OUTLINE
Introduction tospinal cord
Spinal nerves
~Cervical nerves
~ Thoracic nerves
~ Lumbar nerves
~ Sacral nerves
~ Coccygeal nerves
Segments of the spinal cord
Special features of the spinal cord
Conclusion
References
4.
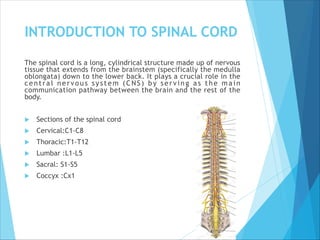
INTRODUCTION TO SPINALCORD
The spinal cord is a long, cylindrical structure made up of nervous
tissue that extends from the brainstem (specifically the medulla
oblongata) down to the lower back. It plays a crucial role in the
central nervous system (CNS) by serving as the main
communication pathway between the brain and the rest of the
body.
Sections of the spinal cord
Cervical:C1-C8
Thoracic:T1-T12
Lumbar :L1-L5
Sacral: S1-S5
Coccyx :Cx1
5.
STRUCTURE OF THESPINAL
CORD
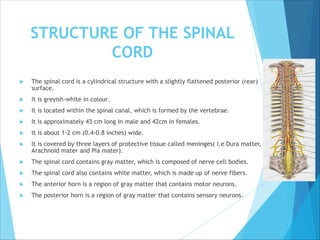
The spinal cord is a cylindrical structure with a slightly flattened posterior (rear)
surface.
It is greyish-white in colour.
It is located within the spinal canal, which is formed by the vertebrae.
It is approximately 43 cm long in male and 42cm in females.
It is about 1-2 cm (0.4-0.8 inches) wide.
It is covered by three layers of protective tissue called meninges( i.e Dura matter,
Arachnoid mater and Pia mater).
The spinal cord contains gray matter, which is composed of nerve cell bodies.
The spinal cord also contains white matter, which is made up of nerve fibers.
The anterior horn is a region of gray matter that contains motor neurons.
The posterior horn is a region of gray matter that contains sensory neurons.
6.
FUNCTIONS OF THESPINAL
CORD
Sensory Processing: The spinal cord processes sensory
information from the body, including pain, temperature,
touch, and pressure.
Motor control: Signals from your brain to other body parts
let you move when you want to. They also control
involuntary (autonomic) functions like your heartbeat and
breathing. Involuntary functions happen automatically
without you thinking about them.
Reflexes: Reflexes are automatic physical responses. The
patellar reflex makes your lower leg kick forward when a
healthcare provider taps your shin just below your kneecap
(patella). Your spinal cord controls some reflexes without
involving your brain.
7.
SPINAL NERVES
Spinal nervesare nerves that arise from the spinal cord and emerge through the
spinal column. There are 31 pairs of spinal nerves:
Functions
1. Motor control: Transmit signals to muscles for movement.
2. Sensory transmission: Carry sensory information from the body to the
brain.
They include the
Cervical nerves (8 pairs): Control neck, shoulder, and arm functions.
Thoracic nerves(12 pairs): Control chest and abdominal functions.
Lumbar nerves (5 pairs): Control lower back, hip, and leg functions.
Sacral nerves (5 pairs): Control pelvic and leg functions.
Coccygeal nerve (1 pair): Controls pelvic floor functions.
9.
CERVICAL NERVES
INTRODUCTION
The cervicalnerves are a group of spinal nerves that arise from the
cervical spine (neck region) in the human body.
There are 8 pairs of cervical nerves (C1-C8) that play a crucial role in
controlling various functions, including motor functions and sensory
functions
Damage or compression of cervical nerves can lead to various symptoms,
including pain, numbness, tingling, and weakness in the neck, shoulders,
and arms
MAJOR FUNCTIONS OF THE CERVICAL NERVES
Motor functions
1. Controlling muscles of the neck, shoulders, and arms
2. Regulating movements of the head, neck, and limbs
Sensory functions
1. Transmitting sensations such as touch, pressure, temperature, and
pain from the skin and muscles of the neck, shoulders, and arms.
10.
MAJOR FUNCTIONS OFEACH OF THE
SEGMENTS OF THE SPINAL NERVES
C1 (Suboccipital nerve): Motor control to suboccipital muscles,
involved in head movements.
C2 (Greater occipital nerve): Sensory innervation to the skin of the
back of the head.
C3: Sensory innervation to the skin of the neck and motor control to
neck muscles.
C4*: Motor control to neck and shoulder muscles, sensory innervation
to the skin of the neck and shoulder.
C5: Motor control to muscles of the shoulder and arm (deltoid, biceps).
C6: Motor control to muscles of the arm and forearm (biceps, wrist
extensors).
C7: Motor control to muscles of the arm and forearm (triceps, wrist
extensors).
C8: Motor control to muscles of the forearm and hand, sensory
innervation to the skin of the arm and hand.
11.
THORACIC NERVES
Each thoracicspinal nerve emerges from the spinal cord at its
respective vertebral level, from T1 to T12. Like all spinal
nerves, they originate from two roots:
- The dorsal (posterior) root carries sensory (afferent) fibers.
- The ventral (anterior) root carries motor (efferent) fibers.
These roots combine to form a mixed spinal nerve that exits
the spinal column via the intervertebral foramina. T1 is unique
because it contributes to the brachial plexus and helps control
the upper limb, while the rest (T2–T12) largely become
intercostal nerves, running between the ribs. T12 becomes the
subcostal nerve.
These nerves are responsible for a lot of essential bodily
functions—from breathing to maintaining posture and
transmitting sensory information from the trunk. They don’t
get the spotlight very often, but they work quietly behind the
scenes to keep us functioning
12.
FUNCTIONS OF THETHORACIC
NERVES
Respiratory Function
Though the phrenic nerve (C3–C5) controls the diaphragm, the intercostal muscles
(innervated by T1–T11) and abdominal muscles (T7–T12) play key roles in breathing,
especially during deep inspiration, forced expiration, coughing, and sneezing.
- External intercostals help lift the ribs for inhalation.
- Internal intercostals aid in forced exhalation.
- T12 also supports core stability and abdominal pressure.
In spinal cord injuries, especially above T6, impaired intercostal function can
cause respiratory complications, even if the diaphragm is still functional.
Dermatomes – Sensory Mapping of the Trunk
Dermatomes are specific skin regions innervated by a single spinal nerve root. The
thoracic dermatomes follow a segmental, belt-like pattern across the chest and
abdomen:
- T4 = nipple line - T10 = umbilicus - T12 = suprapubic area
These landmarks are super important in neurological exams. Conditions like herpes
zoster (shingles) often affect a single dorsal root ganglion, causing pain and a rash
along one dermatome—usually a thoracic one.
13.
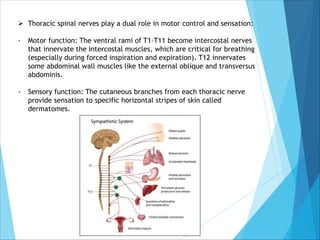
Ø Thoracic spinalnerves play a dual role in motor control and sensation:
- Motor function: The ventral rami of T1–T11 become intercostal nerves
that innervate the intercostal muscles, which are critical for breathing
(especially during forced inspiration and expiration). T12 innervates
some abdominal wall muscles like the external oblique and transversus
abdominis.
- Sensory function: The cutaneous branches from each thoracic nerve
provide sensation to specific horizontal stripes of skin called
dermatomes.
14.
LUMBAR NERVES
INTRODUCTION
Lumbar nervesare the five pairs of spinal nerves (L1-L5)
that emerge from the lumbar region of the spinal cord.
They are vital in transmitting sensory information and
controlling motor functions in the lower back, buttocks, hips,
legs, and feet, contributing to lower limb mobility and
sensation.
The lumbar nerves are a crucial component of the peripheral
nervous system, responsible for transmitting sensory and
motor signals in the lower part of the body.
These nerves emerge through small openings in the vertebral
column called intervertebral foramina
15.
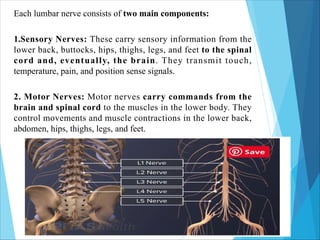
Each lumbar nerveconsists of two main components:
1.Sensory Nerves: These carry sensory information from the
lower back, buttocks, hips, thighs, legs, and feet to the spinal
cord and, eventually, the brain. They transmit touch,
temperature, pain, and position sense signals.
2. Motor Nerves: Motor nerves carry commands from the
brain and spinal cord to the muscles in the lower body. They
control movements and muscle contractions in the lower back,
abdomen, hips, thighs, legs, and feet.
16.
FUNCTIONS OF THELUMBAR NERVES
L1- Responsible for muscle control and sensory
functions in the hip and lower back area. Also plays a
role in the groin and genitals
L2- Controls and Supports the muscles and skin of the
upper thigh and hip. Provides sensation in the front and
the inner thighs
L3- Controls the muscles of the lower abdomen and
thigh. Also involved in knee reflex
L4- Innervates the knee and thigh muscles and lower
legs, playing a role in knee reflexes.
L5- Controls muscles of the lower foot, leg, and toes.
Provides sensation to the outer side of the lower leg, the
top of the foot and the web space between the first and
the second toes
17.
SACRAL NERVES
INTRODUCTION
The sacralnerves are a group of spinal nerves that emerge from the sacral segment of the spinal cord and play
a critical role in motor and sensory innervation to the pelvis, perineum, and lower limbs. They also contribute
significantly to autonomic (parasympathetic) functions in the pelvic organs.
There are five pairs of sacral spinal nerves, labeled S1 to S5, along with the coccygeal nerve (Co1). These nerves
are part of the cauda equina, the bundle of nerves that descends from the conus medullaris (end of the spinal
cord).
SACRAL PLEXUS
The anterior rami of L4, L5 (via the lumbosacral trunk) and S1–S4 form the sacral plexus, which lies on the
posterior pelvic wall, anterior to the piriformis muscle. It gives rise to several important motor and sensory
nerves, notably:
Major Nerves from the Sacral Plexus:
Sciatic nerve (L4–S3) – the largest nerve in the body; supplies the posterior thigh and all of the leg and foot.
Superior gluteal nerve (L4–S1) – supplies gluteus medius, minimus, and tensor fasciae latae.
Inferior gluteal nerve (L5–S2) – innervates the gluteus maximus.
Posterior femoral cutaneous nerve (S1–S3) – supplies skin of the posterior thigh and perineum.
Pudendal nerve (S2–S4) – major somatic nerve of the perineum, innervates external genitalia, perineal
muscles, and the external anal sphincter.
Nerves to pelvic muscles – e.g., nerve to piriformis, nerve to obturator internus, nerve to levator ani.
Pelvic splanchnic nerves (S2–S4) – carry parasympathetic fibers to pelvic viscera, including the bladder,
uterus, and rectum.
18.
FUNCTIONS OF SACRALNERVES
Motor Functions:
Control muscles in the buttocks, posterior thigh, most of the leg and
foot, and pelvic floor muscles.
Enable voluntary control of the urinary bladder and anal sphincters.
Sensory Functions:
Convey sensory input from:
Posterior thigh
Lower leg and foot
Perineal region (including the external genitalia and anus)
Posterior pelvic wall
Autonomic (Parasympathetic) Functions:
Regulate micturition (urination), defecation, and sexual functions
via the pelvic splanchnic nerves.
19.
COCCYGEAL NERVES
INTRODUCTION
Introduction
The coccygealnerve is the 31st pair of spinal nerves in the human body and is the
smallest and most inferior spinal nerve. It arises from the conus medullaris region of
the spinal cord and plays a limited yet important role in sensory innervation of the
skin near the coccyx and minor motor functions in the pelvic floor.
Although often overlooked due to its small size, the coccygeal nerve, along with
contributions from sacral nerves S4 and S5, forms the coccygeal plexus, which
innervates certain structures in the pelvic floor and skin over the coccyx
COCCYGEAL PLEXUS
The coccygeal nerve contributes to the formation of the coccygeal plexus, which is
made up of:
The ventral rami of S4, S5, and Co1.
This small plexus lies on the pelvic surface of the coccygeus muscle and is usually
incomplete or variable among individuals.
Branches and Distribution
Anococcygeal Nerve(s)
Arises from the coccygeal plexus (typically from Co1 and contributions from S4, S5).
Pierces the sacrotuberous ligament and passes to the skin between the coccyx and
the anus.
20.
COCCYGEAL NERVES CONT’D
Providessensory innervation to:
Skin over the coccyx
Post-anal region (sacrococcygeal area)
Note: The number of anococcygeal nerves can vary, often one or two,
and they may be small or absent in some individuals.
Minor Motor Contribution
The Co1 nerve may provide motor innervation to parts of the levator
ani and coccygeus muscles, though this is mostly carried out by
branches from S4 and S5.
21.
FUNCTIONS OF THE
COCCYGEALNERVES
Sensory Functions
• Supplies cutaneous sensation to the skin in the region just posterior to
the anus and over the coccyx.
• This area includes the intergluteal cleft, also called the sacrococcygeal
region.
Motor Functions
• Possible minor innervation of pelvic diaphragm muscles:
• Coccygeus (ischiococcygeus)
• Part of levator ani
• Helps support pelvic organs and maintain continence, although S3–S4
are the main contributors.
• Reflex Involvement
• Participates in sacrococcygeal reflex arcs that may involve autonomic
responses in the anal and genital region.
22.
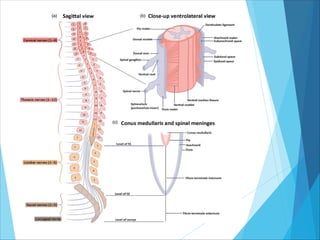
SEGMENTS OF THESPINAL CORD
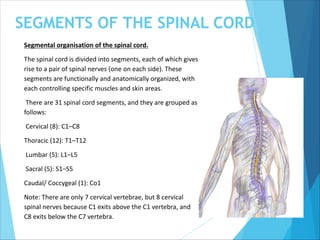
Segmental organisation of the spinal cord.
The spinal cord is divided into segments, each of which gives
rise to a pair of spinal nerves (one on each side). These
segments are functionally and anatomically organized, with
each controlling specific muscles and skin areas.
There are 31 spinal cord segments, and they are grouped as
follows:
Cervical (8): C1–C8
Thoracic (12): T1–T12
Lumbar (5): L1–L5
Sacral (5): S1–S5
Caudal/ Coccygeal (1): Co1
Note: There are only 7 cervical vertebrae, but 8 cervical
spinal nerves because C1 exits above the C1 vertebra, and
C8 exits below the C7 vertebra.
24.
SPECIAL FEATURES OFTHE SPINAL
CORD
REFLEX ACTION CENTER
The spinal cord is a vital component of the central nervous system (CNS)
that functions not only as a pathway for communication between the
brain and body but also as a highly efficient reflex action center. Reflex
actions are automatic, involuntary responses to stimuli that are crucial for
protection, posture, and coordination. The spinal cord is uniquely
structured to process these responses without the need for conscious
brain involvement, allowing the body to react swiftly to potentially
harmful stimuli.
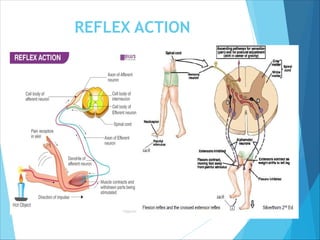
The spinal cord mediates a variety of reflexes:
•Monosynaptic reflexes, such as the patellar (knee-jerk) reflex
•Polysynaptic reflexes, such as the withdrawal reflex
•The crossed extensor reflex involves both sides of the spinal cord and
helps maintain balance when one limb withdraws from a stimulus
TWO WAYCONDUCTION PATHWAY
The spinal cord serves as a bidirectional communication system; sensory info up to the
brain, motor commands down to the body. It is the only structure besides the brainstem
capable of both ascending and descending conduction in real time.
ASCENDING PATHWAYS – SENSORY INPUT TO THE BRAIN
The ascending tracts of the spinal cord are responsible for transmitting sensory (afferent)
information from the body to the brain. These signals include sensations such as touch,
pain, temperature, pressure, and proprioception (awareness of body position).
DESCENDING PATHWAYS – MOTOR OUTPUT FROM THE BRAIN
The descending tracts carry motor (efferent) commands from the brain to the spinal cord
and onward to muscles and glands. These tracts control voluntary movement, muscle
tone, and autonomic functions.
Ø NEUROPLASTICITY AND REPAIR POTENTIAL
Though limited, the spinal cord can exhibit plasticity, it can rewire some functions after
injury and training. It possesses a limited self-repair mechanism, especially in early life or
with therapy.
Ø INTEGRATION WITH AUTONOMIC NERVOUS SYSTEM
The spinal cord controls many autonomic functions such as bladder control, bowel
regulation, blood pressure via sympathetic pathways. The spinal cord acts as a local
controller of automatic internal processes, especially in the absence of brain input e.g
spinal shock recovery
OTHER SPECIAL FEATURES
27.
CONCLUSION
The spinal cordserves as a vital communication high
way between the brain facilitating both sensory input
and motor output through its segmented organization
and associated spinal nerves.
Its special features make it essential for rapid response,
coordination and basic life functions.
Together, these elements underscore the spinal cord’s
essential role in maintaining bodily function,
responsiveness and coordination.
28.
REFERENCES
Sembulingam, K.,& Sembulingam, P. (2019). Essentials
of Medical Physiology (8th ed.). Jaypee Brothers Medical
Publishers.
Guyton, A. C., & Hall, J. E. (2021). Textbook of Medical
Physiology (14th ed.). Elsevier.
Boron, W. F., & Boulpaep, E. L. (2020). Medical
Physiology (3rd ed.). Elsevier.
National Institute of Neurological Disorders and Stroke.
(n.d.). Spinal Cord Anatomy and Function. Retrieved from
https://www.ninds.nih.gov
TeachMeAnatomy. (n.d.). The Spinal Cord. Retrieved
from https://teachmeanatomy.info