectable
disease (see Treatment in the NCCN Guidelines for Anaplastic [Thyroid]
Carcinoma).510,538,553,560-564
Small retrospective studies have reported that
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-106-320.jpg)











![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-52
155. van Heerden JA, Hay ID, Goellner JR, et al. Follicular thyroid
carcinoma with capsular invasion alone: a nonthreatening malignancy.
Surgery 1992;112:1130-1136; discussion 1136-1138. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/1455315.
156. LiVolsi VA, Asa SL. The demise of follicular carcinoma of the thyroid
gland. Thyroid 1994;4:233-236. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/7920009.
157. Brennan MD, Bergstralh EJ, van Heerden JA, McConahey WM.
Follicular thyroid cancer treated at the Mayo Clinic, 1946 through 1970:
initial manifestations, pathologic findings, therapy, and outcome. Mayo
Clin Proc 1991;66:11-22. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/1988751.
158. Lloyd RV, Osamura RY, Klöppel G, Rosai J, eds. WHO Classification
of Tumors of Endocrine Organs. In: Bosman FT, Jaffe ES, Lakhani SR,
Ohgaki H, eds. World Health Organization Classification of Tumors (ed 4).
Lyon, France: International Agency for Research on Cancer; 2017.
159. Maxwell EL, Palme CE, Freeman J. Hürthle cell tumors: applying
molecular markers to define a new management algorithm. Arch
Otolaryngol Head Neck Surg 2006;132:54-58. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/16415430.
160. Belchetz G, Cheung CC, Freeman J, et al. Hürthle cell tumors: using
molecular techniques to define a novel classification system. Arch
Otolaryngol Head Neck Surg 2002;128:237-240. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/11886336.
161. Ganly I, Ricarte Filho J, Eng S, et al. Genomic dissection of Hurthle
cell carcinoma reveals a unique class of thyroid malignancy. J Clin
Endocrinol Metab 2013;98:E962-972. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/23543667.
162. Chen H, Nicol TL, Zeiger MA, et al. Hürthle cell neoplasms of the
thyroid: are there factors predictive of malignancy? Ann Surg
1998;227:542-546. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/9563543.
163. Thompson NW, Dunn EL, Batsakis JG, Nishiyama RH. Hürthle cell
lesions of the thyroid gland. Surg Gynecol Obstet 1974;139:555-560.
Available at: http://www.ncbi.nlm.nih.gov/pubmed/4479589.
164. Lopez-Penabad L, Chiu AC, Hoff AO, et al. Prognostic factors in
patients with Hürthle cell neoplasms of the thyroid. Cancer 2003;97:1186-
1194. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12599224.
165. Samaan NA, Schultz PN, Haynie TP, Ordonez NG. Pulmonary
metastasis of differentiated thyroid carcinoma: treatment results in 101
patients. J Clin Endocrinol Metab 1985;60:376-380. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/3965495.
166. Ruegemer JJ, Hay ID, Bergstralh EJ, et al. Distant metastases in
differentiated thyroid carcinoma: a multivariate analysis of prognostic
variables. J Clin Endocrinol Metab 1988;67:501-508. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/3410936.
167. Samaan NA, Schultz PN, Hickey RC, et al. The results of various
modalities of treatment of well differentiated thyroid carcinomas: a
retrospective review of 1599 patients. J Clin Endocrinol Metab
1992;75:714-720. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/1517360.
168. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. A National
Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in
the U.S., 1985-1995 [see comments]. Cancer 1998;83:2638-2648.
Available at: http://www.ncbi.nlm.nih.gov/pubmed/9874472.
169. Baudin E, Travagli JP, Ropers J, et al. Microcarcinoma of the thyroid
gland: the Gustave-Roussy Institute experience. Cancer 1998;83:553-559.
Available at: http://www.ncbi.nlm.nih.gov/pubmed/9690549.
170. Roti E, degli Uberti EC, Bondanelli M, Braverman LE. Thyroid
papillary microcarcinoma: a descriptive and meta-analysis study. Eur J
Endocrinol 2008;159:659-673. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/18713843.
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-118-320.jpg)
















![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-69
Oncol 2009;10:967-974. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/19767240.
415. McHenry CR, Sandoval BA. Management of follicular and Hürthle cell
neoplasms of the thyroid gland. Surg Oncol Clin N Am 1998;7:893-910.
Available at: http://www.ncbi.nlm.nih.gov/pubmed/9735140.
416. Ustun B, Chhieng D, Van Dyke A, et al. Risk stratification in follicular
neoplasm: a cytological assessment using the modified Bethesda
classification. Cancer Cytopathol 2014;122:536-545. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/24753500.
417. Phitayakorn R, McHenry CR. Follicular and Hürthle cell carcinoma of
the thyroid gland. Surg Oncol Clin N Am 2006;15:603-623. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/16882500.
418. Hedinger CE. [Problems in the classification of thyroid tumors. Their
significance for prognosis and therapy]. Schweiz Med Wochenschr
1993;123:1673-1681. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/8211018.
419. Goffredo P, Roman SA, Sosa JA. Hurthle cell carcinoma: a
population-level analysis of 3311 patients. Cancer 2013;119:504-511.
Available at: http://www.ncbi.nlm.nih.gov/pubmed/22893587.
420. Sugino K, Ito K, Mimura T, et al. Hürthle cell tumor of the thyroid:
analysis of 188 cases. World J Surg 2001;25:1160-1163. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/11571953.
421. Herrera MF, Hay ID, Wu PS, et al. Hürthle cell (oxyphilic) papillary
thyroid carcinoma: a variant with more aggressive biologic behavior. World
J Surg 1992;16:669-674; discussion 774-775. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/1413835.
422. Chindris AM, Casler JD, Bernet VJ, et al. Clinical and molecular
features of Hürthle cell carcinoma of the thyroid. J Clin Endocrinol Metab
2015;100:55-62. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/25259908.
423. Wells SA, Jr., Asa SL, Dralle H, et al. Revised American Thyroid
Association guidelines for the management of medullary thyroid
carcinoma. Thyroid 2015;25:567-610. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/25810047.
424. Kloos RT, Eng C, Evans DB, et al. Medullary thyroid cancer:
management guidelines of the American Thyroid Association. Thyroid
2009;19:565-612. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/19469690.
425. Gagel RF, Hoff AO, Cote GJ. Medullary thyroid carcinoma. In:
Braverman LE, Utiger RD, eds. Werner and Ingbar's The Thyroid: A
Fundamental and Clinical Text, 9th ed. Philadelphia: Lippincott Williams
Wilkins; 2005:967-988.
426. Gagel RF, Cote GJ. Pathogenesis of medullary thyroid carcinoma. In:
JA F, ed. Thyroid Cancer. Boston/Dordrecht/London: Kluwer Academic;
1998:85-103.
427. Gertner ME, Kebebew E. Multiple endocrine neoplasia type 2. Curr
Treat Options Oncol 2004;5:315-325. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/15233908.
428. Raue F, Frank-Raue K. Multiple endocrine neoplasia type 2: 2007
update. Horm Res 2007;68 Suppl 5:101-104. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/18174721.
429. Moers AM, Landsvater RM, Schaap C, et al. Familial medullary
thyroid carcinoma: not a distinct entity? Genotype-phenotype correlation in
a large family. Am J Med 1996;101:635-641. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/9003111.
430. Saad MF, Ordonez NG, Rashid RK, et al. Medullary carcinoma of the
thyroid. A study of the clinical features and prognostic factors in 161
patients. Medicine (Baltimore) 1984;63:319-342. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/6503683.
431. Vitale G, Tagliaferri P, Caraglia M, et al. Slow release lanreotide in
combination with interferon-alpha2b in the treatment of symptomatic
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-135-320.jpg)






![Version 3.2022 © 2022 National Comprehensive Cancer Network©
(NCCN©
), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN.
NCCN Guidelines Version 3.2022
Thyroid Carcinoma
MS-76
525. Burnison CM, Lim S. Multimodal approach to anaplastic thyroid
cancer. Oncology (Williston Park) 2012;26:378-384, 390-398. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/22655531.
526. Wang Y, Tsang R, Asa S, et al. Clinical outcome of anaplastic thyroid
carcinoma treated with radiotherapy of once- and twice-daily fractionation
regimens. Cancer 2006;107:1786-1792. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/16967442.
527. Nachalon Y, Stern-Shavit S, Bachar G, et al. Aggressive Palliation
and Survival in Anaplastic Thyroid Carcinoma. JAMA Otolaryngol Head
Neck Surg 2015;141:1128-1132. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/26512447.
528. Saeed NA, Kelly JR, Deshpande HA, et al. Adjuvant external beam
radiotherapy for surgically resected, nonmetastatic anaplastic thyroid
cancer. Head Neck 2020;42:1031-1044. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/32011055.
529. Pezzi TA, Mohamed ASR, Sheu T, et al. Radiation therapy dose is
associated with improved survival for unresected anaplastic thyroid
carcinoma: Outcomes from the National Cancer Data Base. Cancer
2017;123:1653-1661. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/28026871.
530. Subbiah V, Kreitman RJ, Wainberg ZA, et al. Dabrafenib and
trametinib treatment in patients with locally advanced or metastatic BRAF
V600-mutant anaplastic thyroid cancer. J Clin Oncol 2018;36:7-13.
Available at: https://www.ncbi.nlm.nih.gov/pubmed/29072975.
531. Hong DS, Bauer TM, Lee JJ, et al. Larotrectinib in adult patients with
solid tumours: a multi-centre, open-label, phase I dose-escalation study.
Ann Oncol 2019;30:325-331. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/30624546.
532. Shimaoka K, Schoenfeld DA, DeWys WD, et al. A randomized trial of
doxorubicin versus doxorubicin plus cisplatin in patients with advanced
thyroid carcinoma. Cancer 1985;56:2155-2160. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/3902203.
533. Brose MS, Albert CM, Waguespack SG, et al. Activity of larotrectinib
in patients with advanced TRK fusion thyroid cancer [abstract]. 88th
Annual Meeting of the American Thyroid Association 2018;Clinical Oral
Presentation 10. Available at:
https://www.liebertpub.com/doi/pdf/10.1089/thy.2018.29065.abstracts.
534. Capdevila J, Wirth LJ, Ernst T, et al. PD-1 blockade in anaplastic
thyroid carcinoma. J Clin Oncol 2020;38:2620-2627. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/32364844.
535. Higashiyama T, Ito Y, Hirokawa M, et al. Induction chemotherapy
with weekly paclitaxel administration for anaplastic thyroid carcinoma.
Thyroid 2010;20:7-14. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/20025538.
536. Ain KB. Anaplastic thyroid carcinoma: behavior, biology, and
therapeutic approaches. Thyroid 1998;8:715-726. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/9737368.
537. Ain KB, Egorin MJ, DeSimone PA. Treatment of anaplastic thyroid
carcinoma with paclitaxel: phase 2 trial using ninety-six-hour infusion.
Collaborative Anaplastic Thyroid Cancer Health Intervention Trials
(CATCHIT) Group. Thyroid 2000;10:587-594. Available at:
https://www.ncbi.nlm.nih.gov/pubmed/10958311.
538. Sosa JA, Balkissoon J, Lu SP, et al. Thyroidectomy followed by
fosbretabulin (CA4P) combination regimen appears to suggest
improvement in patient survival in anaplastic thyroid cancer. Surgery
2012;152:1078-1087. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/23158178.
539. Smallridge RC, Marlow LA, Copland JA. Anaplastic thyroid cancer:
molecular pathogenesis and emerging therapies. Endocr Relat Cancer
2009;16:17-44. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/18987168.
540. Savvides P, Nagaiah G, Lavertu P, et al. Phase II trial of sorafenib in
patients with advanced anaplastic carcinoma of the thyroid. Thyroid
Printed by Cristian Díaz rojas on 12/6/2022 11:33:44 PM. For personal use only. Not approved for distribution. Copyright © 2022 National Comprehensive Cancer Network, Inc., All Rights Reserved.](https://image.slidesharecdn.com/thyroid-221220101008-dd5cd148/85/thyroid-pdf-142-320.jpg)