Secondary Immunodeficiency is an weakened immune system that arises a consequence of external factors , this type of immunodeficiency is also known as acquired immunodeficiency.
Seminar assigned date: 27/06/2025
SUB TITLE : IMMUNOLOGY AND MICROBIAL GENETICS
SUB CODE : WMBM31 SEMESTER : III
TITLE : SECONDARY IMMUNODEFICIENCY
Seminar Completion date : 18 /07/2025
SUBMITTED BY:
S. SHAMILY
II M.Sc microbiology
Sri parmakalyani college
alwarkurichi
SUBMITTED TO:
Dr. S. VISWANATHAN
ASSOCIATE PROFESSOR
Sri parmakalyani college
alwarkurichi
2.
Aim :
To understandthe causes,
clinical features, diagnosis,
and management of secondary
(acquired) immunodeficiency
in order to improve early
detection, prevention of
complications, and
appropriate treatment.
Objectives:
1. Define secondary immunodeficiency and
distinguish it from primary immunodeficiency.
2. Identify common causes (e.g., HIV, malnutrition,
chemotherapy, chronic diseases).
3. Describe the underlying mechanisms that lead
to immune suppression.
4. Recognize the clinical features and
complications associated with secondary
immunodeficiency.
5. List diagnostic tools used to detect and monitor
immune system dysfunction.
6. Explain management strategies, including
treating the underlying cause and supportive
therapies.
7. Evaluate the role of prevention (e.g.,
vaccinations, nutritional support) in reducing the
burden of secondary immunodeficiency.
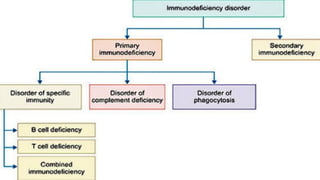
Immunodeficiency is astate in which the body’s immune system is
not able to fight with the infectious conditions.
It is also known as immuno-compromise.
Immunodeficiency disorders impair the immune system’s ability to
defend the body against foreign or abnormal cells that invade or
attack it (such as bacteria, viruses, fungi, and cancer cells).
As a result, unusual bacterial, viral, or fungal infections or
lymphomas or other cancers may develop.
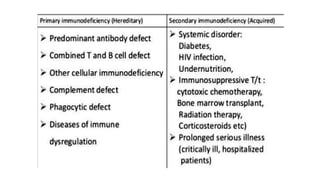
There are two types of immunodeficiency ;
• Primary immunodeficiency
• Secondary immunodeficiency
IMMUNODEFICIENCY
7.
> Secondary Immunodeficiencyrefers to a weakened immune system that
arises as a consequence of external factors or underlying medical
conditions, rather than being innate or genetic.
> This type of immunodeficiency is also known as acquired
immunodeficiency.
> Unlike primary immunodeficiencies, which are often present from birth
due to genetic mutations, secondary immunodeficiencies develop later in
life due to environmental influences, infections, medications, or other
health conditions.
SECONDARY IMMUNODEFICIENCY
8.
A variety ofdefects in the immune system give rise to immunodeficiency. In
addition to the primary immunodeficiencies, there are also acquired or Secondary
immunodeficiencies.
• One that has been known for some time is called acquired
hypogammaglobulinemia.
(As mentioned above, this condition is sometimes confused with common variable
immunodeficiency, a condition that shows genetic predisposition.)
• The origin of acquired hypogammaglobulinemia is unknown, and its major
symptom, recurrent infection, manifests itself in young adults.
9.
The patients generallyhave very low but detectable levels of total immunoglobulin.
T-cell numbers and function may be normal, but there are some cases with T-cell
defects and these may grow more severe as the disease progresses.
The disease is generally treated by immunoglobulin therapy, allowing patients
to survive into their seventh and eighth decades.
Unlike similar deficiencies described above, there is no evidence for genetic
transmission of this disease. Mothers with acquired hypogammaglobulinemia deliver
normal infants.
However, at birth the infants will be deficient in circulating immunoglobulin because
the deficiency in maternal circulation is reflected in the infant.
10.
Another form ofsecondary immunodeficiency, known as agent-induced
immunodeficiency, results from exposure to any of a number of chemical and biological
agents that induce an immunodeficient state.
Certain of these are drugs used to combat autoimmune diseases such as rheumatoid
arthritis or lupus erythematosis.
Corticosteroids, which are commonly used for autoimmune disorders, interfere with
the immune response in order to relieve disease symptoms.
13.
SPREAD OF HIV:
HIV-1 infects an individual is not known, epidemiological data
indicate that common means of transmission include homosexual and
heterosexual intercourse, receipt of infected blood or blood products,
and passage from mothers to infants.
Before tests for HIV in the blood supply were routinely used, patients
who received blood transfusions and hemophiliacs who received blood
products were at risk for HIV-1 infection.
Exposure to infected blood accounts for the high incidence of AIDS
among intravenous drug users who normally share hypodermic needles.
Infants born to mothers who are infected with HIV-1 are at high risk
of infection. Unless infected mothers are treated with anti-viral agents
before delivery, approximately 30% of infants born to them will become
infected with the virus.
14.
Possible vehicles ofpassage from mother to infant include blood transferred
in the birth process and milk in the nursing period.
Transmission from an infected to an uninfected individual is most likely by
transmission of HIV-infected cells—in particular, macrophages, dendritic cells, and
lymphocytes.
In the worldwide epidemic, it is estimated that 75% of the cases of HIV
transmission are attributable to heterosexual contact.
21.
CLINICAL FEATURES OFSECONDARY IMMUNODEFICIENCY :
The signs and symptoms of secondary immunodeficiency are often related to the
underlying cause, but common features may include:
• Increased frequency of infections: Particularly bacterial, viral, and fungal
infections, including opportunistic infections that would typically not affect healthy
individuals.
• Severe or prolonged infections: Infections that last longer than expected or are
more severe.
22.
• Unusual infections:Infections with pathogens that do not normally cause
disease in healthy individuals.
• Delayed wound healing: Because of the inability to mount an effective
immune response.
• Recurrent or chronic infections: Like pneumonia, sinusitis, or urinary tract
infections (UTIs), which may be harder to treat or may recur after treatment.
23.
CAUSES OF SECONDARYIMMUNODEFICIENCY :
1) Infectious Diseases:
HIV/AIDS: The most common cause; targets CD4+ T-helper cells leading to profound
cellular immunodeficiency.
Measles, EBV, CMV, Hepatitis viruses: Can transiently impair immune function.
2) Malnutrition:
Protein-energy malnutrition (PEM) impairs both cellular and humoral responses.
Micronutrient deficiencies (e.g., zinc, iron, vitamin A, and selenium) affect
lymphocyte function.
24.
3) Medical Treatments:
Chemotherapyand Radiotherapy:Non-specifically destroy proliferating immune
cells.
Corticosteroids: Suppress T-cell activation and cytokine production.
Immunosuppressants (e.g., cyclosporine, tacrolimus, biologics): Used in
transplantation and autoimmune diseases.
25.
4) Chronic Diseases:
Diabetesmellitus: Impairs neutrophil function and T-cell activity.
Chronic kidney/liver disease: Affects cytokine production and lymphocyte
function.
Cancer (esp. hematologic malignancies): E.g., leukemia and lymphoma
directly involve immune cells.
5) Age-related Factors:
Neonates: Immature immune system.
Elderly (Immunosenescence): Decline in T-cell number/function and thymic
involution.
26.
6) Environmental &Lifestyle Factors:
Alcoholism: Reduces macrophage and neutrophil function.
Smoking: Impairs mucosal immunity.
Stress and trauma: Can alter immune responsiveness.
27.
1. Clinical Evaluation:
✓ A detailed medical history, including underlying conditions (e.g.,
cancer, HIV, diabetes) and medication use (e.g., immunosuppressive therapy).
✓ Physical examination to look for signs of active or past infections.
DIAGNOSIS OF SECONDARY IMMUNODEFICIENCY :
2. Laboratory Tests :
✓ Complete Blood Count (CBC) to assess immune cell populations (e.g.,
lymphocytes, neutrophils).
✓ Immunoglobulin levels (IgA, IgG, IgM) to check for deficiencies.
✓ T-cell and B-cell counts: A reduced number of T-cells or B-cells may
indicate an underlying problem.
28.
✓ Flow cytometry:This can assess the function and number of
immune cells.
✓ HIV testing: If HIV/AIDS is suspected, specific tests like ELISA or
PCR are used to detect the virus.
3. Culture and Sensitivity:
✓ Culturing pathogens from blood, urine, or other body fluids to
identify infections.
✓ Sensitivity testing can help identify which antibiotics will be
most effective.
30.
The management ofsecondary immunodeficiency primarily involves
addressing the underlying cause of the immunodeficiency and providing
support to the immune system.
1. Treating the Underlying Condition:
HIV/AIDS: Antiretroviral therapy (ART) can help control the virus and
improve immune function.
Cancer: Chemotherapy, radiotherapy, and stem cell transplants may
be used, but these need to be carefully monitored to avoid excessive
suppression of the immune system.
Malnutrition: Proper nutritional support, including vitamins and
minerals, can help improve immune action.
MANAGEMENT AND TREATMENT :
31.
Chronic diseases: Tightmanagement of diseases
like diabetes or kidney disease can reduce the impact
on immune function.
2. Immunoglobulin Replacement Therapy:
For patients with low immunoglobulin
levels, intravenous or subcutaneous immunoglobulin
(IVIG or SCIG) can help provide passive immunity by
supplying the necessary antibodies.
32.
3. Prophylactic Treatment:
Antibiotics,antifungals, and antivirals may be prescribed to prevent
infections, especially in immunocompromised patients like those undergoing
chemotherapy.
Vaccination: It may be recommended for individuals with secondary
immunodeficiency, depending on the cause and type of immunodeficiency.
4. Stem Cell or Bone Marrow Transplantation:
In cases of cancer or certain inherited bone marrow disorders, stem cell or
bone marrow transplantation may be considered to restore immune function.
33.
• kuby Immunology6th
edition (Pg no : 441-444,449,451-455).
• Abbas :“Basic Immunology: Functions and Disorders of the Immune
System”- 6th
edition
• Roitt’s Immunology 8th
edition
https://images.app.goo.gl/z9ehzBpVYrEqfXjk9
Reference :
34.
1.Define secondary immunodeficiencyand distinguish it from primary
immunodeficiency.
2. Identify the major causes of secondary immunodeficiency,
including:Infections (e.g., HIV/AIDS)Malnutrition Medical treatments (e.g.,
chemotherapy, immunosuppressive drugs)Chronic diseases (e.g., diabetes,
cancer).
3. Describe the mechanisms by which these causes impair the immune system.
4. Recognize common clinical manifestations of secondary immunodeficiency
(e.g., increased susceptibility to infections, poor wound healing).
5. Explain the role of HIV as a major example of secondary immunodeficiency,
including its effect on CD4+ T cells.
6.Compare and contrast secondary and primary immunodeficiencies.
7. Discuss strategies for prevention and management.
8. Interpret basic case studies involving patients with secondary
immunodeficiency.
Learning outcomes :
35.
S W OT
Strengths Weaknesses Opportunities Threats
• Good learner & listener
• Creative ability
• Communication skill
• Adaptability
• Good time management
• Positive attitude and confidence
• Poor stress management
• Lack of forgetting certain
points during seminar
• Low self-confidence in new
situations
• Internships and volunteering
experiences.
• Access to online courses,
certifications, and workshops.
• Expanding global
opportunities through
technology.
• Growing industries needing
fresh graduates.
• High competition in the field
• Economic instability
• Requiring constant upskilling
persons.
• Health issues or personal
responsibilities.
• Challenges in workplace.
36.
A wise teacherplaced a large empty jar on the
table.He filled it with big rocks and asked his
students ,“Is it full? ” & his students are answered “
Yes ”.Then he added pebbles.They slid between the
rocks.“Full now?”"Yes."Then he poured sand.It
filled every gap.And finally , he poured in water. It
soaked in silently. The rocks are your values: family,
health, purpose.The pebbles are your goals and
daily duties.The sand is the small stuff, distractions
and the water there’s always time for a quiet
moment with someone you care about.
Moral : What you fill your life with matters more
than how much you fill it.
MORAL OF THE STORY : THE EMPTY JAR
44.
“ TEACHING ANDLEARNING IN ACTION ”
S. SHAMILY
24081236111712112
II M.Sc Microbiology
PG & RESEARCH DEPARTMENT OF
MICROBIOLOGY
Sri PARAMAKALYANI COLLEGE
ALWARKURICHI – 627412.
E-mail id: shamilyammu693@gmail.com