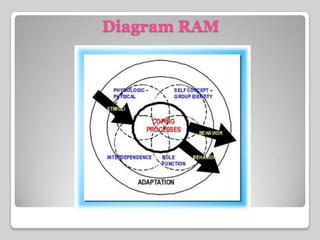
Sister Callista Roy developed the Adaptation Model of Nursing in the 1960s based on her observations of how individuals adapt to changes in their environment. The model views people as adaptive systems that interact with stimuli from the environment. There are four modes of adaptation: physiological, self-concept, role function, and interdependence. The goal of nursing according to the model is to promote positive adaptation by increasing adaptive responses and decreasing ineffective responses. The model has been widely applied in nursing research, education, and practice to understand how patients cope with illness or adversity.