Downloaded 33 times
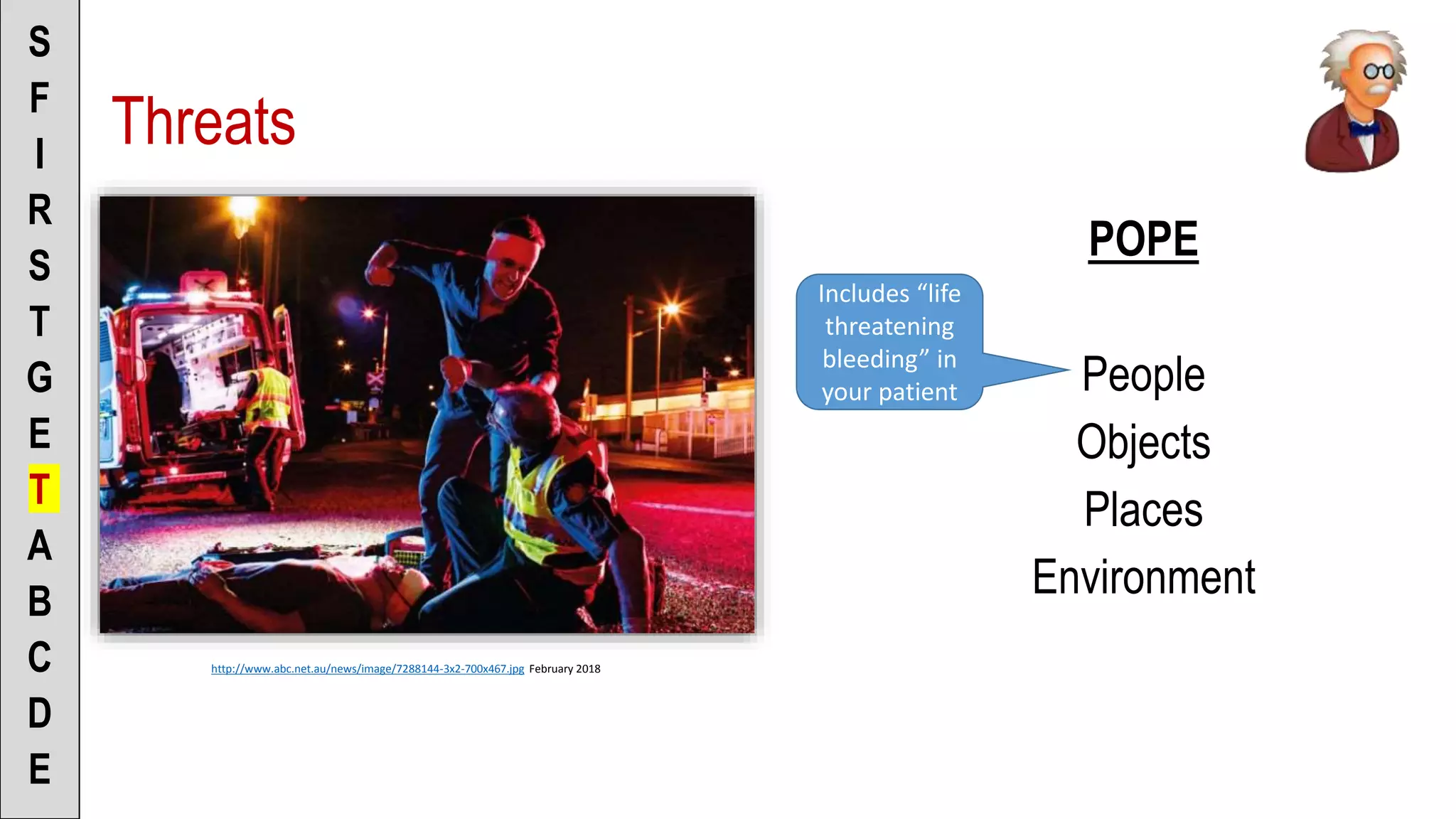
![To the Scenario Director
• “I don’t see anything that makes me
feel unsafe”
[or]
• “I’m concerned about ______ and
would address that by ______
before entering the scene”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
Fear](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-11-2048.jpg)
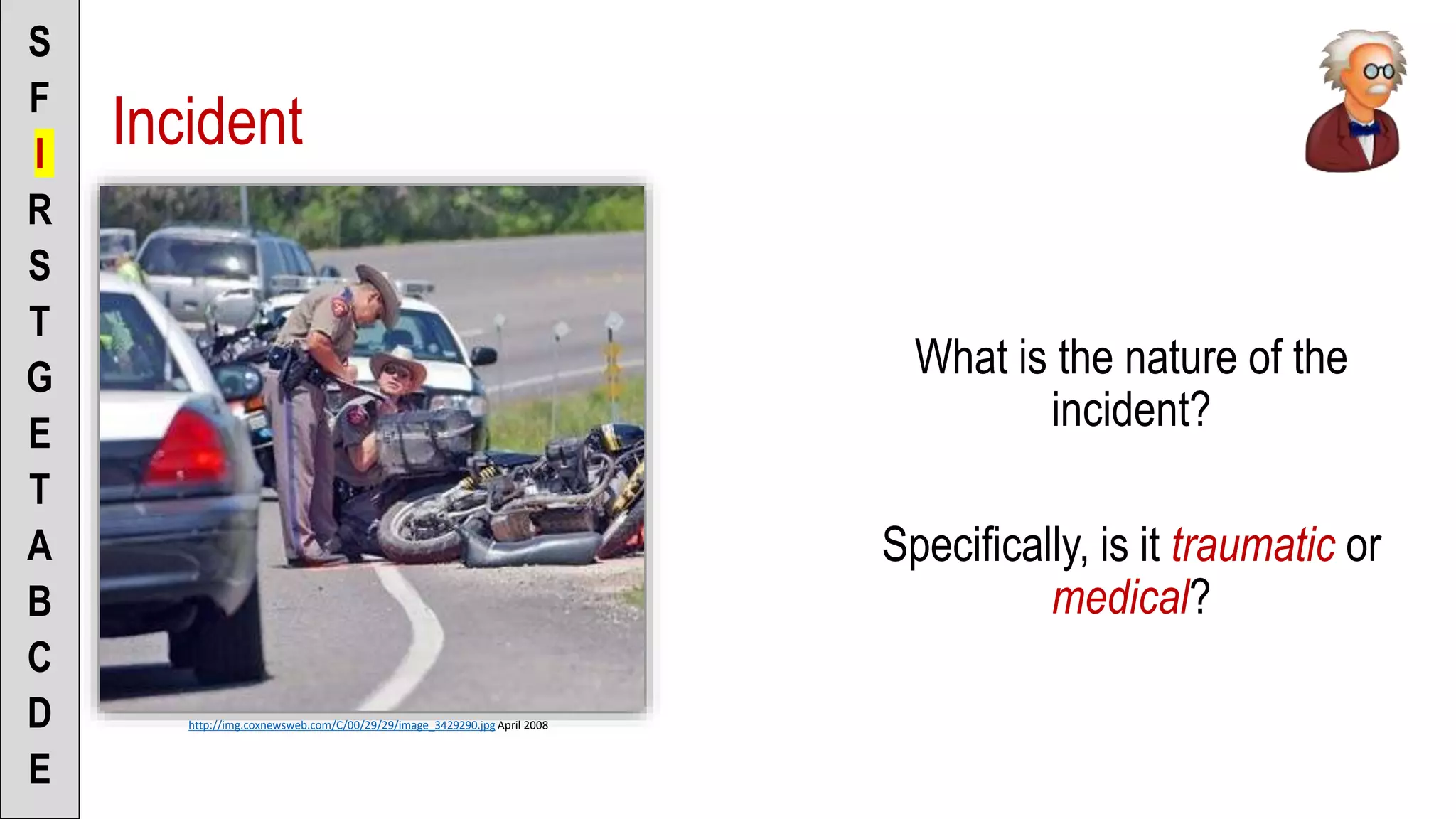
![To the Scenario Director
• “This seems to be a traumatic/non-
traumatic incident” (pick one)
• “I’m considering the mechanism of
injury”
[or]
• “I’m considering the nature of illness”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
Incident](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-14-2048.jpg)
![To the Scenario Director
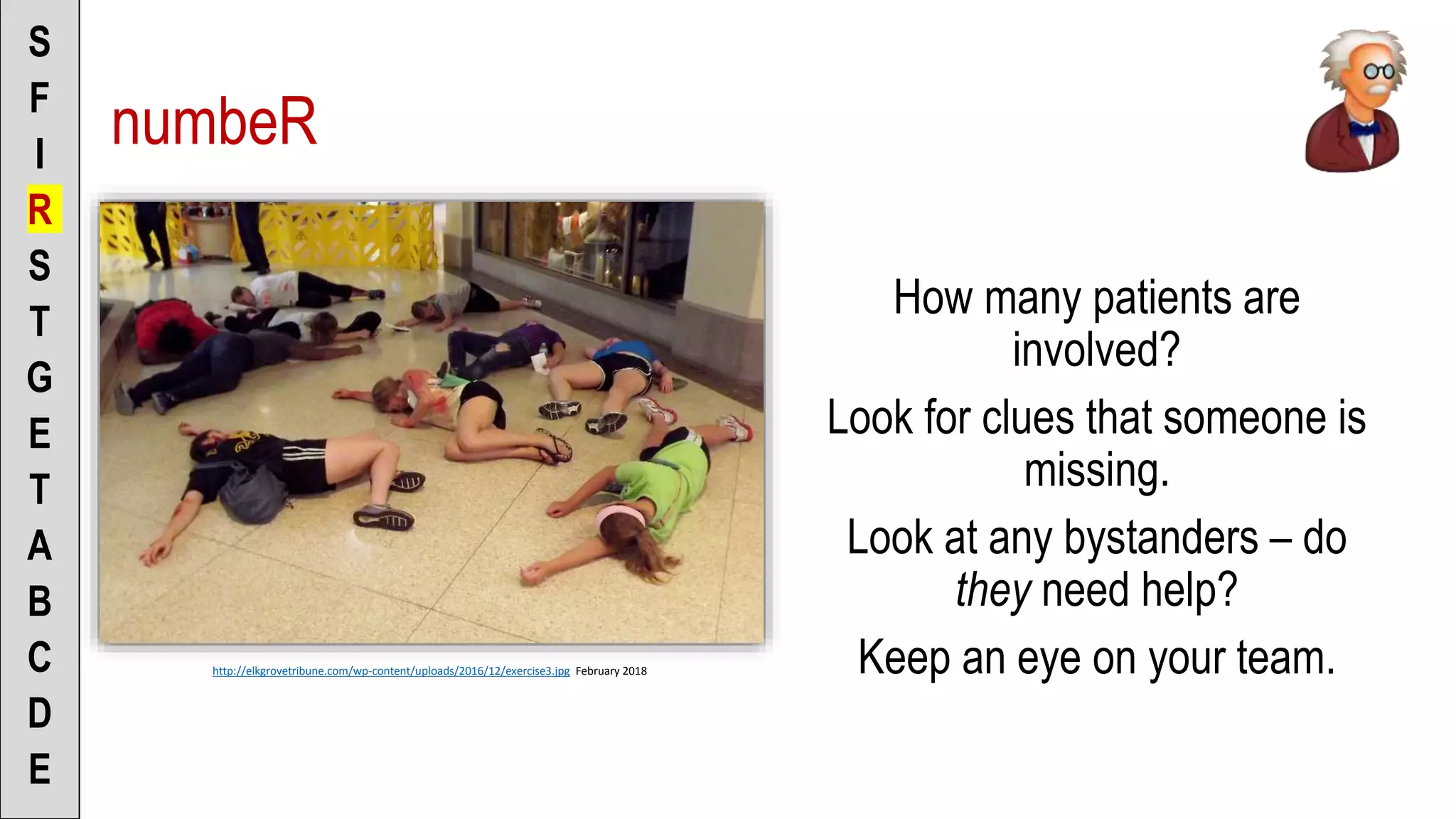
• “There appears to be only one
patient”
[or]
• “I see more than one patient, there
are ______ patients”
• “I see one patient is there anyone
else I need to be concerned about”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
numbeR](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-17-2048.jpg)
![To the Scenario Director
• “No need to send for help at this
point”
[or]
• “I’m going to request ______ for help
because of ______”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
Send for help](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-20-2048.jpg)
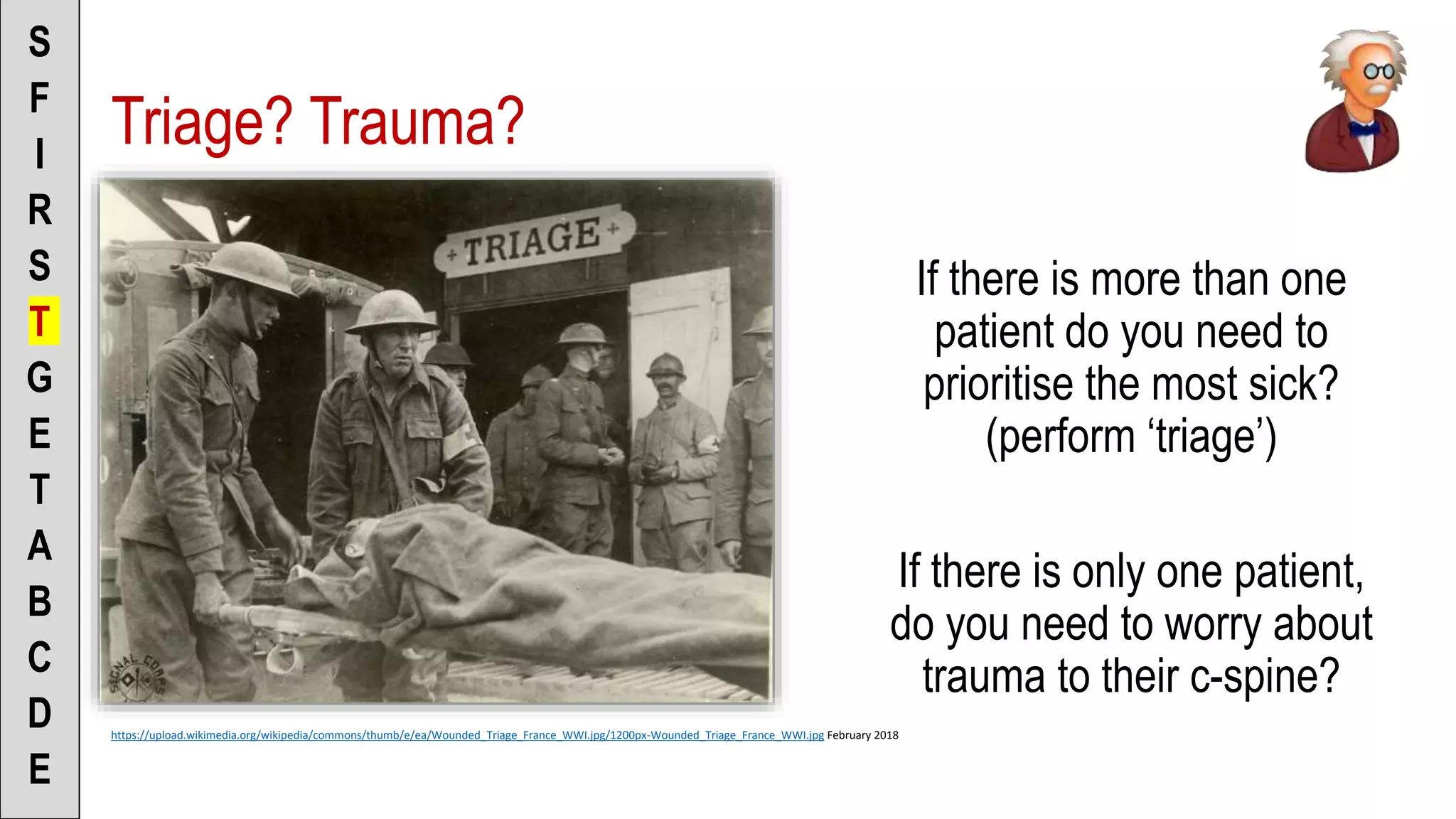
![To the Scenario Director
• “I’m ruling in C-spine – partner can you
immobilise”
[or]
• “I’m ruling out C-spine – no need to
immobilise”
• “There’s only 1 patient so no need to
triage”
[or]
• “There are multiple patients so I will begin
triaging”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
Triage? Trauma?](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-23-2048.jpg)
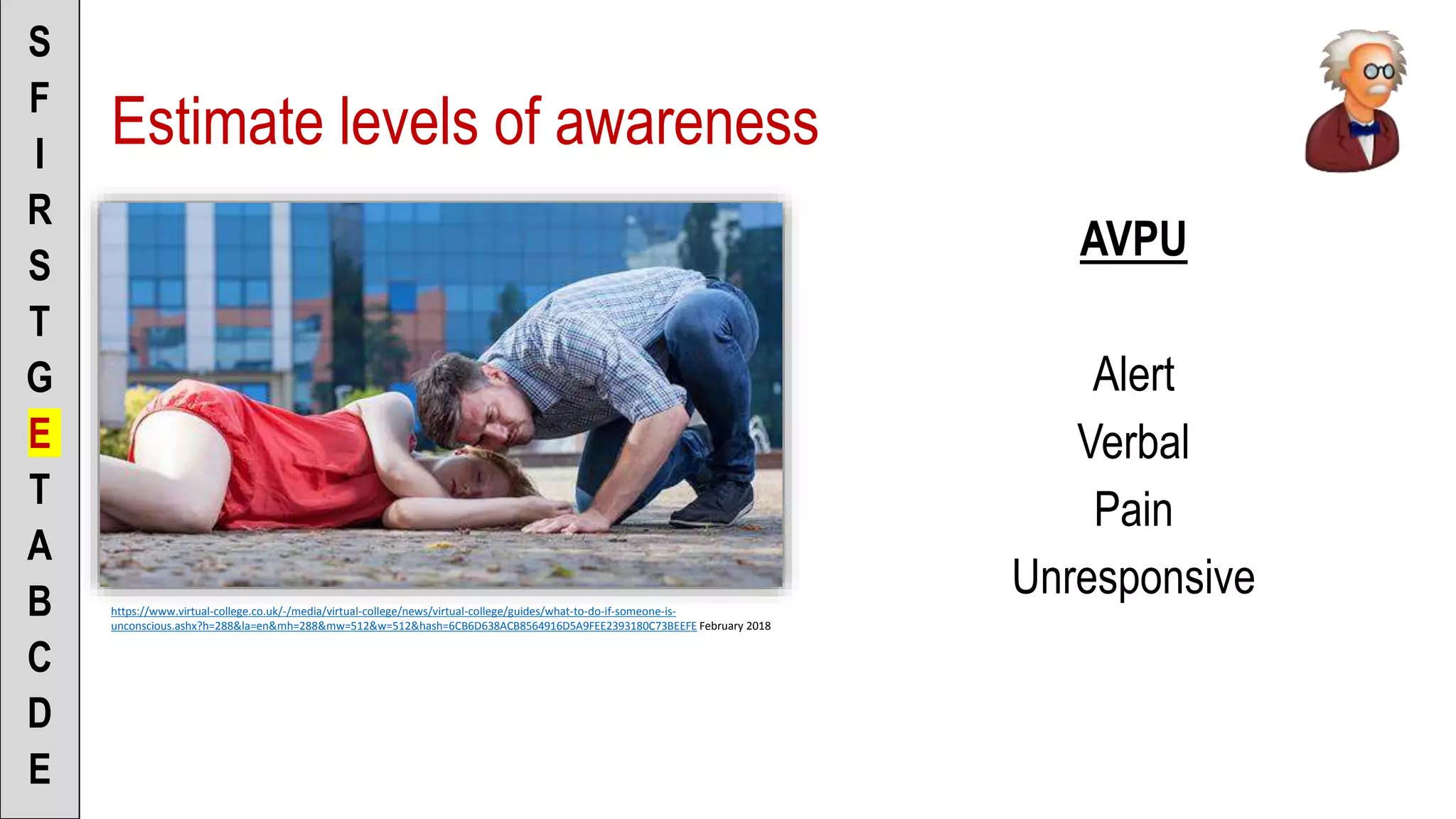
![To the Scenario Director
• “The patient appears to be alert, is
visually tracking me, and is responding
to verbal with normal verbal” [or]
• “Patient is responding to loud verbal by
moaning” [or]
• “Patient is responding to pain by …” [or]
• “Patient is responding to _____ by
_____”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
• “Hi, my name is ______ and I’m a
paramedic, are you ok?”
Estimate LOA’s](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-31-2048.jpg)
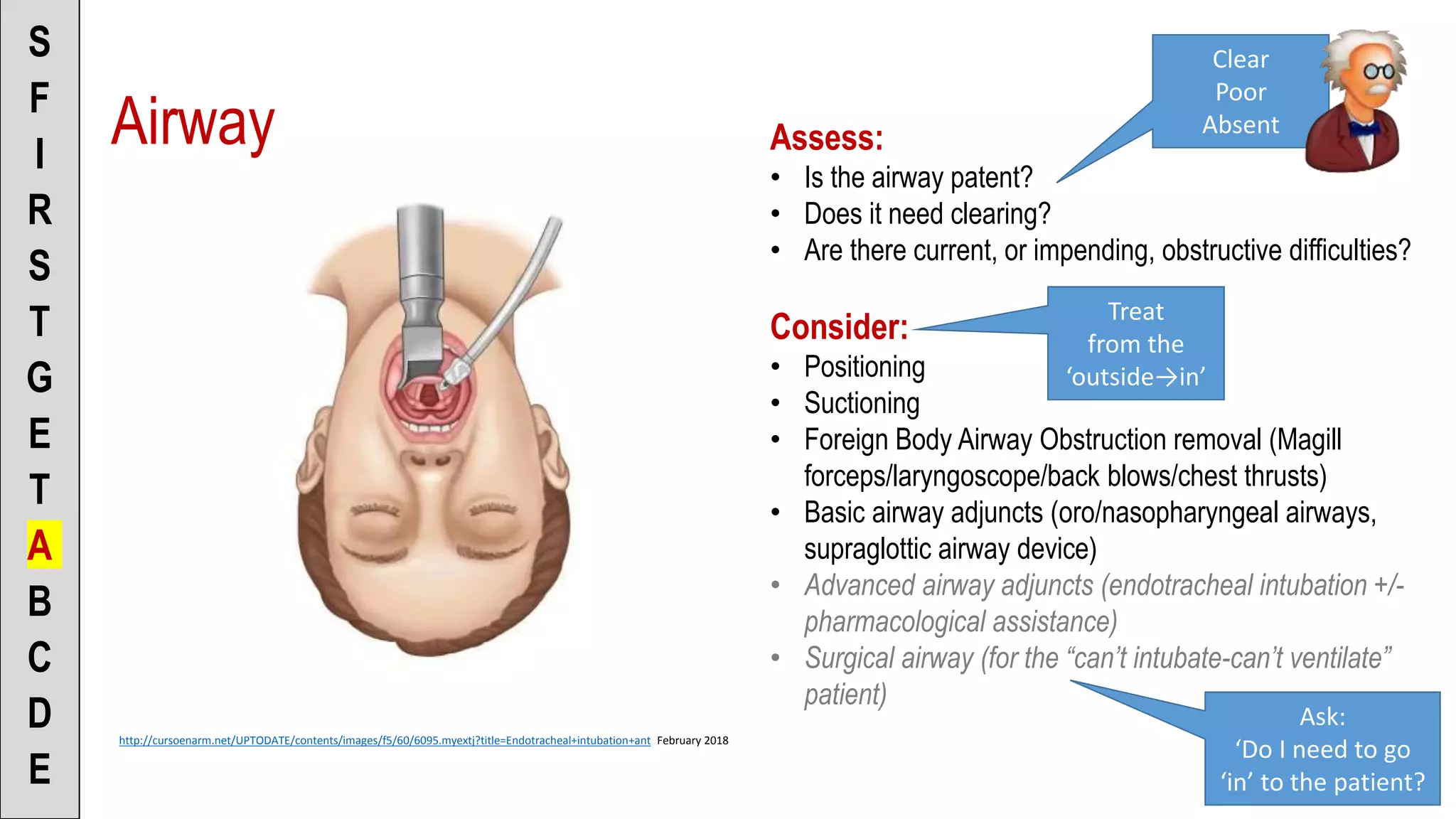
![To the Scenario Director
• “Airway is clear/poor/absent”
• “I’m going to attempt to ventilate the
patient to see if the airway is clear”
[or]
• “Patient does/does-not require
advanced airway support”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
• “How’s your breathing, is it ok?”
• Explain to the patient what you are
doing
• (Be sure to get consent!)
Airway](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-37-2048.jpg)
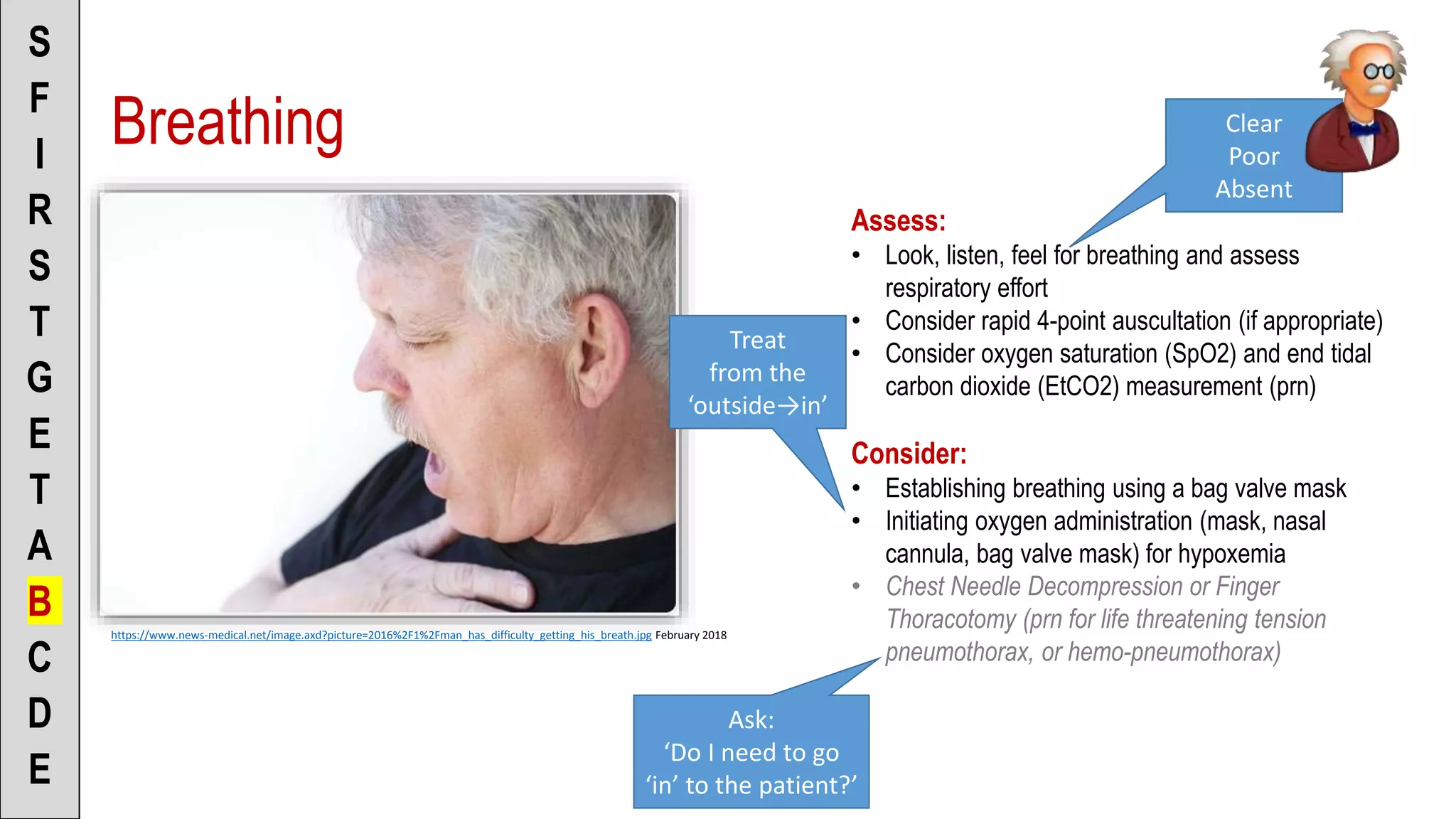
![To the Scenario Director
• “Patient’s breathing is
clear/poor/absent”
• “I’m going to apply a non-rebreather
mask @ 15L per minute” [or]
• “I’m going to apply a nasal cannula
@ 2L per minute” [or]
• “I’m going to ventilate with a BVM”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
• Explain to the patient what you are
doing
• (Be sure to get consent!)
Breathing](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-40-2048.jpg)
![To the Scenario Director
• “There is a strong radial/carotid
pulse” [or]
• “There is no carotid pulse”
• “Patient appears well/poorly
perfused”
• “Skin is pink (pale, mottled), warm
(cool, cold) and dry (clammy, wet)”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
• Explain to the patient what you are
doing
• (Be sure to get consent!)
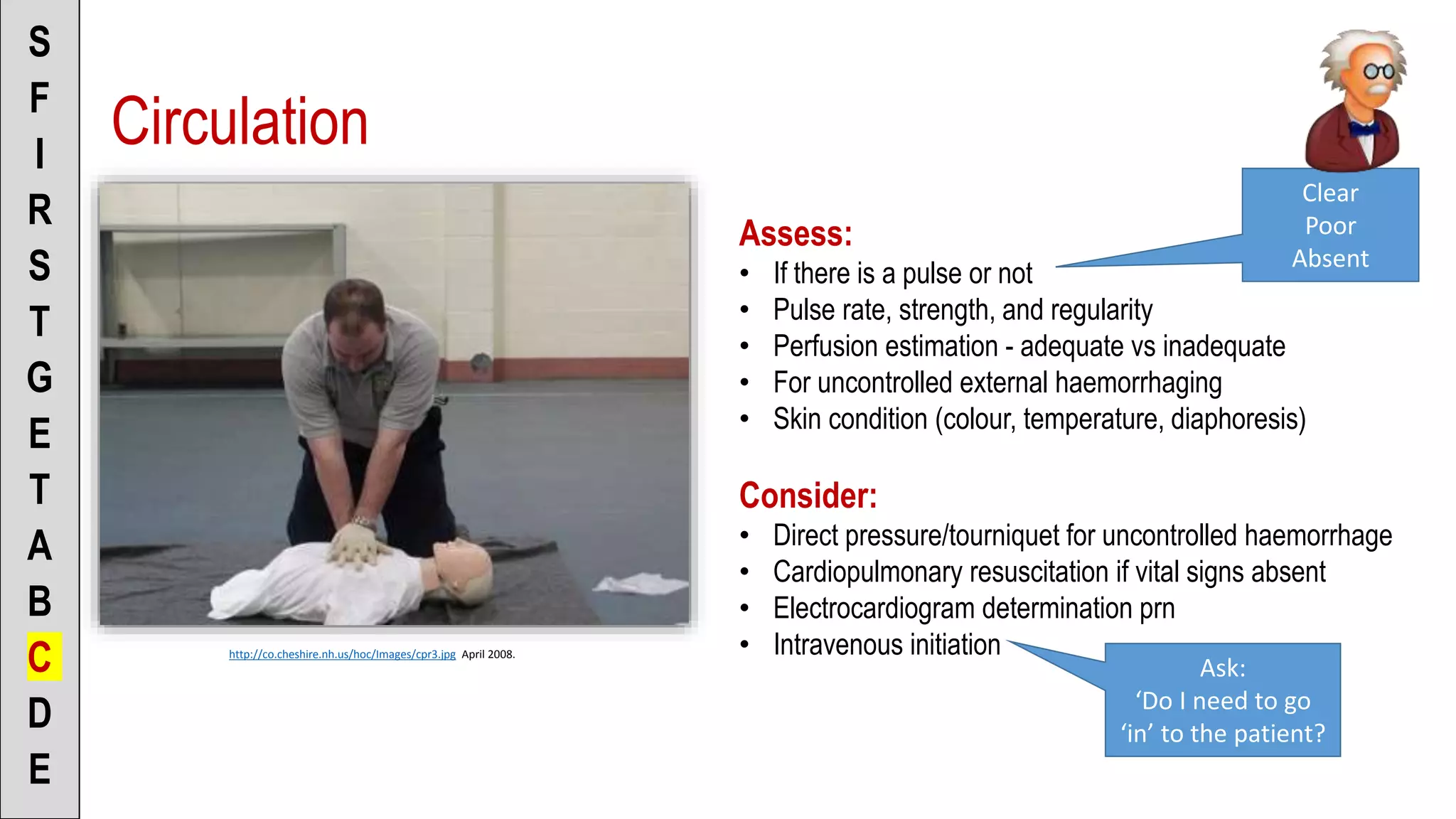
Circulation](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-43-2048.jpg)

![To the Scenario Director
• “I’m assessing for medical disabilities”
• “No treatment required at this point” [or]
• “I want to give Midazolam for seizures” [or]
• “I want to give Adrenaline for anaphylaxis”
[or]
• “I want to give Narcan for opioid overdose”
[or]
• “I want to give Glucose/Glucagon for
hypoglycaemia”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
• Explain to the patient what you are doing
• (Be sure to get consent!)
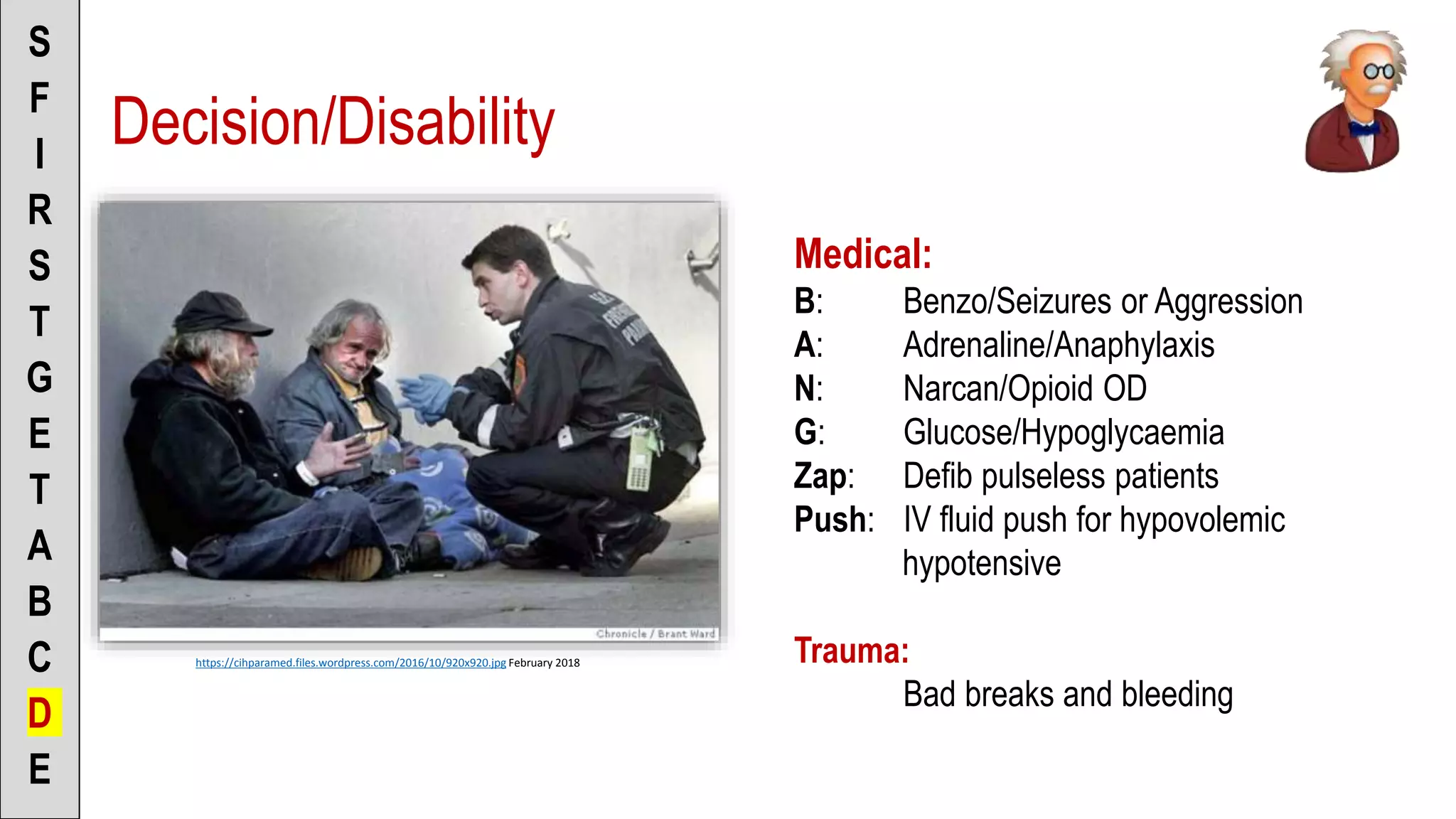
Decision: Medical](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-46-2048.jpg)
![To the Scenario Director
• “I’m assessing for trauma disabilities”
• “The patient has an uncontrolled bleed/or
break – this is a load and go situation” [or]
• “Patient appears to be stable”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
• Explain to the patient what you are doing
• (Be sure to get consent!)
Decision: Trauma](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-47-2048.jpg)
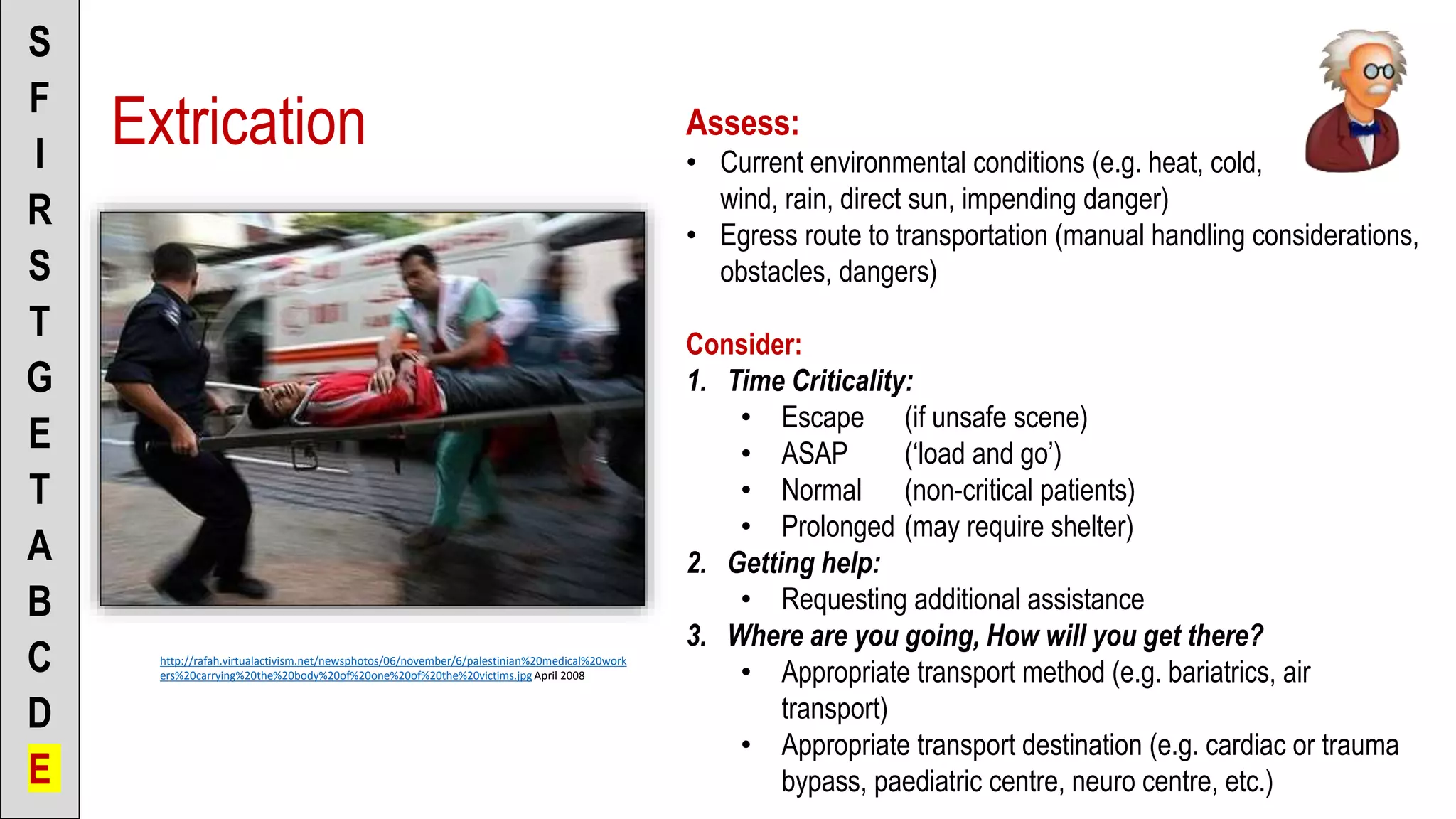
![To the Scenario Director
• “This patient requires immediate extrication”
[or]
• “This patient is a load and go” [or]
• “This patient can be extricated normally” [or]
• “This is going to be a prolonged extrication,
and I’m going to consider _____”
• “I’m going to request _______ to assist in
extrication”
• “I’m going to request _______ to assist in
patient care”
• “I’m going to request _______ for transport”
• “I’m going to transport the patient to _____”
S
F
I
R
S
T
G
E
T
A
B
C
D
E
To the Patient
• Explain to the patient what you are doing
• (Be sure to get consent!)
Extrication](https://image.slidesharecdn.com/teachingtheipps-primary-190313052200/75/Teaching-the-IPPSS-Primary-50-2048.jpg)


The document outlines the creation of evidence-based primary and secondary surveys for paramedicine, stemming from a systematic review by an international team of experts. It includes mnemonics for paramedic students to simplify the learning process, emphasizing safety and sequential assessment. The content focuses on practical applications and structured assessments that paramedics should perform in various emergency scenarios.















































