The document details a gerontological assessment of a 68-year-old woman, focusing on her health status and recommendations for optimal aging. Despite being generally healthy and active, the assessment noted areas such as weight management and exercise that require attention, along with the importance of having an advanced directive. The subject has a positive outlook on life and is keenly aware of societal attitudes towards older adults.



![References:
Barker, L. R., Burton, J. R., Zieve, P. D., & Fiebach, N. H.
(2007). Barker, Burton, and Zieve's
principles of ambulatory medicine. [electronic resource].
Philadelphia, PA: Lippincott Williams & Wilkins, c2007.
Katz Index of Independence in Activities of Daily Living
(ADL). (2007). Urologic
Nursing, 27(1), 93-94.
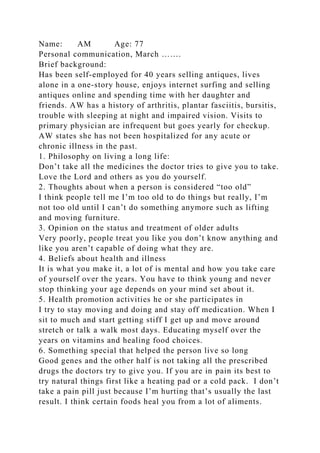
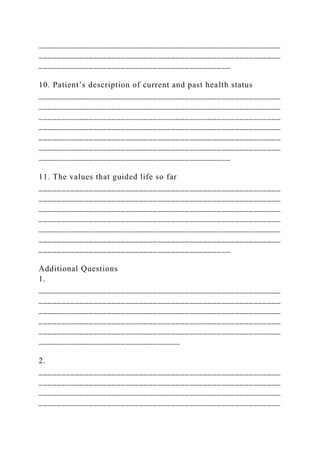
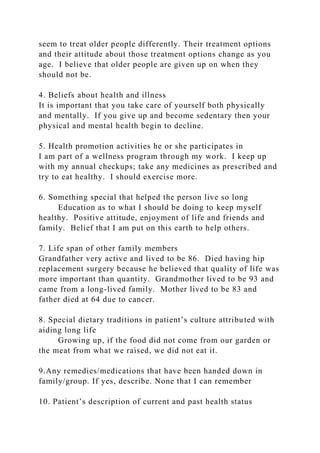
15. TRUNK Marked sway or uses walking aid 0
No sway – but flexion of knees or back,
or spreads arms out while walking
1
No sway, no flexion, no use of arms, and
no use of walking aid
2 2
16. WALKING STANCE Heels apart 0
Heels almost touching while walking 1 1
SCORE – GAIT 13
SCORE – BALANCE 15
SCORE – BALANCE AND GAIT 29
Rate 1 Rate 2 Rate 3
Date of Assessment Assessor Signature and Title Location of
Subject During Assessment
1.Jan 01, 2018 Paige Shinn Home
2
3
TINETTI ASSESSMENT TOOL: BALANCE
Subject’s Name: Pam Browning
Initial Instructions: Subject is seated in a hard, armless chair.
The following maneuvers are tested.](https://image.slidesharecdn.com/runninghead9assessingandplanningcareformyel-230123041416-718cacfa/85/Running-Head-9Assessing-and-Planning-Care-for-My-El-docx-8-320.jpg)



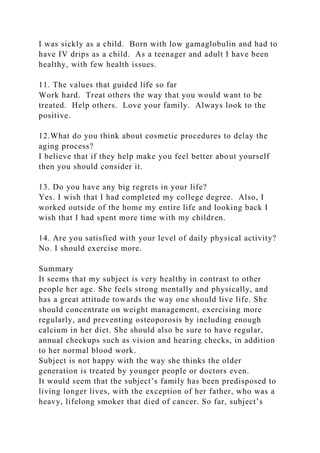
![Straight without walking aid 2 2
Running head: Functional Assessment
[Shortened Title up to 50 Characters] 19
Assessing the Functional Elements of the Older Adult
South University
Assessing the Functional Elements of the Older Adult
Completing a comprehensive assessment of an adult over 65 is a
way for the nurse to identify any issues that need attention and
help the patient have the best quality of life possible. The
purpose of the screening is to provide care, preempt disease,
retain good health, keep a record of health, minimize
disabilities, and give a holistic approach to independent living
(lecture online,wk.2). Various tools can be used to assess the
patient for the functional ability during an assessment. I will
use nursing tools that are applicable to the interviewed subject
and analyze where potential problem areas are. After analyzing
the information gathered, I will then connect the dots with
formulating interventions for the problems identified. I will be
discussing a 77-year-old female, AW, who lives independently
at home alone. The Patient interview
To ensure privacy of the person being discussed, I will refer to
the interviewee as AW. AW lives alone in her single floor
home close to her daughter and granddaughter. For the past
seventy years she has had very few medical issues which
include, arthritis, vision impairment, bursitis and plantar
fasciitis (personal conversation, Appendix A) AW’s view on life
is holistic and autonomous. AW has a good sense of control of
her medical problems and indicates that she is “in good health”.
AW agreed to a comprehensive assessment and each tool used
was explained to her in detail. I believe her cognitive status was
intact to understand and consent to this project. I will first](https://image.slidesharecdn.com/runninghead9assessingandplanningcareformyel-230123041416-718cacfa/85/Running-Head-9Assessing-and-Planning-Care-for-My-El-docx-12-320.jpg)




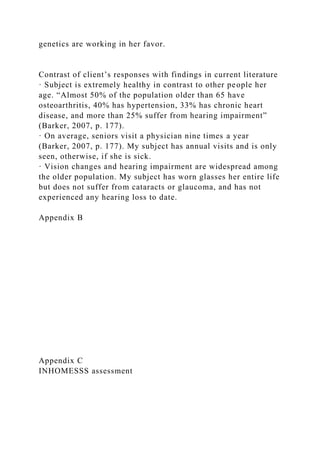
![After completing the functional assessment there was no need
for a true mental assessment for AW. Her ability to answer,
recall information and perform all tasks independently were
sufficient for a mental assessment and no deficits were noted.
Using all the tools discussed and her interview, I was able to
formulate problem areas with interventions. After reviewing
age related changes that pertained to AW I have recognized four
problem areas of health and living well. From the problems
noted, I applied nursing evidence based practice suggestions
and ideas, from literature read and experience as a nurse to give
at least three detailed interventions for each problem listed. The
importance of assessing older adults is to identify conditions
that affect not only health but level of functioning and quality
of life (Miller, 2015, p.99).
References
Internet Stroke Center. retreived from:
http://www.strokecenter.org
Miller, C. A. (2015). Nursing for wellness in older adults, (7th
ed). [Bookshelf Online]. Retrieved from
https://bookshelf.vitalsource.com/#/books/9781469895277/
Medscape.com. Retreived from: http://medscape.com.
Shelkey, M., Wallace, M., (2012). Katz index of independence
in activities of daily living. New York University College of
Nursing, I (2).
South University Online (2018). NSG4067: Gerontological
nursing: week 3: lecture 3. Retrieved from myeclassonline.com.
Appendix A
Patient Questionnaire by Chasidy Ward](https://image.slidesharecdn.com/runninghead9assessingandplanningcareformyel-230123041416-718cacfa/85/Running-Head-9Assessing-and-Planning-Care-for-My-El-docx-17-320.jpg)