Download to read offline






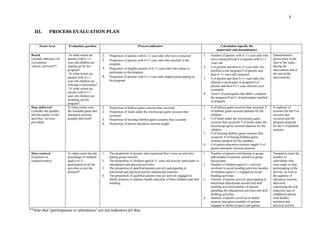



NOLA's Kids in Motion is a 4-month intervention for children ages 6-11 and their parents in New Orleans. It aims to teach nutrition, physical activity, and stress coping skills through twice weekly games and weekly Dance Dance exergames. The target population has a BMI over the 95th percentile. The intervention will be evaluated through a process evaluation measuring reach, dose delivered, and dose received using indicators like participation rates and the number of planned versus delivered activities.






















































