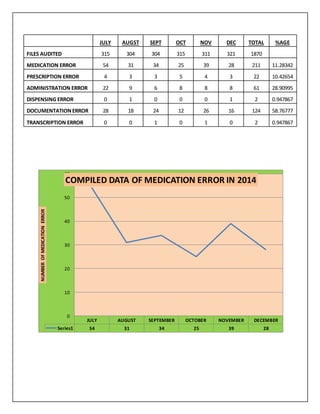
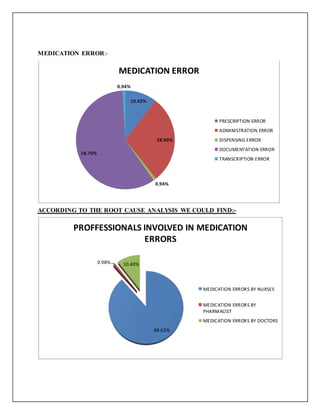
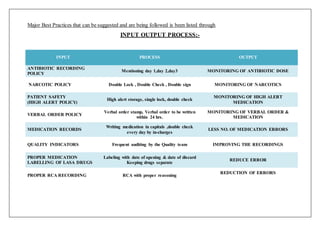
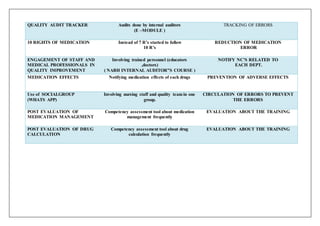
A study was conducted from July 2014 to December 2014 to detect medication errors at a hospital in India. A total of 1870 patient files were reviewed and 211 medication errors were found, representing an error rate of 11.28%. The most common errors were documentation errors (58.76%), followed by administration errors (28.90%). Nurses were responsible for most errors (88.62%), followed by doctors (10.40%). Best practices for medication safety identified included strict policies on antibiotics, narcotics, and high-alert medications, as well as improved documentation, labeling, auditing, and staff education.