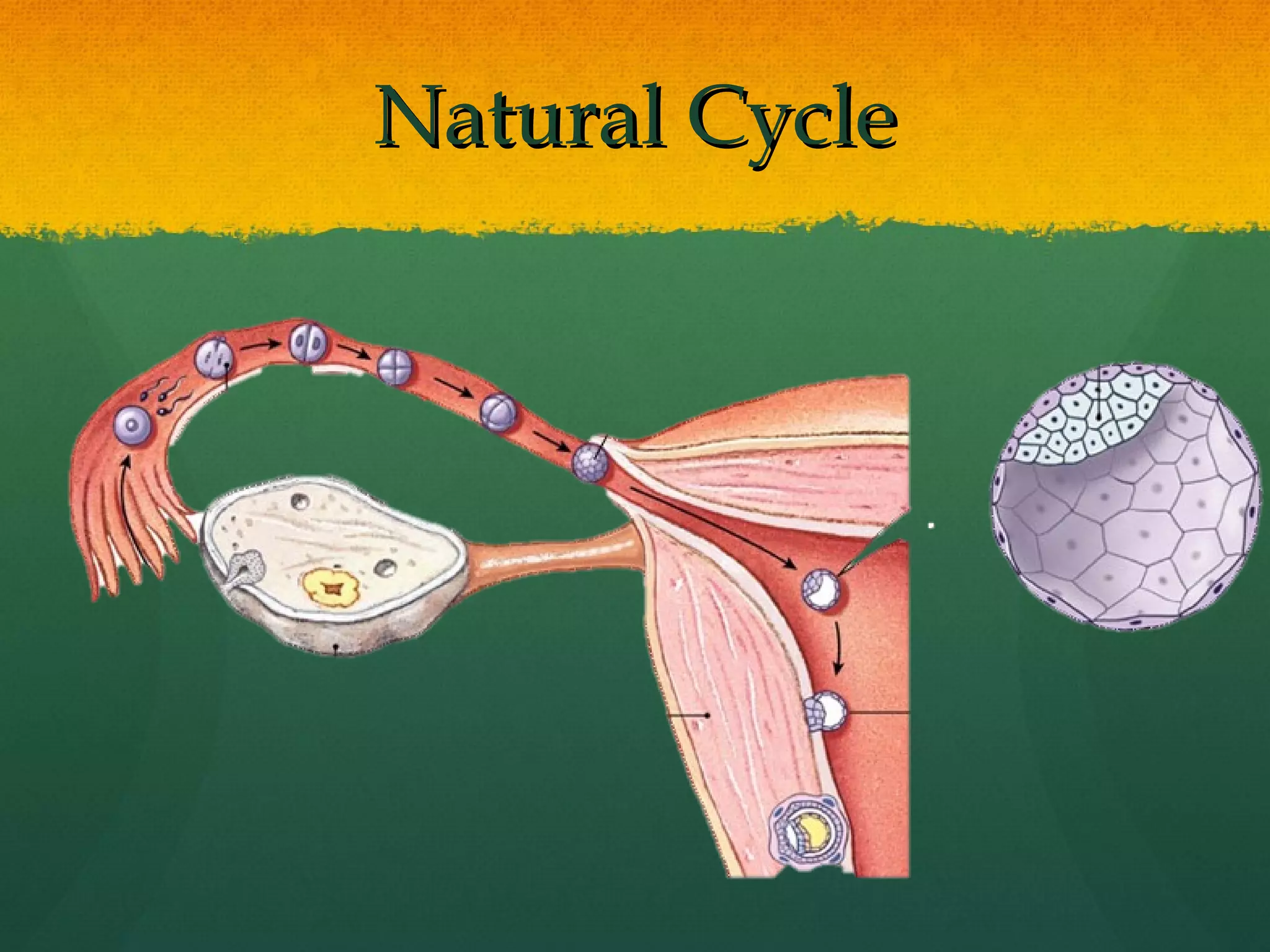
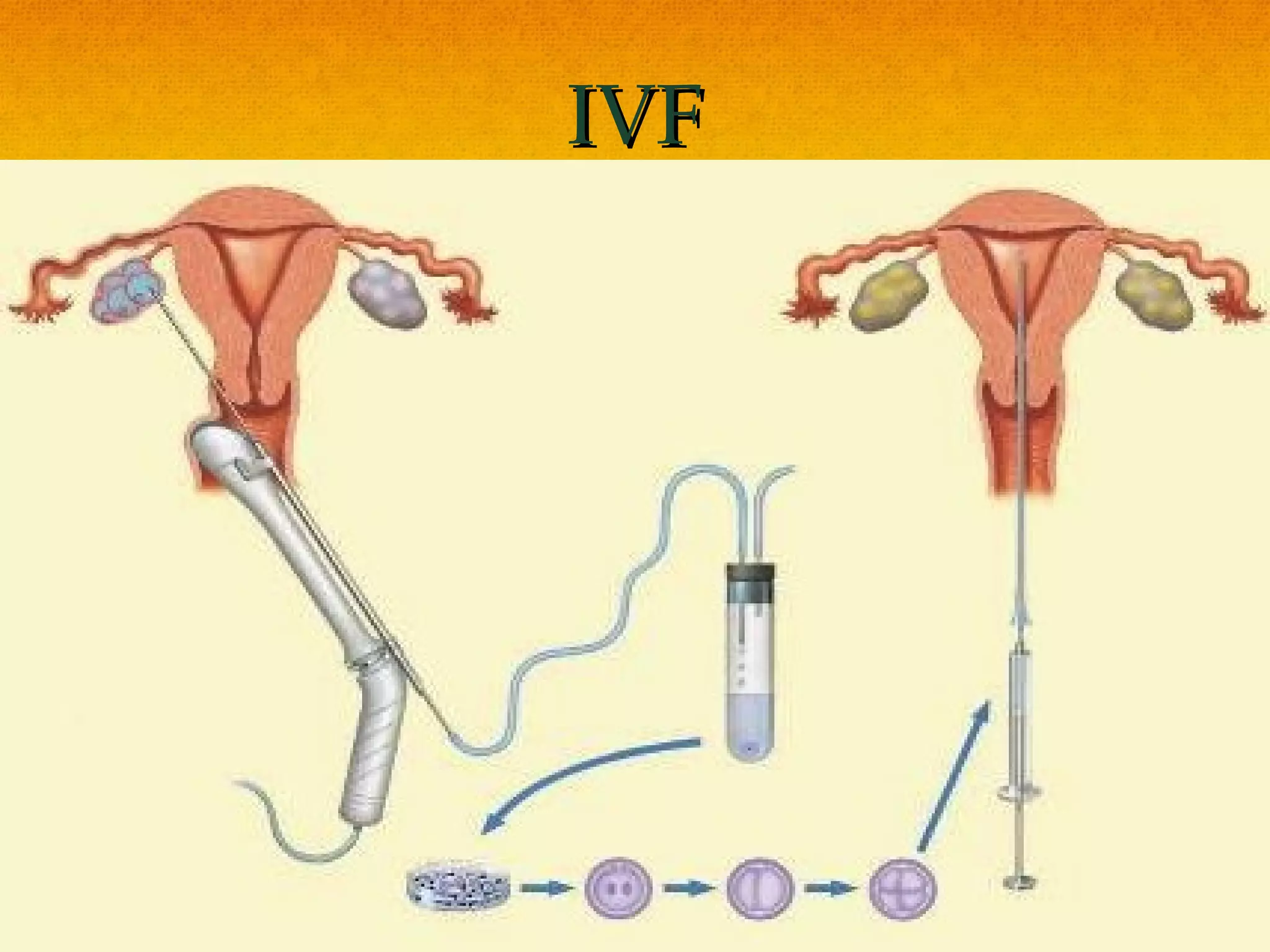


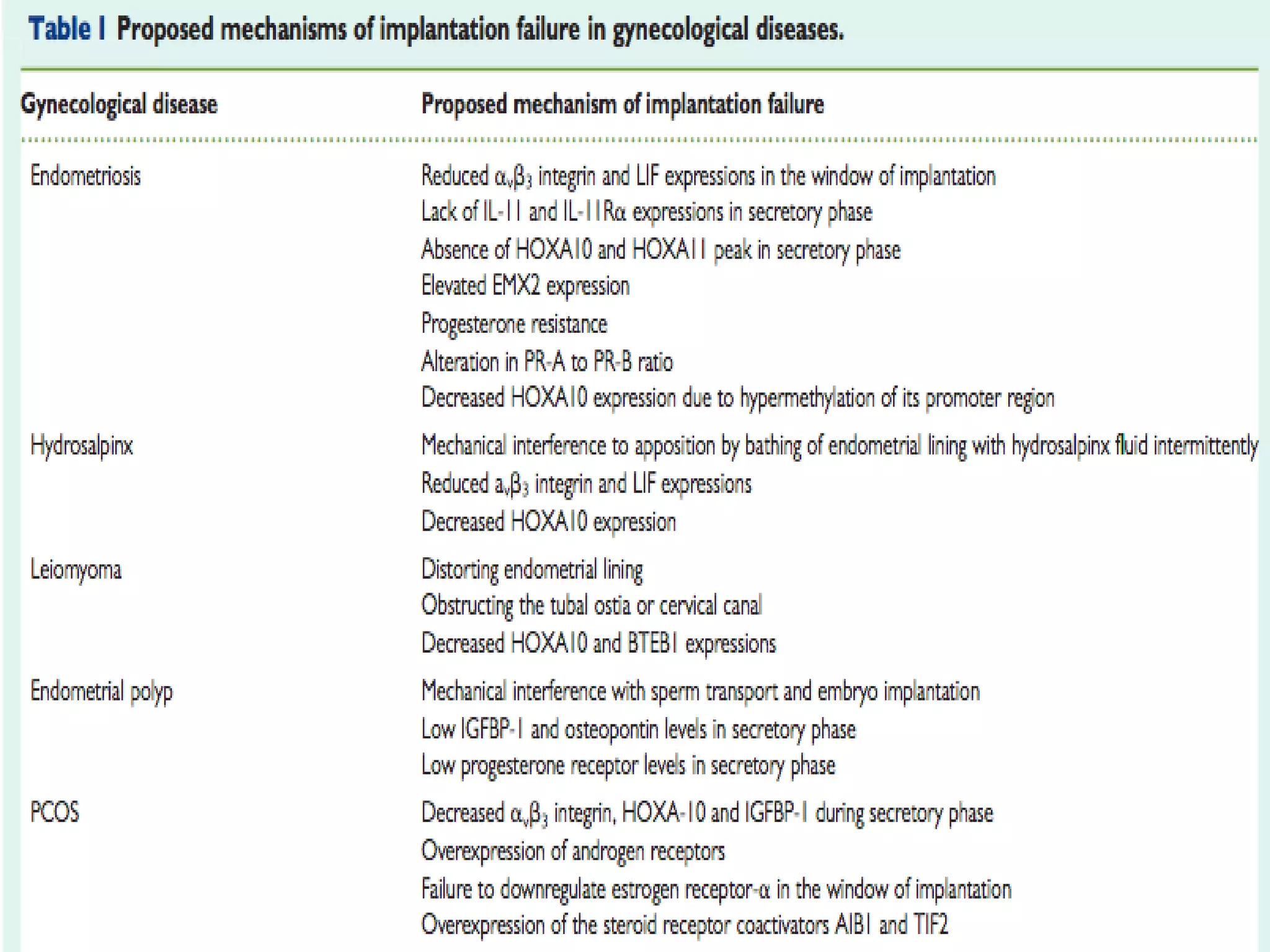


Dr. Priya Chittawar discusses the challenges and complexities of implantation in IVF, noting that 60% of cycles don't result in pregnancy despite improved techniques. Key factors affecting implantation include the quality of embryos, endometrial receptivity, and hormonal interactions, with a significant portion of conceptus lost before implantation. Future advancements may focus on better assessment of endometrial conditions and potential gene therapies to enhance implantation success rates.









































































