
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to PD ADEQUACY
Similar to PD ADEQUACY (20)
Recently uploaded
Recently uploaded (20)
PD ADEQUACY
- 1. DOI: 10.1510/icvts.2007.165118 2007; 2008;7:116-120; originally published online Nov 30,Interact CardioVasc Thorac Surg Giorni, Luca Di Chiara and Sergio Picardo Zaccaria Ricci, Stefano Morelli, Claudio Ronco, Angelo Polito, Giulia V. Stazi, Chiara surgery Inotropic support and peritoneal dialysis adequacy in neonates after cardiac http://icvts.ctsnetjournals.org/cgi/content/full/7/1/116 located on the World Wide Web at: The online version of this article, along with updated information and services, is 1569-9293. (ESCVS). Copyright © 2008 by European Association for Cardio-thoracic Surgery. Print ISSN: for Cardio-thoracic Surgery (EACTS) and the European Society for Cardiovascular Surgery is the official journal of the European AssociationInteractive Cardiovascular and Thoracic Surgery by on August 20, 2008icvts.ctsnetjournals.orgDownloaded from
- 2. ARTICLE IN PRESS www.icvts.org doi:10.1510/icvts.2007.165118 Interactive CardioVascular and Thoracic Surgery 7 (2008) 116–120 ᮊ 2008 Published by European Association for Cardio-Thoracic Surgery Institutional report - Congenital Inotropic support and peritoneal dialysis adequacy in neonates after cardiac surgery Zaccaria Ricci *, Stefano Morelli , Claudio Ronco , Angelo Polito , Giulia V. Stazi , Chiara Giorni ,a, a b a a a Luca Di Chiara , Sergio Picardoa a Department of Pediatric Cardiology and Cardiac Surgery, Bambino Gesu` Hospital, Piazza S.Onofrio, 00100, Rome, Italya Department of Nephrology Dialysis and Transplantation, St Bortolo Hospital, Vicenza, Italyb Received 15 August 2007; received in revised form 12 November 2007; accepted 14 November 2007 Abstract We describe the impact of cardiovascular pharmacologic support on peritoneal dialysis adequacy in 20 neonates who required postoperative renal replacement therapy following cardiopulmonary bypass exposure. Peritoneal dialysis was administered for 2.5 (2) days. Peritoneal dialysis creatinine clearance was 3.4 (2.1) mlyminy1.73 m and ultrafiltration rate was 9.75 (10) mlyh. Residual creatinine clearance was2 31 (26) mlyminy1.73 m . Peritoneal dialysis creatinine clearance appeared to be a function of dialysate flow up to 100 mlyh. No correlation2 was present between inotropes and vasopressors infusion and peritoneal dialysis creatinine clearanceyultrafiltration rate. LDH clearance was 0.59 (0.85) mlyminy1.73 m and it did not appear to have a correlation with dialysate flow. Patients in-hospital mortality was 20%,2 significantly higher than overall neonatal population admitted to our ICU (4.8%, Ps0.02). Peritoneal dialysis in neonates allows optimal ultrafiltration rate and adequate small solute clearance, irrespective of hemodynamic status or vasopressor support. ᮊ 2008 Published by European Association for Cardio-Thoracic Surgery. All rights reserved. Keywords: Peritoneal dialysis; Inotropic score; Congenital heart disease; Acute kidney injury 1. Introduction Renal replacement therapy (RRT) is delivered in up to 10% of children undergoing cardiac surgery for correction of congenital heart disease and is associated with an increased mortality rate w1–3x. Cardiopulmonary bypass (CPB) and low flow states likely contribute to the devel- opment of acute kidney injury (AKI) w4, 5x. Even in the absence of evident signs of renal dysfunction, a clinical condition of fluid retention and generalized edema is common in neonates after major cardiosurgical interven- tions w3x. While various therapeutic options are available, early peritoneal dialysis (PD) administration is the treat- ment of choice for these patients in many centers w2x. Optimization of fluid balance is primarily targeted by PD initiation. Nonetheless, clearance of nitrogenous waste products and other solutes is also likely to be important in children who develop AKI. Efficiency of PD in the immediate postoperative period following CPB, however, may be affected by several factors: small dialysate exchange vol- umes are often prescribed and delivered in order to mini- mize hemodynamic derangements, excessive abdominal pressure rise and leakage of abdominal catheters w6x. Fur- thermore, blood flow to the peritoneum may be reduced secondary to diminished cardiac output, high vasopressors dose, changes in vascular resistance, or capillary leak w6x. *Corresponding author. Tel.: q39 06 6859 3333. E-mail address: zaccaria.ricci@fastwebnet.it (Z. Ricci). PD is currently accepted as a feasible, safe and effective therapy but information on clearance and ultrafiltration patterns during PD in this specific subset of patients are missing. This study aimed to describe the impact of hemo- dynamic pharmacologic support on PD adequacy in neonates who require postoperative PD following CPB exposure. 2. Materials and methods 2.1. Study protocol We conducted a prospective observational study on a cohort of 20 consecutive neonates who received postoper- ative PD after cardiac surgery requiring CPB. Indications to PD were the presence of oliguria (defined as urine output -0.5 mlykgyh for more than 4 h) andyor generalized ede- ma with need for supplementary ultrafiltration. At the time of enrollment, demographic and clinical data (age, sex, body surface area, primary diagnosis, surgery, duration of CPB) were collected (Table 1). Cycling peritoneal dialysis was performed in all subjects using a cuffed Tenckhoff catheter. A fixed exchange volume of 10 mlykg was always infused. Dwell and drainage times varied depending on patients needs. Hence, final dialysate flow (hourly Qd: exchange volume=number of exchanges per hour) was exclusive function of dwell and drainage times and not of volume infused per cycle. Dialysis fluid glucose concentra- tion (ATC B05DA, AIC Baxter SpA, Rome, Italy) was 1.35%. by on August 20, 2008icvts.ctsnetjournals.orgDownloaded from
- 3. ARTICLE IN PRESS 117Z. Ricci et al. / Interactive CardioVascular and Thoracic Surgery 7 (2008) 116–120 Table 1 Demographic and clinical data of enrolled patients Age (days) Sex BSA (m )2 Diagnosis CPByX clamp (min) Surgical procedure INM 23 M 0.190 DORVqPValveStqTAPVR 115 S-P shunt No 12 F 0.198 AAI type B 180 Correction Yes 16 F 0.198 TGA 440 Correction No 10 F 0.134 AAI type B 120 Correction No 19 F 0.134 AAI type B 140 Correction No 4 M 0.149 AoCo 120* Coartectomy Yes 30 M 0.198 AoCoqSubAoStqMitralRing 258 Ross-KonnoqMVS No 25 M 0.195 AoCo 18* Coartectomy Yes 2 M 0.198 TAPVRqAoCo 100 Correction No 2 M 0.168 PAqVSD 120 Correction No 26 M 0.226 Tetralogy of Fallot 212 Correction No 8 M 0.204 PAqIAS 60 OPqBT-shunt dx No 24 M 0.198 TGAqIAS 270 ASO No 19 F 0.190 TGAqVSD 330 ASOqclosure of VSD No 30 F 0.184 cAVC type A 230 Correction No 23 M 0.180 Tetralogy of Fallot 195 Correction No 5 F 0.190 HLHS 270 Norwood-Sano Yes 25 M 0.195 AoCo 28* Aortoplasty No 26 M 0.226 Tetralogy of Fallot 212 Correction Yes 30 M 0.180 Tetralogy of Fallot 98 Correction No BSA, body surface area; CPB, cardiopulmonary bypass; *, cross-clamp time; M, male; F, female; DORV, double outlet right ventricle; PvalveSt, pulmonary valve stenosis; TAPVR, total anomalous pulmonary venous return; S-P, systemic to pulmonary; AAI, aortic arch interruption; TGA, transposition of the great arteries; AoCo, aortic coactation; SubAoSt, subaortic stenosis. PA, pulmonary artery; VDS, ventricular septal defect; IAS, intact atrial septum; OPqBT-shunt, outflow patch and Blalock Taussig shunt; ASO, arterial switch operation; CAVC, common atrioventricular canal; HLHS, hypoplastic left heart syndrome; INM, in-hospital mortality. After the institution of PD and every 24 h for a period of three days a simultaneous sample of blood and 6 h PD drainage were analyzed locally for creatinine, lactic dehy- drogenase (LDH), sodium, potassium, glucose and lactates. These solutes were selected among those routinely avail- able in our laboratory. Six-hour urine collection was also analyzed for creatinine clearance in patients with residual renal function. Mean arterial pressure, heart rate, vaso- pressors dose, diuretics, ultrafiltration rate, fluid balance and significant clinical events occurring during the study period were recorded. Duration of PD, length of intensive care unit stay and out of hospital mortality were also documented. The Institutional Review Board of Bambino Gesu` Hospital approved the protocol and waived the need for consent from patient parents because of the observa- tional nature of the study. 2.2. Measurements Body surface area (BSA) was determined using duBois formula as follows: BSA m s0.007184=wt =ht .2 0.425 0.725 PD solute clearance was calculated by multiplying a 6 h dialysate volume by the ratio between solute concentration in dialysate and plasma (DyP ). Residual creatinine clear-solute ance was calculated when present multiplying 6 h urine volume (simultaneous to dialysate collection) by the ratio between creatinine concentration in urine and plasma. The period of 6 h was selected in order to include periods with constant hemodynamic parameters and drug infusions that could occur over a broader time. Clearances were always indexed to 1.73 m .2 Inotropic score (IS) was calculated as previously described w7x: dopamine mgykgymin=1qdobutamine mgykgymin=1q milrinone mgykgymin=15qepinephrine mgykgymin=100. IS is represented by a wide range of values indicating different inotropic and vasopressor drug regimens. In the absence of other direct instrumental measures of cardiac performance, that are not currently available for neonates, different ISs correlate with different dosages of vasoactive drugs indirectly indicating different cardiac output states. In order to compare subgroups subjected to different ISs, we stratified patients into three pre determined categories: low IS (value -20), intermediate IS (value between 21 and 30), high IS (value over 31). A further stratification was obtained dividing patients in low Qd (30–40 mlyh), inter- mediate Qd (60–75 mlyh) and high Qd (90–120 mlyh). 2.3. Statistical analysis All data are expressed as mean (S.D.). One-way analysis of variance was utilized for analysis of hemodynamic par- ameters among the three IS categories. Two-way analysis of variance with Qd and IS as sources of variation was utilized to show the impact of these parameters on solute clearances and ultrafiltration. Wilcoxon signed rank test was utilized to compare groups where appropriate. Spear- man test was used for correlations. A P-value -0.05 was considered significant. 3. Results Twenty consecutive neonates who underwent post CPB PD were considered eligible and no one was excluded from the protocol. Indication to RRT was oliguria in 13 cases and generalized edema with need for supplementary ultrafiltra- tion in seven patients. In all cases AKI developed after by on August 20, 2008icvts.ctsnetjournals.orgDownloaded from
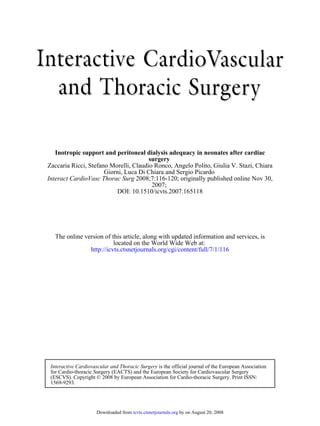
- 4. ARTICLE IN PRESS 118 Z. Ricci et al. / Interactive CardioVascular and Thoracic Surgery 7 (2008) 116–120 Fig. 2. Both PD creatinine (a) and LDH (b) dialysate to plasma ratio (DyP) showed a direct correlation with dwell times duration. In the case of LDH, longer dwell times allowed a relatively higher increase in DyP ratio with respect to creatinine. This effect might elucidate the role of allowing longer dwell times in order to optimize clearance of higher molecular weight solutes. Fig. 3. PD creatinine clearance appeared to be a function of Qd. Fig. 1. Serum creatinine concentration at PD start, day 2 and day 3. Table 2 Hemodynamic parameters within the three inotropic score (IS) classes IS 1 IS 2 IS 3 P-value Lactates (mgydl) 36 (44) 36 (51) 41 (41) 0.88 MAP (mmHg) 48 (7) 53 (9) 48 (10) 0.15 CVP (mmHg) 8 (3) 9 (2) 7 (3) 0.43 HR (bymin) 152 (6) 152 (15) 163 (14) 0.10 MAP, mean arterial pressure; CVP, central venous pressure; HR, heart rate. surgery. Age at operation was 21 (17) days and weight 2.8 (0.6) kg. Fifty-five dialysate collections were performed. Five patients out of 20 stopped PD before the third protocol day. PD was administered for 2.5 (2) days. Heart rate, systolic arterial pressure, central venous pressure and lac- tate levels did not show statistical differences between the three IS categories (P)0.05) (Table 2). Serum creatinine concentration at PD start was 0.97 mgydl (0.9); it was 0.8 (0.6) at PD stop (P-0.05) (Fig. 1). Mean prescribed Qd was 60 (45) mlyh. PD creatinine clearance was 3.4 (2.1) mlyminy1.73 m and ultrafiltration rate was 9.75 (10)2 mlyh. As expected, DyP showed a direct correlationcreatine with dwell time duration (rs0.37, Ps0.009) (Fig. 2a). PD creatinine clearance appeared to be correlated Qd up to a dialysate of 100 mlyh (Ps0.02) (Fig. 3). No correlation was present between IS and PD creatinine clearance (rs0.178, Ps0.2). This tendency was maintained when patients were stratified into three IS classes and three Qd classes (Fig. 4): Qd but not IS was found to affect peritoneal creatinine clearance (Ps0.0135). Residual renal creatinine clearance was present in seven patients and was 31 (26) mlyminy1.73 m . Ultrafiltration rate was not correlated to Qd (rsy0.05,2 Ps0.2) nor to IS (rsy0.02, Ps0.18). PD allowed to achieve a mean negative fluid balance of 160 (228) mlyday, that corresponded to 10.5 mlyh. LDH clearance was 0.59 (0.85) mlymin=1.73 m . DyP appeared to have2 LDH a direct correlation with dwell times (rs0.28, Ps0.048) (Fig. 2b) but linear regression did not show any correlation between LDH clearance and Qd. Albumin loss was present through peritoneal drainage. Mean DyP was 0.05 (0.06)albumin without significant differences within the three IS classes (P)0.05). Mean albumin concentration in peritoneal drain- age was 0.27 gydl (0.46) with a mean albumin loss in the 24 h of 2.2 g (1.3): in particular, daily albumin loss ranged from 0.01 to 4.3 g. In-hospital mortality among this cohort of patients was 20%, that was significantly higher than the overall neonatal population admitted to our ICU (4.8%, Ps0.02). There was full renal recovey in 19 patients (95%) at PD stop. No major complications were reported. Catheter site leakage from catheter insertion was observed in two patients but did not require any specific intervention. Hemodynamic derange- ments were never described in correlation with DP cycles. by on August 20, 2008icvts.ctsnetjournals.orgDownloaded from
- 5. ARTICLE IN PRESS 119Z. Ricci et al. / Interactive CardioVascular and Thoracic Surgery 7 (2008) 116–120 Fig. 4. Patients were stratified into three IS classes and three Qd classes: Qd but not IS was found to affect peritoneal creatinine clearance (Ps0.0135). 4. Discussion PD represents a simple and safe system for fluid removal, depending on osmolarity, volume and dwell-time of the dialysis fluid. Prevention and treatment of fluid overload, main goal of acute renal support, are more likely to be achieved by application of high dialysate volumes w8–10x. Unfavorably, modifications of atrial and mean pulmonary artery and systemic pressure have been observed in chronic PD and in children after cardiac surgery w11x. For this reason, a PD prescription of 10 mlykg, previously defined ‘low volume PD’, is commonly prescribed during neonatal RRT w8x. The aim of our study was to show adequacy of low flow PD, evaluating if its efficiency at different dwell times was affected by vasopressor drug administration and patients hemodynamic conditions. Our cohort of 20 post- cardiosurgical neonates was very homogeneous about age, weight and BSA. Interestingly, our patients tended to main- tain a similar mean arterial pressure and heart rate inde- pendently from IS, probably due to the fact that in our center inotropes and vasopressors dose is targeted on these parameters. In all patients, ultrafiltration needs were ade- quately fulfilled by PD with an ultrafiltration rate of about 10 mlyh and a negative fluid balance ranging from 50 to 500 mlyday. Net ultrafiltration depends mainly on glucose concentration of dialysis bags: in our cohort, ultrafiltration was not influenced by Qd nor by IS. Our PD prescription determined a relatively low creatinine clearance with a tendency to increase with Qd: since cycle volumes were predetermined at 10 mlykg, Qd was augmented only by the increase of cycles per hour and by the consequent decrease of dwell times. Creatinine molecular weight is sufficiently small to cross efficiently the peritoneal membrane (high DyP ) even when dwell times were very short (Fig. 2a):creatine for this reason low flow PD is able to progressively increase creatinine clearance at high Qd with short dwell times. IS seemed to have no impact on PD efficiency and creat- inine clearance was never affected by hemodynamic status. Peritoneal blood flow is generally considered high enough to avoid any limitations in solute clearance. Nonetheless, the real impact of effective peritoneal blood flow is still controversial w12x. In our patients, the absence of corre- lation between IS and PD creatinine clearance might sug- gest that during low volume PD mesenteric blood flow never decreased to a level able to impact PD efficiency. It remains to be elucidated however, if vasopressor adminis- tration actually causes mesenteric blood flow reduction, when hemodynamic parameters are maintained close to normal levels w13x. The direct correlation between creat- inine clearance and Qd tended to reach a plateau for flows above 100 mlyh, that were rarely achieved in our patients. This threshold might represent the point where mesenteric blood flow is considered to be a limiting factor to further clearance rise: it can be speculated that only after reaching this level of PD dose, IS and hemodynamic status might impact treatment efficiency. For larger solutes, the low diffusion coefficients of the molecule may represent the most important limitation to transport w14, 15x. In our treatments, analysis of LDH clearance, a 140 kD molecular weight solute, showed a different clearance pattern from creatinine: dwell times influenced DyP (Fig. 2b) to theLDH point that the increase of cycles per hour and the conse- quent decrease of dwell times did not determine any clearance rise. Differently from what is described above about creatinine, higher molecular solutes clearance might be improved by high exchange volumes with prolonged dwell times, in order to optimize peritoneal diffusion. We found a significant albumin loss through peritoneal drain- age: such amount of proteins is routinely infused in excess by fresh frozen plasma and human albumin to our patients. Furthermore, the clinical meaning of such finding is unclear: particularly, the wide range of albumin loss does not allow to understand whether the albumin was lost due to ascites, secondary to heart failure, or to capillary leakage, secondary either to generalized inflammation and to chemical peritonitis. A major limit of this study was its observational nature and no definitive conclusions can be drawn by these results. Measured solutes and PD prescriptions were not modified with respect to the routine of our department. Nonethe- less, this is the first attempt to monitor PD prescription and delivery. Further prospective studies should analyze different PD exchange models and specific mediators clear- ances to verify our suggestions. 5. Conclusions Low flow PD in neonates shows optimal ultrafiltration patterns and adequate small solute clearances, irrespective of hemodynamic status or vasopressor support. References w1x Chan K-L, Ip P, Chiu CSW, Cheung Y-F. Peritoneal dialysis after surgery for congenital heart disease in infants and young children. Ann Thorac Surg 2003;76:1443–1449. w2x Sorof JM, Stromberg D, Brewer ED, Feltes TF, Fraser CD. Early initiation of peritoneal dialysis after surgical repair of congenital heart disease. Pediatr Nephrol 1999;13:641–645. w3x Kist-van Holthe tot Echten JE, Goedvolk CA, Doornaar MBME, van der Vorst MMJ, Bosman-Vermeeren JM, Brand R, van der Heijden AJ, Schoof PH, Hazekamp MG. Acute renal insufficiency and renal replacement therapy after pediatric cardiopulmonary bypass surgery. Pediatr Cardiol 2001;22:321–326. w4x Picca S, Principato F, Mazzera E, Corona R, Ferrigno L, Marcelletti C, Rizzoni G. Risks of acute renal failure after cardiopulmonary bypass surgery in children: a retrospective 10-year case-control study. Nephrol Dial Transplant 1995;10:630–636. w5x Bailey D, Phan V, Litalien C, Ducruet T, Me´rouani A, Lacroix J, Gauvin F. Risk factors of acute renal failure in critically ill children: a prospect- by on August 20, 2008icvts.ctsnetjournals.orgDownloaded from
- 6. ARTICLE IN PRESS 120 Z. Ricci et al. / Interactive CardioVascular and Thoracic Surgery 7 (2008) 116–120 ive descriptive epidemiological study. Pediatr Crit Care Med 2007;8:29– 35. w6x McNiece KL, Ellis EE, Drummond-Webb JJ, Fontenot EE, O’Grady CM, Blaszak RT. Adequacy of peritoneal dialysis in children following cardio- pulmonary bypass surgery. Pediatr Nephrol 2005;20:972–976. w7x Shore S, Nelson D, Pearl J, Manning P, Wong H, Shanley T, Keyser T, Schwartz S. Usefulness of corticosteroid therapy in decreasing epineph- rine requirements in critically Ill infants with congenital heart disease. Am J Cardiol 2001;88:591–594. w8x Golej J, Kitzmueller E, Hermon M, Boigner H, Burda G, Trittenwein G. Low-volume peritoneal dialysis in 116 neonatal and paediatric critical care patients. Eur J Pediatr 2002;161:385–389. w9x Goldstein SL, Somers MJ, Baum MA, Symons JM, Brophy PD, Blowey D, Bunchman TE, Baker C, Mottes T, McAfee N, Barnett J, Morrison G, Rogers K, Fortenberry JD. Pediatric patients with multi-organ dysfunc- tion syndrome receiving continuous renal replacement therapy. Kidney Int 2005;67:653–658. w10x Foland JA, Fortenberry JD, Warshaw BL, Pettignano R, Merritt RK, Heard ML, Rogers K, Reid C, Tanner AJ, Easley KA. Fluid overload before continuous hemofiltration and survival in critically ill children: a ret- rospective analysis. Crit Care Med 2004;32:1771–1776. w11x Dittrich S, Vogel M, Daihnert I, Haas NA, Alexi-Meskishvilli V, Lange PE. Acute hemodynamic effects of post cardiotomy peritoneal dialysis in neonates and infants. Intensive Care Med 2000;26:101–104. w12x Waniewski J, Werynski A, Lindholm B. Effect of blood perfusion on diffusive transport in peritoneal dialysis. Kidney Int 1999;56:707–713. w13x Bourgoin A, Leone M, Delmas A, Garnier F, Albanese J, Martin C. Increasing mean arterial pressure in patients with septic shock: effects on oxygen variables and renal function. Crit Care Med 2005;33:780– 786. w14x Bokesch PM, Kapural MB, Mossad EB, Cavaglia M, Appachi E. Drummond- Webb JJ, Mee RBB. Do peritoneal catheters remove pro-inflammatory cytokines after cardiopulmonary bypass in neonates? Ann Thorac Surg 2000;70:639–643. w15x Alkan T, Evin AA, Tu Rkog Lu H, Paker T, Sas, Mazel A, Bayer, Ersoy C, Askin D, Aytac A. Postoperative prophylactic peritoneal dialysis in neonates and infants after complex congenital cardiac surgery. ASAIO J 2006;52:693–697. by on August 20, 2008icvts.ctsnetjournals.orgDownloaded from
- 7. DOI: 10.1510/icvts.2007.165118 2007; 2008;7:116-120; originally published online Nov 30,Interact CardioVasc Thorac Surg Giorni, Luca Di Chiara and Sergio Picardo Zaccaria Ricci, Stefano Morelli, Claudio Ronco, Angelo Polito, Giulia V. Stazi, Chiara surgery Inotropic support and peritoneal dialysis adequacy in neonates after cardiac This information is current as of August 20, 2008 & Services Updated Information http://icvts.ctsnetjournals.org/cgi/content/full/7/1/116 including high-resolution figures, can be found at: References http://icvts.ctsnetjournals.org/cgi/content/full/7/1/116#BIBL This article cites 15 articles, 3 of which you can access for free at: Subspecialty Collections http://icvts.ctsnetjournals.org/cgi/collection/congenital_cyanotic Congenital - cyanotic http://icvts.ctsnetjournals.org/cgi/collection/congenital_acyanotic Congenital - acyanotic http://icvts.ctsnetjournals.org/cgi/collection/cardiac_other other Cardiac -http://icvts.ctsnetjournals.org/cgi/collection/anesthesia Anesthesia following collection(s): This article, along with others on similar topics, appears in the Permissions & Licensing icvts@ejcts.chits entirety should be submitted to: Requests to reproducing this article in parts (figures, tables) or in Reprints icvts@ejcts.ch For information about ordering reprints, please email: by on August 20, 2008icvts.ctsnetjournals.orgDownloaded from