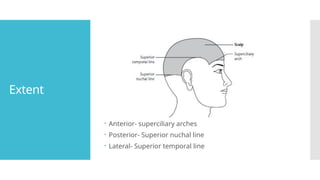
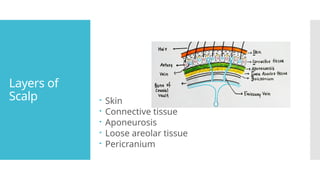
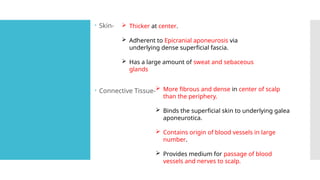
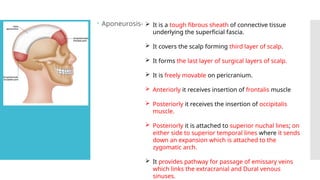
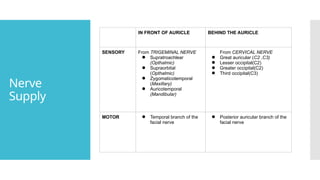
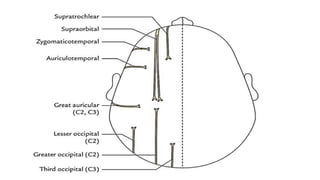
The document provides an extensive overview of the anatomy of the scalp, detailing its layers: skin, connective tissue, aponeurosis, loose areolar tissue, and pericranium, along with their functions, including blood supply and nerve innervation. It also discusses clinical applications, such as the dangerous area of the scalp, various hematomas, and associated blood and venous drainage. Additionally, the document describes conditions like caput succedaneum and cephalhematoma that present in clinical scenarios related to childbirth and cranial injuries.






































![Scalp[1]](https://cdn.slidesharecdn.com/ss_thumbnails/scalp1-170504174806-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








