Download to read offline

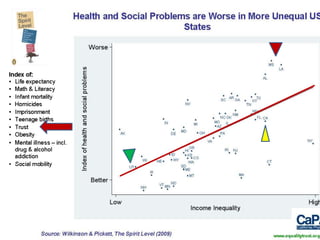
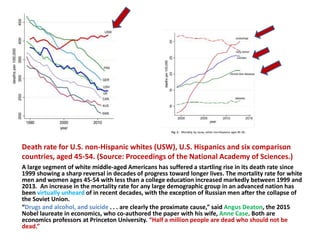
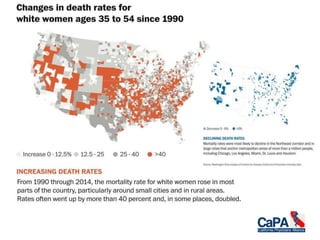
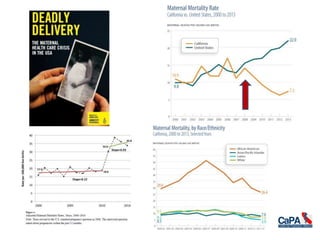
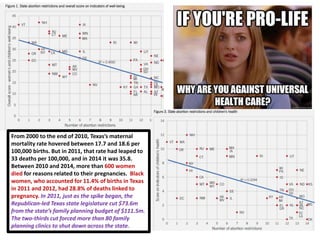


The document discusses the implications of the Affordable Care Act (ACA) and the recent threats to it posed by the Trump administration and Republican lawmakers, highlighting potential increases in uninsured rates and rising healthcare costs. It notes alarming trends in life expectancy related to income disparities and a significant rise in mortality rates among middle-aged white Americans, primarily due to substance abuse and suicide. Additionally, it details how the ACA expanded healthcare access and reduced bankruptcy rates due to medical expenses, contrasting it with the proposed American Health Care Act (AHCA) that could reverse these gains.



































































