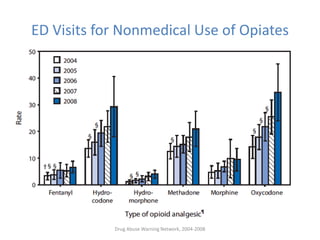
This document summarizes substance abuse issues faced in emergency departments. It notes that substance abuse patients are frequent emergency department users who require significant resources. Over 5 million emergency department visits annually are related to drugs, including 2.5 million specifically for drug abuse or misuse. Prescription opioid abuse and overdoses have risen dramatically in recent years. New CDC guidelines aim to curb opioid prescribing practices to help address this crisis. Emergency physicians are on the front lines of this issue and see the consequences of opioid addiction firsthand.






































































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)




![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)


