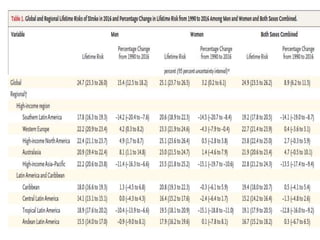
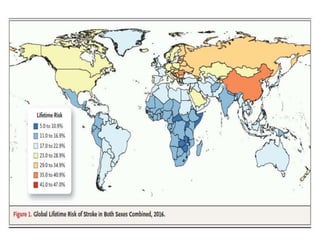
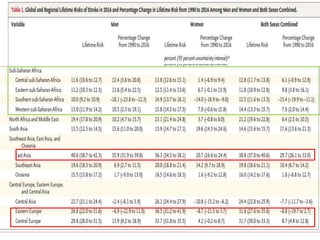
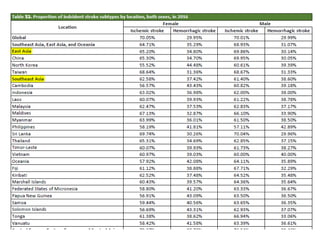
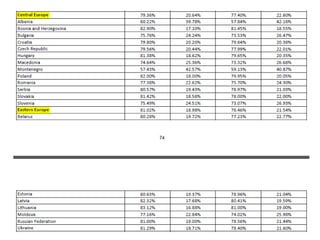
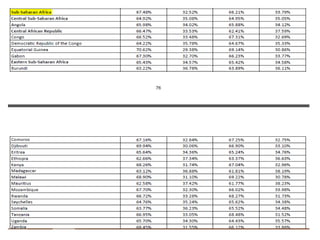
This document presents a study on global, regional, and country-specific lifetime risks of stroke from 1990 to 2016, revealing that stroke accounts for a significant portion of global deaths and disability-adjusted life-years, particularly in low-income countries. The global lifetime risk of stroke was estimated at 24.9% in 2016, with variations by region and socioeconomic development, and it increased from 22.8% in 1990. Key risk factors include elevated blood pressure, and the findings suggest the importance of preventative measures for stroke across various demographics.