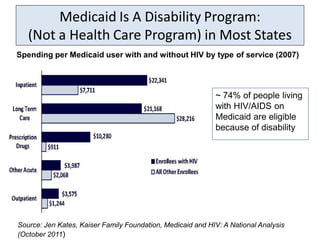
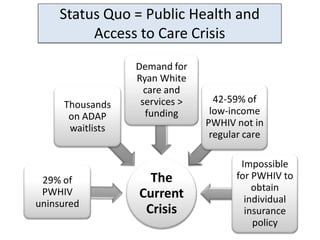
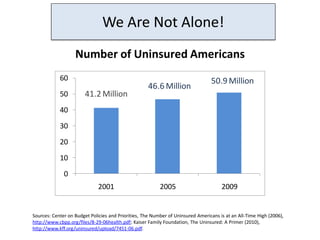
The document discusses health care reform opportunities and challenges for people living with HIV/AIDS. It outlines the current access to care crisis, including high rates of uninsured individuals with HIV/AIDS and limited Medicaid access in most states. It then describes major opportunities created by health care reform, such as expanded Medicaid eligibility, enhanced Medicaid care coordination, increased access to Medicare prescription drugs, private insurance market reforms, and new investments in prevention and care delivery. Finally, it discusses key challenges in ensuring these opportunities translate into real benefits for people with HIV/AIDS.




![Know the Facts: Health Care Reform Will
Reduce the Federal Deficit
Federal v. State Share of From the Congressional
Medicaid Expansion Budget Office and the Joint
Committee on Taxation:
“The effects . . . [of health care
reform] on direct spending and
revenues related to health care
will reduce federal deficits by
$210 billion over the 2012-2021
period.”
Sources: Center on Budget Policies and Priorities, Hatch-Upton Report on Costs to States of Expanding Medicaid Relies on
Seriously Flawed Estimates (2011), http://www.cbpp.org/files/3-16-11health.pdf.
Congressional Budget Office , CBO’s Analysis of the Major Health Care Legislation Enacted in March 2010, (March 2011),
http://www.cbo.gov/ftpdocs/121xx/doc12119/03-30-HealthCareLegislation.pdf](https://image.slidesharecdn.com/syncingchronicdiseaseadvocacygreewald-120501105052-phpapp01/85/Syn-cing-chronic-disease-advocacy-greewald-35-320.jpg)