Downloaded 50 times











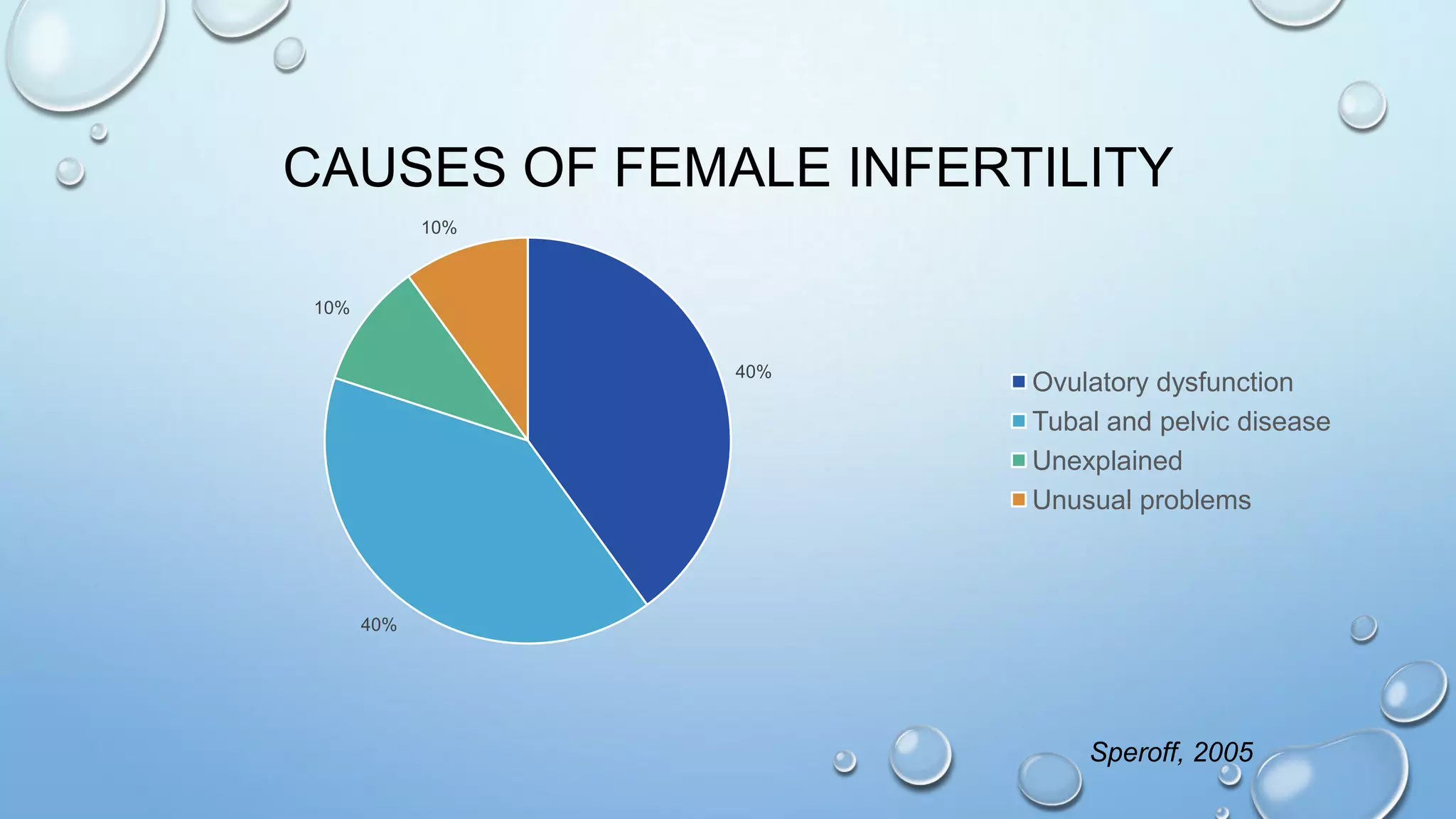

The document outlines the management of infertile couples in primary care, detailing gynecologic cancer screening, pre-conception counseling, and infertility evaluations. It includes guidelines on cervical, breast, endometrial, and ovarian cancer screening as well as definitions and causes of infertility, and emphasizes the need for various assessments and potential treatments. Additionally, it highlights the importance of optimally managing medical conditions and lifestyle factors in pre-conception care.



































































