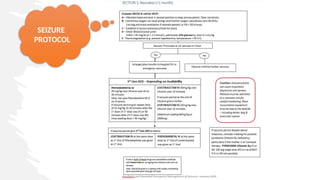
seizure
Seizure: A transientoccurrence of signs and/or symptoms due to abnormal
excessive and/or hypersynchronous discharge of neurons
• In practice two unprovoked seizures
occurring at least 24 hours apart.
• Unprovoked means a seizure that occurs
without an acute or reversible cause
Epilepsy: chronic
neurological disorder
characterized by
recurrent seizures that
occur without an acute
or reversible cause
3.
status epliepticus
Acondition InWhich Aseizure Lasts For About More Than 5mint
Without Self Termination Therefore Requiring With Antiepliptic Drugs
If Seizure Persist More Than 30mints Despite The Use Of Two AEDS
Patients Are Considered To Have Refactory SE
Which Can Have Long Term Consequences Including
Neuronal Death’ Neuronal Injury ‘And Alteration Of Neuronal
Netwerks
4.
Post ictal state
Alteredconsciousness
drowsiness
Confusion
nausea
hypertension
hemiparesis
headache,or other disorienting symptoms after aseizure
This may last for about 5-30 minutes
5.
What we willcover
• Epilepsy
• Key question in the history
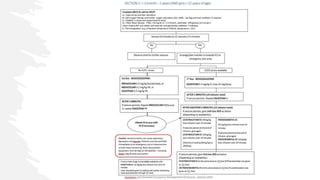
• Seizure protocol
• Choice of maintaince/when to start
• Advice on discharge for patient
• Approach to a child with motor delay
• Approach to history
• Upper motor neuron V lower motor neurons
• Quick comment on cerebellar signs
• Cerebral palsy
• Consideration for discharging patients with a complex neurology
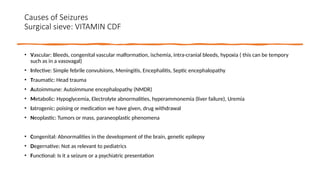
Causes of Seizures
Surgicalsieve: VITAMIN CDF
• Vascular: Bleeds, congenital vascular malformation, ischemia, intra-cranial bleeds, hypoxia ( this can be tempory
such as in a vasovagal)
• Infective: Simple febrile convulsions, Meningitis, Encephalitis, Septic encephalopathy
• Traumatic: Head trauma
• Autoimmune: Autoimmune encephalopathy (NMDR)
• Metabolic: Hypoglycemia, Electrolyte abnormalities, hyperammonemia (liver failure), Uremia
• Iatrogenic: poising or medication we have given, drug withdrawal
• Neoplastic: Tumors or mass, paraneoplastic phenomena
• Congenital: Abnormalities in the development of the brain, genetic epilepsy
• Degernative: Not as relevant to pediatrics
• Functional: Is it a seizure or a psychiatric presentation
8.
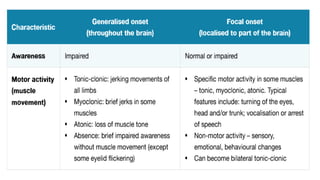
Symptoms of seizure
Eye deviation,staring or rapid eye blinking
Lip smack or bitting down(clonic)
Loss of tone (atonic)
Stiff extended limbs( tonic)
Rhythmic jerking of limbs or nodding of head( Tonic- clonic)
Loss of consciousness or impaired awareness
Appearing confused or notion of absence
9.
Continued…
Lip smackingor bitting down (clonic)
Loss of tone (atonic)
Stiff extended limbs( tonic)
Rhythmic jerking of limbs or nodding of head (tonic-clonic)
Loss of consciousness or impaired awareness
Appearing confused or notion of absences
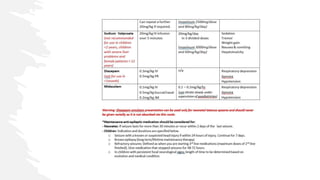
Respiratory distress or apnoeic spells
Loss of bladder or bowel control k
Epigastric sensation,sweating
Vocalisation ,arrest of speech
l
10.
Continued…
Some childrenmay experience an aura or a warning sign just before a seizure is about to happen
these can be feelings (e.g fear ,impending doom) or changes in vision/flashing lights,hearing or
sense of smell
Or hallucinations
Older children over 6y usually have similar seizure to adults
While infants and young children are more likely to have focal seizure with impairment of
awareness
11.
Are we sure
itseven a
seizure?
• Movement disorders
• Dystonia
• Non-epileptic
myoclonus
• Dyskinesia
• Paroxosymal ataxia
• Syncope and anoxic
seizures
• Reflex anoxic
seizures
• Breath holding
attacks
• Simple faints
( vasovagal syncope)
• Cardiac syncope and
long QT
• Behavioral event and
psychological disorders
• Daydreams
• Self gratification
• Tics and
steryotopies
• Non – epileptic
attack disorder –
psychogenic
• Sleep disorder
• Nightmares, night
terrors, narcolepsy
Seizure History
• Seizures
•Describe
• Before: Any trigger, any aura, any palpitation, what were they doing when it stared
• During: how long did it last, which movement started first, tongue bitting, urinary incontinence
• After: how long to take to return to normal? Confusion?
• Any associated symptoms in the past few days
• If new seizures must ask about head trauma
• Signs of raised ICP: early morning headache, vomiting, new weakness
• Symptoms that may cause electrolyte imbalance: Vomiting, diahorrea
• Recent illness, fever
• If they have had previous seizures what happened before
• If there is a history of seizures before on there on anti-epilieptic question that help you think why they have got worse
• What medication have they had, have they taken it, have they changed
• Is there development appropriate for there age
• Is there any family history of seizures
• Any cardiac history
• Past medical history that includes birth history
A child youhave just given two dose of
diazepam start to breath slower, what
medication could you consider now…….
24.
A child youhave just given two dose of diazepam
start to breath slower, what medication could you
consider now…….
Flumazenil
25.
Simple febrile convulsion
•Definition: An event occurring in Infancy or childhood between 3 months and 5 years of age,
associated with fever but without evidence of intracranial infection or defined cause for the
seizure
• National institute for health definition
• Can be Simple (70%) or Complex (30%)
• Simple: Generalized with no focalization, short (under 10-15mins), do not reoccur within 24
hours or the same febrile episode
• Important to warm families that could re-occur in the child next febrile illness
• Often run in families
• Most febrile seizures do not develop epilepsy
• If simple febrile convulsion and you have a clear source of fever child can be safely discharged
from hospital in ER
26.
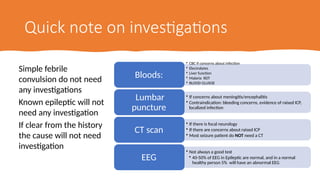
Quick note oninvestigations
Simple febrile
convulsion do not need
any investigations
Known epileptic will not
need any investigation
If clear from the history
the cause will not need
investigation
• CBC if concerns about infection
• Electrolytes
• Liver function
• Malaria RDT
• BLOOD GLUSOE
Bloods:
• If concerns about meningitis/encephalitis
• Contraindication: bleeding concerns, evidence of raised ICP,
localized infection
Lumbar
puncture
• If there is focal neurology
• If there are concerns about raised ICP
• Most seizure patient do NOT need a CT
CT scan
• Not always a good test
• 40-50% of EEG in Epileptic are normal, and in a normal
healthy person 5% will have an abnormal EEG
EEG
27.
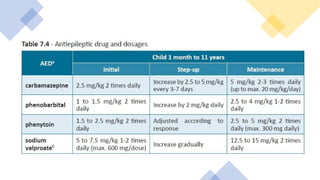
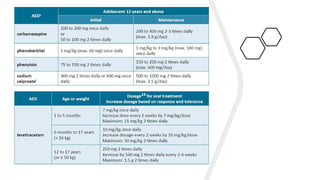
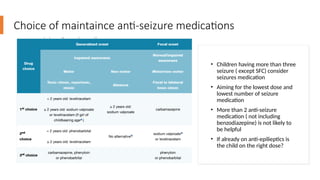
Choice of maintainceanti-seizure medications
• Children having more than three
seizure ( except SFC) consider
seizures medication
• Aiming for the lowest dose and
lowest number of seizure
medication
• More than 2 anti-seizure
medication ( not including
benzodiazepine) is not likely to
be helpful
• If already on anti-epilieptics is
the child on the right dose?
28.
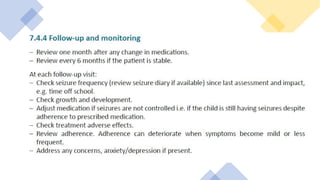
Advice on dischargefor Epileptics
• Explain what epilepsy is
• Explain what to do if a child has another seizure
• Remove the child from where thing can harm them
• Things a child should not do if they have epilepsy
• Be left alone in water, be alone near open fire, think about heights
• Talk about the importance of compliance with medication
• Explain if there are any side effect of the drugs that they should look out for
• Can think about advice around stigma
• Advice them to seek support for someone to monitor there seizure medication as an
outpatient
29.
A child with
developmentaldelay
• A 9 month old presents with malnutrition. Mother
tells you that they cant always neck hold and that
sometime they cough after feeding?
Key question toask in the History
• Movements
• Ask what they can do for themselves and
what age they learnt to do these skills
• Any regression/ loss of skills
• Associated features
• Seizures, abnormal movement
• Feeding
• Ask about vomiting
• When they cough after feeding
• How easy it was for them to establish feeding
• Past medical history
• Birth history
• Problem in the pregnancy: maternal
illness
• Problems in the delivery: birth asphyxia,
• Any illness in the neonatal periods
• challenges feeding, significant jaundice
• Drug history: medication and vaccinations
• Family history
• Similar children
• Early infant death, miscarriages
• Social history
• Consanguinity
32.
How would youexamine
• OBSERVATION: this will give you most of the clues
• What is the position of the limbs at rest
• What movement is there
• Is there asymmetry
• What are they eyes doing
• Smiling
• TONE
• Reflexes
• power
• If you never practice on a healthy baby you will never know what normal feels like
• Have a look up baby reflexes
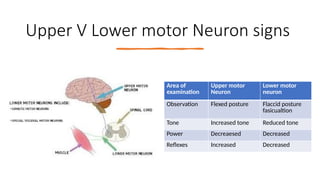
Upper V Lowermotor Neuron signs
Area of
examination
Upper motor
Neuron
Lower motor
neuron
Observation Flexed posture Flaccid posture
fasicualtion
Tone Increased tone Reduced tone
Power Decreaesed Decreased
Reflexes Increased Decreased
35.
Differential diagnosis formotor delay
• Vascular: Perinatal ischemia, neonatal strokes, hydrocephalus
• Infective: Congenital infections, Consequence of CNS infection
• Trauma: Birth trauma, Head trauma
• Autoimmune:
• Metabolic: Inborn errors of metabolism, hypothyroidism, kernicterus,
• Iatrogenic: Consequence of medication or surgery
• Neoplastic: Tumours – brain or paraneoplastic effect
• Congential: Congenital malformation, can be part of syndrome
• Degenerative: Genetic disorder e.g. SMA
• Functional: Malnutrition, poverty, poor attachment
36.
Cerebral palsy
• Definition:permanent, but not unchanging, disorders of movement and/or posture and
of motor function, which are due to a non-progressive interference, lesion, or
abnormality of the developing/immature brain
39.
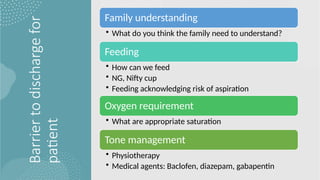
Barrier
to
discharge
for
patient
Family understanding
• Whatdo you think the family need to understand?
Feeding
• How can we feed
• NG, Nifty cup
• Feeding acknowledging risk of aspiration
Oxygen requirement
• What are appropriate saturation
Tone management
• Physiotherapy
• Medical agents: Baclofen, diazepam, gabapentin
#11 Syncope: a paroxysmal event cause by a sundden temporary decrease in the supply of oxygenated blood to the brain – manifested as loss of awareness
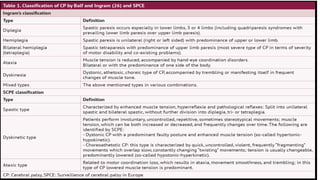
Dystonia: Dystonia is a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal, often repetitive, movements, postures, or both. Dystonia is often initiated or worsened by voluntary action and associated with overflow muscle activation
#25 Risk factors for re-occurance: ages less than 18 months, family history of febrile convulsion, low tempreture at the time of seizure and short duration of illness
Increased risk compared to the normal population
#32 What is Spasticity: Velocity dependent increase in tone













































![Shock_and_fluid_managment.......[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shockandfluidmanagment1-250618103540-0c29c219-thumbnail.jpg?width=640&height=640&fit=bounds)






















