Downloaded 26 times

![[ http://www.umm.edu/patiented/articles/how_serious_hypothyroidism_000038_6.htm -
accessed August 2015 and 08 20 2016]
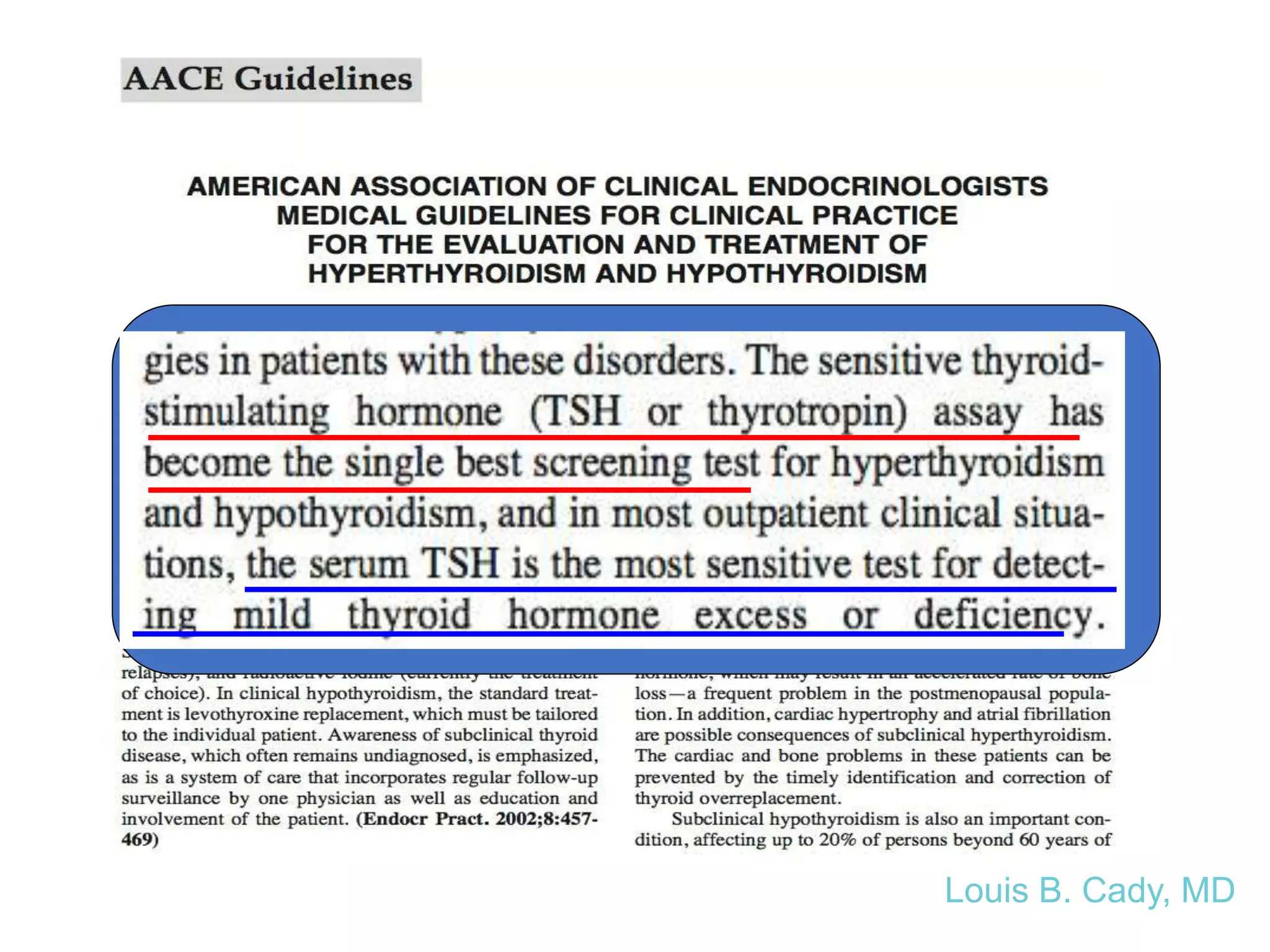
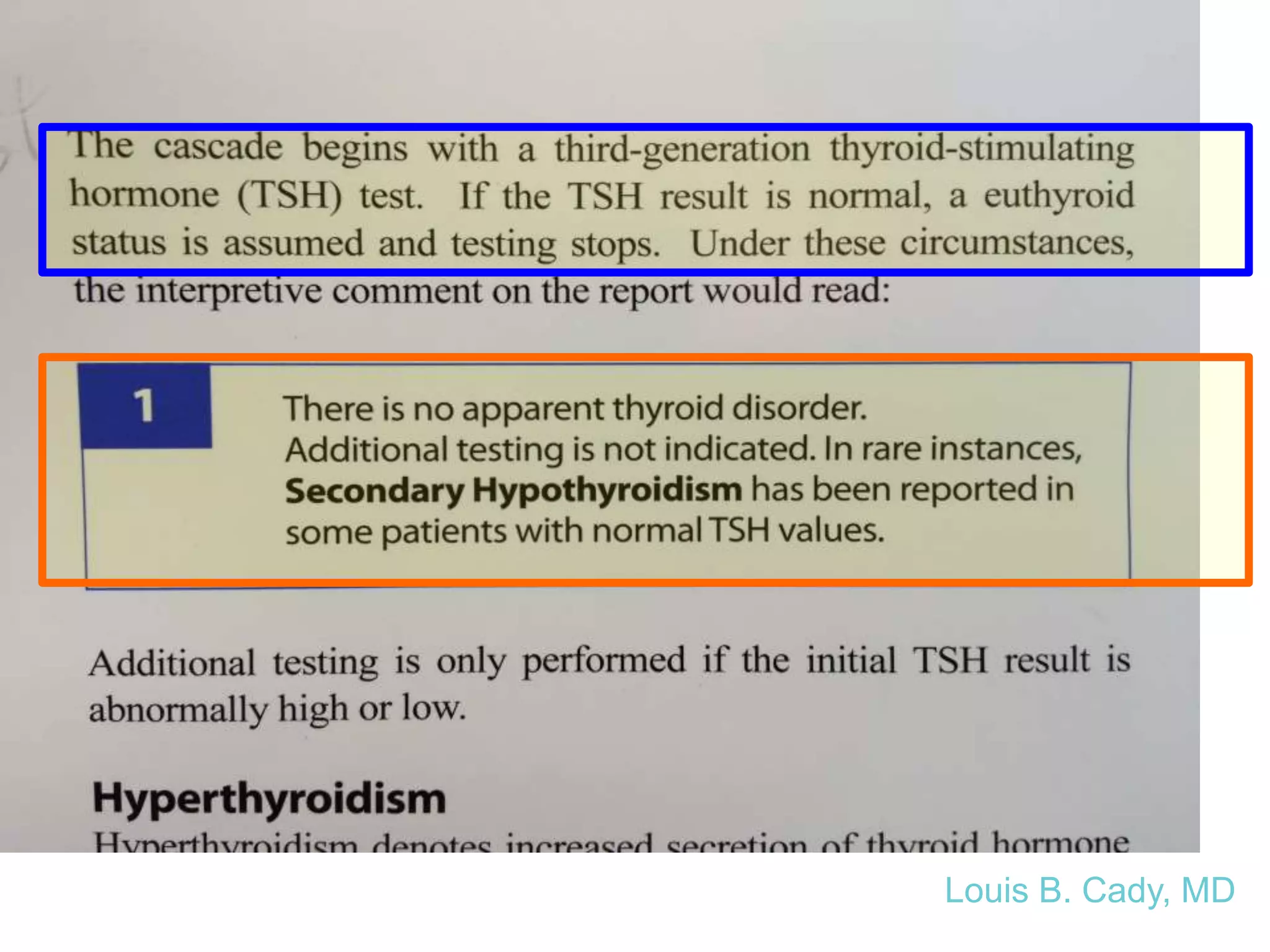
• “Thyrotropin (Thyroid-Stimulating Hormone or
TSH). Measuring TSH is the most sensitive
indicator of hypothyroidism.” (hunh?!) –
accessed 9/5/2011
• “…blood tests for measuring levels of TSH and
free thyroxine (T4) are the only definitive way to
diagnose hypothyroidism” – 10/6/2012
Louis B. Cady, MD](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-9-2048.jpg)
![Who cares
about T3??
Effectively:
- These genes make THR alpha
- THR Alpha is a nuclear receptor for tri-
iodothyronine [T3].
- “[This receptor] has been
shown to mediate the
biological activities of
thyroid hormone.”
- This is where thyroid
(T3) works – AT THE
TISSUE LEVEL.
- (NOT TSH. NOT T4.) Source: Gene ID: 7067, updated 9-Jul-2017](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-19-2048.jpg)
![Some recent citations…
• “Paucity of treatment options for bipolar disorder.” “Many
clues suggesting that T3 could augment and accelerate
treatment response [with lithium and antidepressants].”
• Parmentier T et al. J Affect Disord. 2018 Mar 15;229:410-414.
• “Backing into the future: pharmacological approaches to the
management of resistant depression” (failure of two
antidepressants)= Rx with atypical antipsychotics, lithium,
T3 (triiodothyronine). Ketamine. Anti-inflammatory agents.
Pramipexole (dopamine agonist).
• Psychol Med. 2017 Nov;47(15):2569-2577.](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-31-2048.jpg)
![Subclinical hypothyroidism in
the US– what’s the latest?
As of August 6, 2015• Synthesis: treat only those with TSH >10
– Hennessey JV Espaillat R. Diagnosis and management of Subclinical
Hypothyroidism in Elderly Adults: A Review of the Literature. J
Am Geriatr Soc. 2015 Jul 22. epub ahead of print
• Synthesis: SCH [TSH >/= 4.5- 19.99] associated with hip and
other fractures.
– Blum MR et al. Subclinical thyroid dysfunction and fracture risk: a meta-
analysis. JAMA. 2015 May 26;3(20):2055-65.
• Synthesis: Treatment of SCH [TSH 4-11] improved risk of
coronary heart dz risks. “Direct evidence on the benefits
and harms of screening remains unavailable.”
– Rugge JB et al. Screening for and treatment of thyroid dysfunction: An
evidence review for the US. Rockville (MD) Agency for Healthcare Research
and Quality (IS);2014 Oct. Report No. 15-05217-EF-1.](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-58-2048.jpg)
![Dr. Imre Zs-Nagy, MD – one more time!
Archives of Gerontology and Geriatrics, Volume 48, Issue 3, May-June 2009, 271-275
"[The] gerontological elite has instead sought to
obfuscate the facts ... the reason for this is
nothing less than an abject fear ... to avert their
loss of control, power, prestige, and position in
the multi-billion dollar industry of gerontological
medicine.”
Prof. Dr. Imre Zs.-Nagy, MD - part of the gerontology movement for four
decades; founder and Editor-in-Chief of the Archives of Gerontology and
Geriatrics](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-59-2048.jpg)
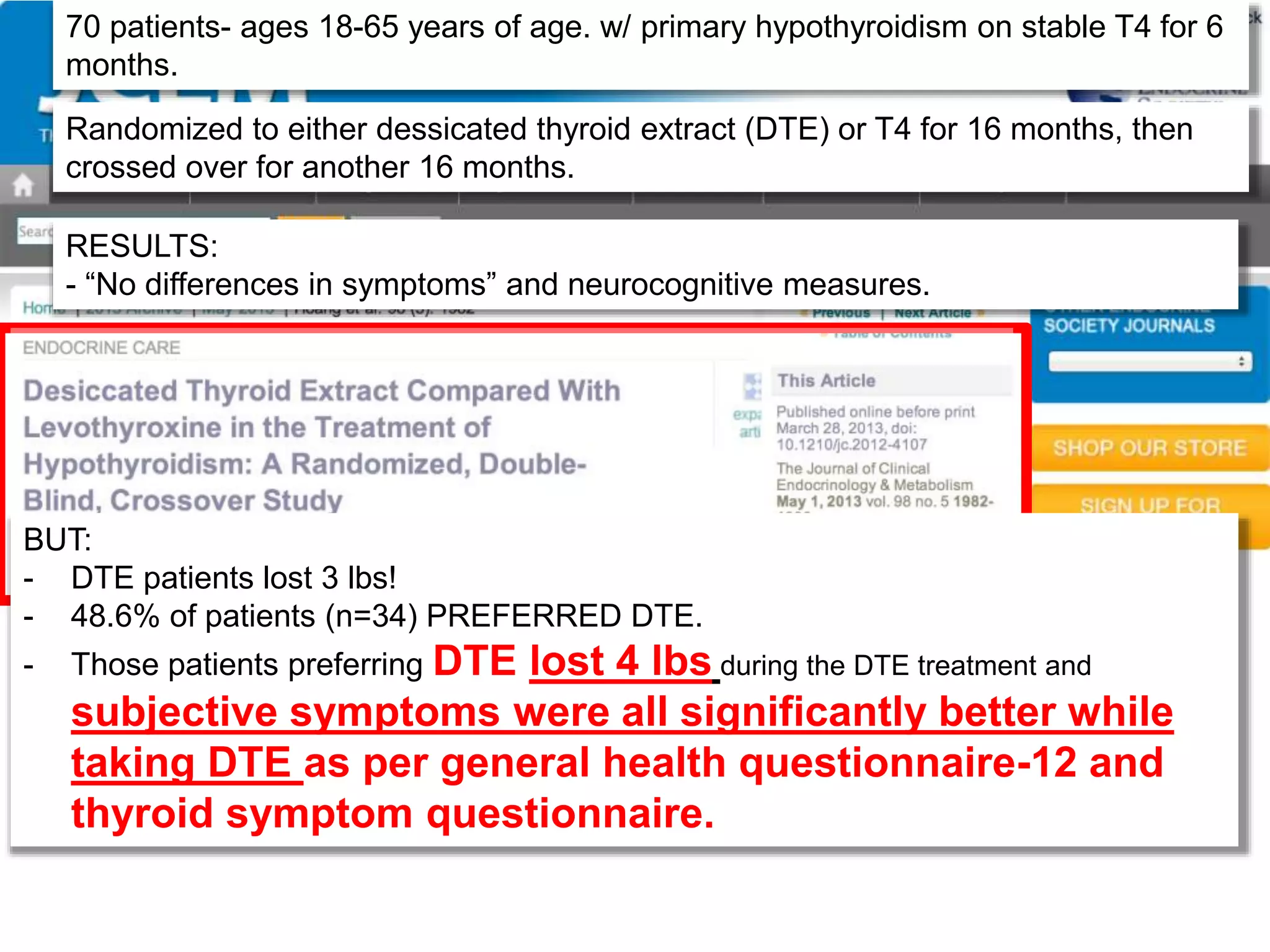
![“Conclusions”:
- DTE therapy did not result in a significant improvement in quality of life; however,
DTE caused modest weight loss and nearly half (46.8%) of the study patients
expressed preference for DTE over L-T4.
DTE therapy may be relevant for some
hypothyroid patients.” [Can you believe it????]](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-71-2048.jpg)
![Framework:
• Decide where in the literature you want to be.
• Do you want to practice the way things “used
to be” or do you want to practice evidence
based medicine?
–[or just blindly listen to the specialty societies
who parrot from the past?]
• Do you want your patient to be “normal” or
“optimal”?
• And can you live with yourself and your
decision?
Louis B. Cady, MD](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-75-2048.jpg)
![RX: You MUST Know This
Transthyretin = carrier protein)
• Terasaki, T. and Pardridge, W.M.: Stereospecificity of
triiodothyronine transport into brain, liver, and salivary gland: role
of carrier- and plasma protein-mediated transport. Endocrinology,
121(3):1185-1191, 1987.
• http://www.kingpharm.com/uploads/pdf_inserts/Cytomel_PI.pdf.
• Mooradian, A.D.: Blood-brain transport of triiodothyronine is
reduced in aged rats. Mech. Ageing Dev., 52(2-3):141-147, 1990.
• Cheng, L.Y., Outterbridge, L.V., Covatta, N.D., et al.: Film
autoradiography identifies unique features of [125I]3,3'5'-
(reverse) triiodothyronine transport from blood to brain. J.
Neurophysiol., 72(1):380-391, 1994.
• Rudas, P. and Bartha, T.: Thyroxine and triiodothyronine uptake
by the brain of chickens. Acta Vet. Hung, 41(3-4):395-408, 1993.
Or: The idiocy of T4 only thyroid treatment…](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-76-2048.jpg)
![Other studies in children
• Endocrine-disrupting chemicals (EDC’s) and perturb
normal levels of hormones required for normal neural
circuit development.
– Three ubiquitous endocrine disruptors studied
[polychlorinated biphenyls, polybrominated diphenyl
esters, and bisphenol A.]
– Impact of these disrupts goes beyond relative
hypothyroidism and affect memory, cognition, and social
behavior.
– Pinson A et al. Andrology. 2016 Jul;4(4):706-22
Louis B. Cady, MD](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-110-2048.jpg)
![Prevalence of thyroid dysfunction and its impact
on cognition in older Mexican adults (SADEM
study)
• 1750 participants evaluated via interviews, TSH, and Free T4 levels.
• TSH of 0.4 – 4 was considered euthyroid.
• Over hypothyroidism = TSH>4.8
• Overt hyperthyroidism – TSH <0.3 IU/L
• Results:
• Overall estimated prevalence of thyroid dysfunction in Mexican
population was 23.7%.
• 15.4% we were classified as subclinical hypothyroidism.
• Thyroid dysfunction and cognitive impairment was most evident
in overt hypothyroidism [OR=1.261]
• Juarez-Decillo T et al. J. Endocrinol Invest. 2017 Mar 25.
Louis B. Cady, MD](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-115-2048.jpg)
![Somatotropic and thyroid hormones in the
acute phase of subarachnoid haemorrhage.
• Complicated hospital course was associated
with a deeper fall in TSH and T3
concentrations.
• “Low concentrations of TSH and T3 were
connected to worse SAH [subarachnoid
haemorrhage] grade and poor outcome.”
–Implications for treatment? No conclusions
given.
–Zetterling M et al. Acta Neurochir (Wien). 2013
Nov;155(11):2053-62.](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-127-2048.jpg)
![Exogenous T3 administration provides
neuroprotection in a murine model of traumatic brain
injury.
• Thyroid hormones noted to be decreased in patients with
brain jury.
• Controlled cortical impact injury (CCI) [widely used
experimentally] was used in adult male mice.
• Tx with T3 (1/2 MICROgrams/100 grams body weight IP)
one hour after TBI resulted in a significant improvement in
motor and cognitive recovery after CCI.
• 24 hours after brain trauma, T3 treated mice showed
significantly lower number of apoptotic neurons.
• T3 significantly enhanced post-TBI expression of BDNF
and GDNF compared to control vehicle.
– Crupi R et al. Pharmacol Res. 2013 Apr;70(1):80-9.](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-128-2048.jpg)
![Multiple hormonal derangements seen as determinant
of cognitive decline in older men
• Thyroid, cortisol, and anobolic hormones [DHEA-S,
testosterone, and IGF-1] noted to decline with age.
• Frailty related to consequences of cognitive
impairment and cognitive decline.
• Correlation with changes of thyroid hormone and
anabolic hormones in older men was found.
– Maggio M et al. J Nutr Health Aging. 2012 Jan;16(1):40-
54.
Louis B. Cady, MD](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-129-2048.jpg)
![• “…levothyroxine replacement therapy with vitamin
E supplementation may ameliorate cognitive deficit
in PTU-induced hypothyroidism [experimental
model of hypothyroidism] through the decrease of
oxidative stress status.”
• Note: BOTH were used.
• Pan T, et al. Endocrine. 2013 Apr;43(2):434-9.](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-133-2048.jpg)
![Louis B. Cady, MD
“subclinical hypothyroidism bipolar disorder” 1/28/2018
43 citations
• “Thyroid abnormalities occur frequently in patients with BD regardless of
treatment.” [Lambert CG et al. Bipolar Disord. 2016 May;18(3):247-60]
• Patients with SCH had poorer performance than patients without SCH in
measures of verbal memory, attention, language, and executive functions.
[Martino DJ, et al. Subclinical hypothyroidism and neurocognitive
functioning in bipolar disorder. J Psychiatr Res. 2015 Feb;61:166-7]
• “There is no significant association between hypothyroidism and bipolar
disorder.” Menon B. Hypothyroidism and bipolar affective disorder: is
there a connection. Indian J. Psychol Med. 2014 Apr;36(2):125-8
• Hypothyroidism, either overt or more commonly subclinical, appears to the
commonest abnormality found in bipolar disorder. Chakrabarti S. Thyroid
functions and bipolar affective disorder. J Thyroid Res. 2011;2011;
2011:306367.](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-143-2048.jpg)
![As of August 21, 2016
NEW LITERATURE – AUGUST 2016 – “Association between serum
thyrotopin levels and mortality among euthyroid adults in the
United States. [Inoue K et al. Thyroid. 2016 Aug 18 [Epub ahead of print]
• Population – NHANES III study . N = 12,584 adults>/= 20 years of
age.
• Associations between TSH tertiles (high, medium, and low)
and mortalities (all cause, cardiovascular and cancer)
• Mean followup = 19.1 years with 3,395 deaths.
• Increase risk of all-cause mortality found in high normal TSH
compared to medium normal TSH group. ( Low normal
compared to medium also had higher all cause mortality).
• “This study indicated that the normal range of TSH levels may
require reevaluation.”
Louis B. Cady, MD](https://image.slidesharecdn.com/cadythyroidpresentationforimmh2018-180908180520/75/THE-THYROID-AXIS-FROM-A-TO-Z-145-2048.jpg)

This document provides an overview of a lecture on thyroid health. It begins with the speaker, Louis Cady, MD, disclosing commercial relationships and interests. It then outlines the structure of the lecture, which will cover thyroid basics, practical information, and conclusions. The document discusses conventional thyroid testing and its limitations. It also reviews factors that affect thyroid hormone production and conversion. Overall, the document introduces topics to be covered in the lecture regarding thyroid function and testing.